Opioid prescribing: what do the 2020 PBS changes mean for GPs?
On 1 June 2020, TGA and consequent PBS changes to reduce prescription opioid-related harm came into effect. They include changed PBS categories and clinical criteria, and smaller pack sizes for opioids. The implications for GPs prescribing opioids and managing patients with severe pain are illustrated by case studies.
Important update: further opioid prescribing changes
On 1 October 2020, further PBS changes that impact on opioid prescribing were announced. These included clarification of the requirements for secondary review of opioid use, particularly for palliative care patients, and for recording of the second prescriber review. The article has been updated to include these changes. The updated article is available here.
- On 1 June 2020, TGA regulatory and PBS changes that affect opioid prescribing came into effect.
- The changes include smaller pack sizes to limit unused medications for severe acute pain and re-defined indications for immediate- and modified-release formulations and higher potency opioids.
- The changes aim to minimise harms associated with prescribed opioids in line with current evidence and best practice.
- Evidence supports managing chronic noncancer pain with multimodal strategies, with function an important measure of efficacy.
- The use of opioids in the management of cancer pain and palliation and end-of-life care is unaffected by the TGA and PBS changes.
Opioids can be highly effective in managing pain but carry risk. The TGA regulatory changes and consequent changes to the PBS schedule for prescription opioids that came into effect on 1 June 2020 were a surprise to many prescribers. The changes are intended to support prescribers, improve patient safety, ensure safer treatment of acute severe pain and facilitate judicious, evidence-based advice on use of opioids for chronic noncancer pain, without impeding appropriate management of chronic severe cancer pain and end-of-life and palliative care. The changes acknowledge the unique presentation of each patient and recognise that treating doctors are in the best position to work collaboratively with their patients and other providers to make treatment decisions.
This article explains the TGA and PBS changes that impact on opioid prescribing and came into effect on 1 June 2020. Case studies illustrate the implications of the changes for GPs prescribing opioids and managing patients with severe pain.
Benefits of opioids
Opioids are considered to be essential medicines.1 They are acknowledged by the TGA to have an established role in pain management.2 The use of opioids to treat acute severe pain and for palliative care has never been questioned, and a small group of patients may benefit from long-term use for chronic noncancer pain.3 However, it is now understood that opioids are of limited benefit for most patients with chronic noncancer pain.4 Opioids are best used for a brief period for acute severe pain, for palliative care and for selected individuals with chronic severe noncancer pain.3
Risks of opioid prescribing
Australia has seen a rapid increase in use of prescribed opioids. Between 1990 and 2014, there was a fourfold increase in dispensing of opioids.5 In 2016-17, one or more prescriptions for opioids (mostly oxycodone) were dispensed to 3.1 million people, or 13% of the Australian population. Over the same period, 1.5% of the population were taking opioids on a daily basis.
For many patients, opioids are appropriate and relieve pain, reduce suffering, and improve function and quality of life. However, with potential good comes potential harm; in Australia, three people die of opioid overdose and 150 are hospitalised with nonfatal poisoning or overdose every day.6 Pharmaceutical opioids were considered a significant contributing factor in 70% of the deaths.7 In patients prescribed opioids for acute pain, the risk of progressing to long-term use starts to rise within days of commencing the opioid.8
For many people, long-term use of prescribed opioids for chronic severe noncancer pain is inappropriate, with no improvement in function or reduction in pain.9 Common adverse outcomes of opioids include hyperalgesia, endocrine abnormalities, falls and fractures. Aberrant medication behaviours, dependence, addiction and on-selling or sharing of medications are common.10-14 The risks increase the longer a person takes opioids and as dose increases.15,16 The adverse effects and aberrant behaviours affecting families, communities and the health system should not be underestimated.17,18 Furthermore, notwithstanding the evidence of opioid-related harms, recent evidence shows that opioids lack efficacy in chronic noncancer pain and do not improve function.9
History of the TGA and PBS changes
Concerns have been increasing about the risks associated with prescription opioid use in Australia for over 20 years, leading to progressive policy changes.5 In 2017, the TGA proposed additional changes and publicly sought comment from interested parties. The TGA received 98 submissions, all broadly supporting the proposed changes.
In 2019, the Chief Medical Officer wrote to the 5000 top opioid prescribers in Australia. This application of ‘nudge theory’ was intended to encourage prescribers to review their practice. However, it was interpreted by some as ‘heavy handed and intimidating’.19,20 Some doctors suddenly ceased opioid treatment for some patients, many without planned management, leading to suffering and anguish.
To counterbalance this and encourage evidence-based pain management, several education programs were rolled out through the National Prescribing Service (NPS), Royal Australian College of General Practitioners (RACGP) and Faculty of Pain Medicine of the Australian and New Zealand College of Anaesthetists (FPM ANZCA).
In December 2019, the Pharmaceutical Benefits Advisory Committee (PBAC) recommended the PBS changes suggested by the TGA. These were made public in early 2020 and were rolled out in June 2020. However, not all prescribers were aware of the changes, resulting in frustration for themselves and their patients.
What are the June 2020 changes?
The TGA and PBS changes seek to decrease harm while maintaining patient access to affordable opioid treatment. The changes introduced on 1 June 2020 include:
- introduction of smaller pack sizes (in addition to those currently available)
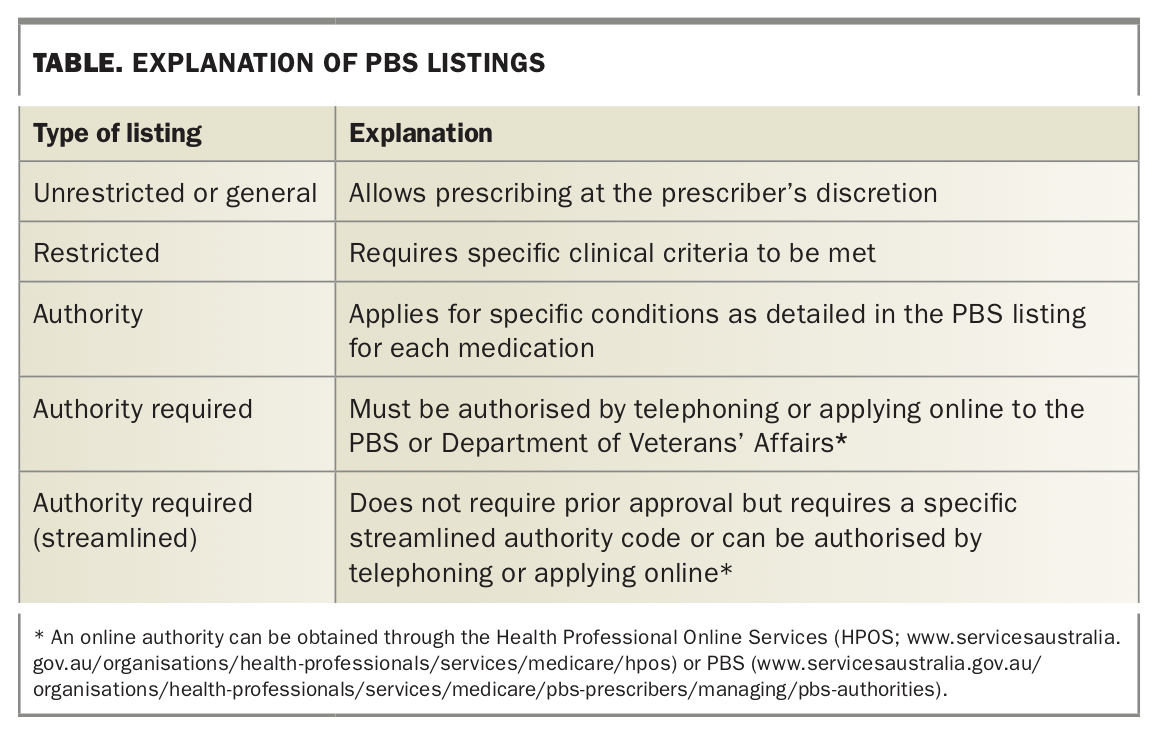
- changes in PBS categories – all opioids are now listed as either restricted or authority under the PBS (Table)
- new additional listing for codeine 30 mg for cough suppression with a restricted benefit for 20 tablets
- amended clinical criteria, with clinical indications classified into three groups – acute severe pain, chronic severe pain (cancer and noncancer pain), and cough suppression – with re-defined criteria for each
- stipulation not to use high-potency opioids in opioid-naïve patients
- changes to label warnings and consumer medicines information (CMI) documents.
{kind=link}
The TGA is working with stakeholders to raise awareness about these changes and also about the importance of nonopioid alternatives and safe disposal of unused opioids.
Opioid medicines are classified based on their time to onset and duration of activity and potency:
- immediate release (IR) opioids – buprenorphine, codeine, codeine and paracetamol, morphine IR, oxycodone IR, tapentadol IR and tramadol IR
- modified release (MR) opioids (MR and slow release [SR] formulations are now both listed under MR) – buprenorphine (transdermal patches), morphine MR or SR, oxycodone MR, oxycodone MR with naloxone, tapentadol SR and tramadol SR
- potent opioids – hydromorphone MR, methadone and fentanyl (transdermal).
Opioid prescribing changes in detail
All opioids for the treatment of severe pain are now listed under the PBS as either restricted or authority required. The re-defined criteria and PBS listings for opioid prescribing and other changes are detailed below, with cases illustrating their application in general practice.
Restricted benefit for IR opioids
The category of restricted benefit IR opioids has specific clinical indications:
- nonopioid options (pharmacological and nonpharmacological) have not adequately managed the pain
- the pain is considered severe enough to warrant treatment with opioids
- the person cannot use nonopioid medications because of contraindications, adverse effects or intolerance.
For prescription of high-potency IR opioids (e.g. oral hydromorphone), patients must meet the above clinical criteria and also the below criterion:
- other opioids have not adequately treated the pain and the person is not opioid naïve (i.e. must be already taking opioids and be tolerant to their effects).
The TGA also flags that IR opioids are generally not appropriate for the treatment of chronic severe pain.
New smaller IR opioid pack sizes with restricted benefit for short-term acute severe pain
The smaller pack sizes (10 tablets) of IR opioids (codeine, codeine and paracetamol, oxycodone, tapentadol IR and tramadol IR) are for the treatment of acute severe pain not responding to nonopioid analgesia and simple nonpharmacological care. IR opioids prescribed under these listings cannot include repeats or increased quantities.
Evidence indicates that many people do not need large quantities of tablets to manage short-lasting acute severe pain.21 The smaller pack sizes limit wastage and ‘stockpiling’ in people’s homes, reducing medication sharing and inappropriate use. They also send a clear message that use is expected to be only short term (e.g. for postoperative pain), and encourages people to return to their medical practitioner for review if their condition does not improve.
Case study 1. Small pack size for acute severe pain
Jack, aged 35 years, attends your surgery with severe acute pain after a knee arthroscopy. He has tried paracetamol and anti-inflammatories, but these have offered little relief. You provide a prescription for a low-dose opioid in the smallest pack size (10 tablets). You discuss the risks of the opioid medication. Three days later, Jack returns for review. He reports he needed only eight of the tablets because the pain settled quickly. He is seeing his surgeon for review the following day. He takes the unused tablets to the pharmacy for safe disposal.
Full pack size with restricted benefit for IR opioids for treatment of acute severe pain
The full pack size (20 tablets) of IR opioids will continue to be available for patients where the prescriber considers that a larger pack will be needed for the treatment of acute severe pain. MR opioids are not recommended for the treatment of acute severe pain.
Case study 2. Larger pack size for acute severe pain
Jill, aged 40 years, attends your practice. You note her standing awkwardly in the waiting room, and she walks slowly and carefully into your surgery. She says she has hurt her back. ‘I was playing with the kids and suddenly got this terrible pain in my lower back. I didn’t sleep last night and I can hardly move.’ Paracetamol and ibuprofen are ineffective.
There are no red flags, and you diagnose a possible acute disc tear or prolapse and explain that the symptoms will most likely resolve with conservative management. You prescribe paracetamol and an IR opioid using the standard pack size (20 tablets), as you consider she is likely to need this quantity. You encourage her to see a physiotherapist and to ‘keep moving’.
You follow her up weekly. Her symptoms slowly improve, and by week 4 she is almost free of pain. She takes the opioid at night to help her sleep for the first two weeks but does not need it any longer.
Opioids for cancer pain and palliative and end-of-life care
There is good evidence supporting the use of opioids for cancer pain and palliative and end-of-life care. The PBS listings have been brought into line with opioids for other indications, and they are now either restricted or authority (streamlined). ‘Pain directly attributable to cancer’ is an indication for opioid use. This is unchanged from previous listings. Both IR and MR formulations can be used for this indication.
Case study 3. Severe cancer-related pain
Julie, aged 52 years, has end-stage lung cancer. She is distressed by severe back pain caused by metastatic disease. You prescribe her authority (streamlined) MR opioids to reduce the pain and balance her distress against her desire to spend quality time with her husband and children. You review her regularly in consultation with the palliative care team.
Opioids for treatment of chronic noncancer pain
The recent PBS and TGA changes apply to the following MR formulations:
- buprenorphine (transdermal patches)
- morphine MR
- oxycodone and oxycodone with naloxone MR
- tapentadol MR
- tramadol MR.
- They also apply to second-line agents if the above opioids are ineffective and a more potent opioid is clinically indicated:
- fentanyl (transdermal patches)
- hydromorphone MR
- methadone (this is a potent opioid with complex pharmacology and should not be prescribed for pain without specialist advice).
All the above formulations have been moved from the restricted category to the authority (streamlined) category under the PBS. The authority (streamlined) category requires an authority prescription with a streamlined authority code or a telephone or online authority obtained through the Health Professional Online Services (HPOS), PBS or Department of Veterans’ Affairs (e.g. https://www.servicesaustralia.gov.au/organisations/health-professionals/services/medicare/pbs-prescribers/managing/pbs-authorities).
As in the case of opioids prescribed for acute severe pain, opioids prescribed for chronic severe pain are funded through the PBS only for specific indications. The criteria are:
- the pain must be continuous and daily and due to cancer (see case study 3, above), or
- the pain must be continuous and daily, and the patient has experienced inadequate pain management taking the maximum recommended doses of nonopioids, or
- the person cannot use nonopioids because of contraindications, adverse effects or intolerance.
In addition, fentanyl, methadone or hydromorphone should not be prescribed to an opioid-naïve person (i.e. a person who has not been trialled on other opioids and has no tolerance). Before prescribing, the patient’s presentation is best discussed with a pain or palliative medicine specialist.
MR opioids are generally not appropriate for breakthrough or as-needed pain relief for chronic noncancer pain.2
Management of chronic severe noncancer pain
The TGA notes that the management of chronic noncancer pain is complex and that this pain responds better to a multimodal or multidisciplinary approach. There is good evidence that nonpharmacological treatments, including active self-management, education, cognitive therapies, counselling and physical activity, have a role for every patient with chronic noncancer pain, and many will obtain similar benefit from nonopioid medications.4 Opioids are best used in the context of multidisciplinary, nonpharmacological pain management and only added if clinically necessary where the benefit outweighs the risk.9,11 This may be difficult for some prescribers and patients with limited access to multidisciplinary care, for example in rural areas.
The TGA states that ‘modified release opioids are not indicated to treat chronic non-cancer pain (other than in exceptional circumstances)’.2 The definition of ‘exceptional’ is interpreted by the FPM (a cross-disciplinary group of pain management clinicians within ANZCA) as:
‘severe pain, for which other treatment options have failed, are contraindicated, not tolerated or are otherwise inappropriate to provide sufficient management, and which has been shown to be opioid-responsive’.22
This approach flags the role of opioids in severe chronic noncancer pain and the recommendation to use them only in conjunction with other pain management strategies for conditions that show substantial improvement with the opioid (see case study 4, below).
Opioid use and reliance on opioid analgesia can often be reduced or avoided with nonpharmacological pain management strategies. Adjuvant therapies such as tricyclic antidepressants (amitriptyline and nortriptyline), serotonin and noradrenaline reuptake inhibitors (e.g. duloxetine and venlafaxine) and antineuropathic medications (e.g. gabapentin and pregabalin) may be useful for reducing opioid requirements. The focus of treatment is not complete pain relief but rather improved function and quality of life, and manageable pain. This should be discussed with the patient at treatment commencement, with the understanding that the opioid will not continue if these objectives are not met (see case study 5, below).
Case study 4. Chronic severe noncancer pain in exceptional circumstances
John, aged 38 years, has a history of severe neck pain due to injury and takes an oral opioid daily at an oral morphine equivalent daily dose (OMED) of 30 mg. He has no history of aberrant behaviour and no other current alcohol or other drug use. You have confirmed through available means in your state that you are his only prescriber and your prescriptions are dispensed from only one pharmacy.
At your regular reviews, he appears to be managing the neck pain well, his mood is good and he is working and providing good care as a single parent to two primary school-aged children, who you see often in the practice. He has regular physiotherapy and counselling. He has seen a pain specialist in the past, who supports the ongoing use of opioids for his condition. John says, ‘You know, the thing that helps the most is the counselling. It helps me manage my thinking and stops me overreacting when it feels like the pain is damaging my bones. I calm down, feel less scared, and this helps me manage with the pain.’
You regularly reassess John and confirm that his condition is opioid responsive. With counselling and active self-management, he continues taking the opioid, which is a small but important part of his management.
Case study 5. Chronic severe noncancer pain unresponsive to opioids
Jasmine, aged 29 years, sees you for lower back and hip pain following a motor vehicle accident nine months ago in which her pelvis and femur were fractured. She has been taking an opioid medication, but her pain is not adequately controlled. You explain the lack of response and together decide that it would be best to ‘taper and terminate’ the opioid medication. She slowly cuts down the dose of oral opioid, ceasing after eight months. She finds the process challenging, but with your support and counselling succeeds in ceasing. Notably, her pain improves without the opioid.
Second prescriber review
PBS restrictions on long-term opioid prescribing continue to require review of the patient’s treatment by another prescriber after 12 months of opioid treatment if increased maximum quantities or repeats are sought. This review must be within the past 12 months or within 15 months of commencement, with the reviewer’s name and date of review listed on the application. This encourages reassessment of current management, ensuring the patient is receiving the most appropriate pain management. It is not necessary for this review to be provided by a specialist; it is up to the prescriber to decide who would be most beneficial given the individual clinical presentation (see case studies 6 and 7).
The second prescriber review can help set boundaries, ensure patient safety and encourage a reluctant patient to reconsider treatment. It can also help put in place other harm reduction measures, such as intranasal naloxone to treat opioid overdose, staged supply, dose reduction, opioid rotation or medication-assisted treatment for opioid dependency (see case study 7).23-25
Case study 6. Second prescriber review – ongoing use appropriate
Jules, aged 70 years, has severe osteoarthritis of both knees. He is active, enjoys walking his dogs and cares for his frail wife aged 72 years. He has been using low-dose transdermal opioid patches for nine months and finds that they really help him ‘manage his day’. He takes no other analgesic medications and is on the waiting list for knee replacement.
You ask Jules to see your colleague, who is highly experienced in this management, for review, who agrees with your assessment of his opioid needs. You plan with Jules to continue prescribing the opioid until he has surgery and encourage him to continue walking and strength exercises.
Case study 7. Second prescriber review – opioid use not appropriate
Gretel, aged 48 years, is a long-term patient of your practice. She has anxiety, depression, asthma and chronic pelvic pain. She has been taking an oral opioid for some years, with the dose slowly increasing over that time. She still complains of severe pain and is often tearful and overwhelmed in the surgery.
You explain you are concerned about her opioid medication and risk, given her health issues, current opioid dose, and the fact that the treatment regimen is not working. You prescribe intranasal naloxone because you are concerned about her opioid overdose risk, arrange staged supply of her medication from her pharmacy and explain she needs to see a specialist for review.
Gretel is reluctant, but when you explain that to continue opioid treatment, she needs urgent review, she agrees. She is reviewed in a pain clinic, where alternative safer strategies are suggested to manage the pain, improve her quality of life and further reduce opioid harm.
Diagnosing and managing opioid use disorder
Long-term use of opioids increases the risk of opioid use disorder, which is best managed in a medication-assisted treatment for opioid dependence (MATOD) program.
Case study 8. Second prescriber review – opioid use disorder
Harry, aged 45 years, began taking opioids after surgery. He has struggled to stop this medication, experiencing nausea, abdominal discomfort, goose flesh, sweats, anxiety and an intense desire to take opioids. He has seen multiple doctors to obtain his medication and has increased to an OMED of 180 mg. He is worried about this use and says it has taken over his life.
You diagnose opioid use disorder and, in consultation with your local addiction service, Harry begins on a MATOD program. His symptoms settle and he is relieved to have his life back in control.
Opioids for cough suppression
Prescribing of codeine for cough suppression has been moved to its own listing with a restricted benefit. The change aims to clarify this indication and allow monitoring of codeine use for cough suppression.
Good practice in opioid prescribing
Prescribers are responsible for all prescriptions they write. Some Australian doctors have found themselves needing to justify their opioid prescribing to state and federal authorities whose role is ensuring compliance with legislation. To ensure compliance, ongoing assessment for treatment efficacy and risk is required. Recommended steps in opioid prescribing are summarised in the Box.24,25
The TGA has compiled a webpage of resources that links to consumer information and prescriber information, including guidelines and position statements from several sources (www.tga.gov.au/opioid-resources).
Conclusion
The June 2020 PBS and TGA changes align with current evidence on opioids. They seek to discourage inappropriate opioid prescribing and to reduce the prevalence of opioid-related harms, while ensuring patient access to essential treatment. They also acknowledge that prescribers are best placed to make clinical decisions collaboratively with their patients.
The TGA and PBS regulations support both prescribers and patients. They help ensure that safety and wellbeing are maintained and encourage prescribers to diligently implement best practice. MT