Urethritis in men

Sexually transmitted infections
Men's health
Urethritis often results from a sexually transmitted infection, and doctors must consider treating partners as well as patients. Clinical features guide immediate treatment, but testing is important to confirm the treatment is correct.
Urethritis usually refers to urethral symptoms, often resulting from sexually transmitted infection (STI) of the male urethra. Before the era of sensitive nucleic acid amplification testing (NAAT), urethritis was often diagnosed by finding neutrophil polymorphs on a Gram-stained urethral smear. This is an insensitive test for the presence of infection and has been superseded by NAAT.1
Urethritis is often obvious, but it can be subtle and a urinary tract infection may be suspected because the patient reports dysuria. Urethritis is usually divided into gonococcal urethritis and nongonococcal urethritis. Clinicians can usually distinguish between these after taking a brief sexual history and examining the patient, but microbiological tests are required to establish the aetiology.
Causes
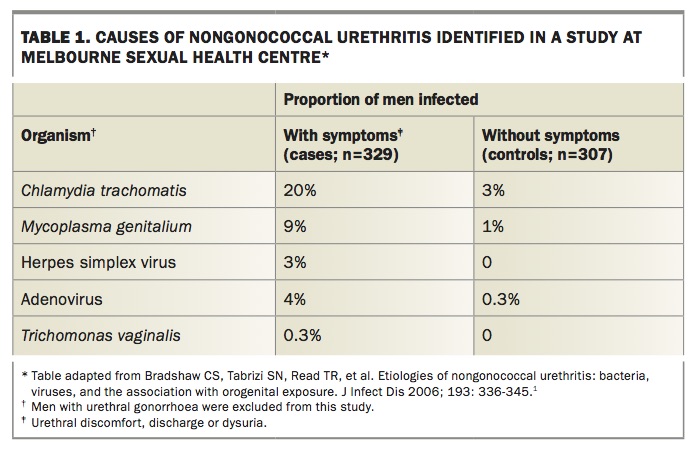
In Australia, Neisseria gonorrhoeae is a common cause of urethritis among men who have sex with men (MSM) and among Indigenous men, and is less common in other groups. Table 1 lists causes of nongonococcal urethritis identified in a study at Melbourne Sexual Health Centre (MSHC) in 2006.1 Men with gonorrhoea were excluded from this group of men who presented with urethral symptoms. Chlamydia trachomatis was detected in 20% of cases, Mycoplasma genitalium in 9% and herpes simplex virus or adenovirus were detected in 7%. No aetiological agent was found in the other 64%.
{kind=link}
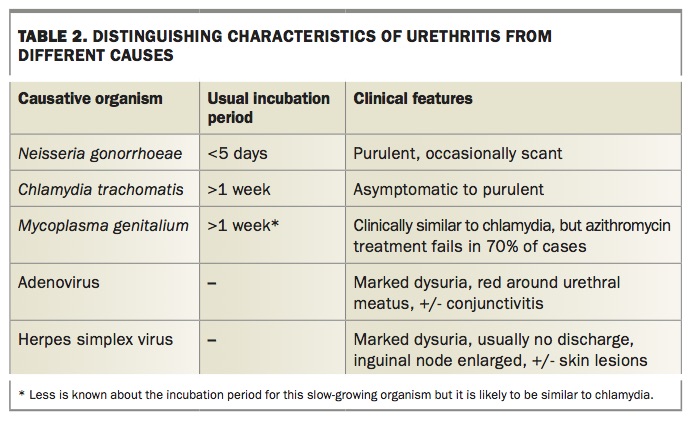
Useful clinical features that help to distinguish common causes of urethritis are listed in Table 2. Gonorrhoea is usually purulent and presents within a day or two of infection. Urethral chlamydia infection is frequently asymptomatic and chlamydial urethritis is often mild; however, mild or asymptomatic urethral gonorrhoea and purulent urethral chlamydia can occur. M. genitalium infection is less common but very similar in its presentation to C. trachomatis infection.
{kind=link}
Men with viral urethritis usually have marked dysuria, with or without a nonpurulent discharge, and often a bright red patch of skin surrounding the urethral meatus. Conjunctivitis is also a common feature of adenoviral urethritis.2 Urethritis is a common feature of initial attacks of genital herpes and causes the dysuria that often accompanies herpes lesions. Much less commonly, herpes simplex virus infection can present as urethritis alone.3
In a man with a male partner, a purulent urethral discharge is very likely to be urethral gonorrhoea (Box 1). Perimeatal erythema may indicate nongonococcal urethritis, due to infection with C. trachomatis, M. genitalium or a virus (Box 2). However, each can masquerade as the other. Although treatment is often started on the day of presentation, tests are required to ensure the treatment was correct.
{kind=link}
{kind=link}
Investigations
If a patient has a urethral discharge, collect some on a swab and send it for microscopy and gonococcal culture. There is no need to swab a dry urethra. If taking a swab, collect it before the patient urinates.
Collect the first 15 to 20mL of urine (‘first pass’ or ‘first void’) and request NAAT for N. gonorrhoeae, C. trachomatis and, if available, M. genitalium. Gonococcal NAAT is much more sensitive than culture, but culture provides information on gonococcal antibiotic sensitivities. If you need to diagnose or exclude gonorrhoea urgently, microscopy of the urethral smear can be performed quickly and the result communicated by telephone. Tests for Ureaplasma urealyticum or Mycoplasma hominis are very unhelpful as these are common commensal organisms.
Treatment
Before treating the patient, consider who else needs treatment for this infection. You may learn more by asking who your patient has had sex with, before you discuss the treatment plan.
In most cases of urethritis, patients are keen for treatment and it is generally recommended to treat immediately, without waiting for test results. The clinical features of either gonococcal or nongonococcal urethritis may be obvious and can be used to guide treatment. If there is any doubt, use the regimen for gonorrhoea because it includes azithromycin, which is also active against chlamydia. Further treatment will be required if M. genitalium is detected. If gonorrhoea appears unlikely, treat for nongonococcal urethritis with doxycycline and add to this if N. gonorrhoeae or M. genitalium are detected. Treatments are summarised in Table 3.4 Treatment guidelines are available online at www.sti.guidelines.org.au and at www.mshc.org.au.
{kind=link}
Eric (Box 1) is likely to have gonorrhoea, but may possibly have chlamydia or both infections. He should be treated for gonorrhoea with ceftriaxone (active against gonorrhoea alone) and azithromycin (active against chlamydia and many gonococcal isolates).
Tony (Box 2) appears to have nongonococcal urethritis, so treating him for chlamydia alone with doxycycline 100mg twice daily is sufficient, pending test results.
In patients with nongonococcal urethritis who are MSM consider adding ceftriaxone, particularly if it is impractical to review with test results. In very mild cases, where the question is whether there is an infection at all, treatment can be delayed until results are available. As Table 1 shows, most cases of urethral symptoms do not have an identifiable pathogen.5
Owing to increasing concerns about macrolide resistance, both the UK and European guidelines have recently switched to recommending doxycycline (100mg twice daily) as first-line therapy rather than azithromycin for nongonococcal urethritis.6,7 The Australian national guidelines are about to follow suit. Azithromycin resistance is now present in more than half of cases of M. genitalium infection in Melbourne, and azithromycin treatment fails and results in azithromycin resistance in at least 10% of initially susceptible cases.8,9 Doxycycline is also ineffective in most M. genitalium cases, but does not seem to generate further resistance.10 This underscores the importance of testing for M. genitalium.
Treating Mycoplasma genitalium
Some laboratories offer combined diagnostic resistance assays for M. genitalium, which allow treatment to be chosen based on the macrolide resistance profile. The widespread use of azithromycin for STIs may have led to increasing macrolide resistance in gonorrhoea and syphilis, in addition to M. genitalium.
At MSHC, we have now replaced doxycycline with azithromycin for treatment of nongonococcal urethritis for this reason, and because there is evidence that initial treatment with doxycycline increases the likelihood of a second antibiotic curing M. genitalium.11 Patients with M. genitalium should be recalled while still on doxycycline and prescribed a second antibiotic chosen according to whether the M. genitalium is macrolide sensitive or resistant.
Some polymerase chain reaction tests also detect a resistance mutation. If this is not available, resistance can be assumed in cases where azithromycin has already failed and in MSM (80% of whom had resistant infections in a Melbourne study).12 If M. genitalium is known or suspected to be macrolide resistant, patients should be prescribed moxifloxacin 400mg daily for seven days. Moxifloxacin is expensive, is not approved by the Therapeutic Goods Administration for this indication and is associated with serious but uncommon side effects including tendinopathy.13 In cases known or suspected to be macrolide susceptible then azithromycin can be prescribed directly after doxycycline. MSHC has evaluated treatment with 2.5g azithromycin (after doxycycline), given as 1g immediately followed by 500mg daily for three days, and this regimen cured more than 90% of infections.11 However, it is uncertain whether the higher dose of azithromycin is necessary after pretreatment with doxycycline.
In all patients, ensure a test of cure is performed at least three weeks after starting the second, more effective, antibiotic. If azithromycin was used to treat the urethritis rather than doxycycline, and the symptoms have improved, then wait for the test-of-cure result before treating further.
Partners
Sexually transmitted bacteria are highly infectious, especially N. gonorrhoeae. Condoms are protective, but testing is still recommended. Pharyngeal and anal gonorrhoea and anal chlamydia are common.
Sexual contacts should be offered treatment and testing for whatever is infecting your patient. Patients may be reluctant to contact some partners and can do this anonymously via www.letthemknow.org.au, which will send an anonymous SMS advising of the need for treatment. There is evidence that female partners of men with nongonococcal urethritis are at increased risk of pelvic or genital symptoms, even when no pathogen is detected in the index case, so it may be worth discussing antibiotic treatment with these women.14 Always consider testing for other STIs and remember that HIV and syphilis serology may be negative for a month after infection.4 Anal and throat swabs for N. gonorrhoeae and C. trachomatis are recommended for MSM.
Managing urethral symptoms that persist or return
Possible reasons for persistent urethral symptoms are outlined in the Flowchart. Reinfection is common, and patients should be asked about any sex since treatment, particularly with an untreated partner.
Less common pathogens should be considered. Cory (Box 3) should certainly be tested for M. genitalium. Trichomonas vaginalis can cause urethritis and is more common in parts of the world with poor access to health care.5 Treatment failure due to resistance is common with M. genitalium infection and should always be considered for N. gonorrhoeae; however, tests for the latter were negative in Cory’s case. Cory’s symptoms have probably lasted too long to be attributed to viral urethritis. Most cases of pathogen-negative urethritis improve within a few weeks. It is possible that Cory initially had a bacterial urethritis that was successfully treated, but he is suffering from the symptoms that can grumble intermittently for many weeks in some patients. Cory’s symptoms are not typical of urethritis and may be amplified by anxiety. Careful enquiry may be more helpful than repeating negative tests and prescribing more antibiotics.
{kind=link}
Conclusion
Men with urethral symptoms need to be tested for N. gonorrhoeae, C. trachomatis and M. genitalium. It is important to treat without delay and cover gonorrhoea if the discharge is purulent. Further treatment should be added if necessitated by the test results. Tests for other STIs such as syphilis (Table 3), and testing and treating the patient’s contacts must not be neglected. MT
Acknowledgement
Tim Read is supported by NHMRC Early Career Fellowship 1091536.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.