Long-acting depot buprenorphine: a new treatment option for opioid dependence

Long-acting depot buprenorphine is a new treatment option for opioid dependence that avoids the burden of daily dosing seen with sublingual buprenorphine while minimising risk of diversion. GPs need to be aware of potential treatment issues in their patients receiving this therapy.
Almost 50,000 people in Australia are currently receiving opioid pharmacotherapy for opioid dependence.1 When administered in accordance with best practice guidelines, opioid pharmacotherapy reduces mortality and morbidity and improves social functioning of people with opioid dependence. It is recommended by both professional and government authorities.
Opioid pharmacotherapy for opioid dependence has traditionally comprised two main options: oral methadone and sublingual buprenorphine, the latter taken either as a tablet or, combined with naloxone, as a film. The recent TGA approval of long-acting depot injectable buprenorphine provides a new treatment option for patients seeking help for opioid dependence. It has the potential to increase convenience while also reducing the risks of diversion.
At the time of writing, long-acting depot buprenorphine was licensed to treat opioid dependence only in specialist settings. Here we describe the available formulations of long-acting depot injectable buprenorphine and the clinical issues that GPs and other clinicians may encounter in their patients receiving these medications.
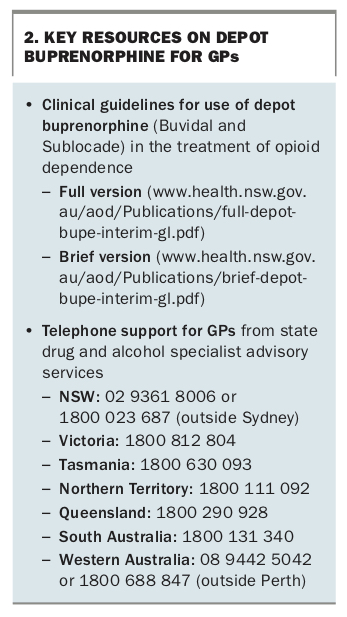
Many GPs currently prescribe sublingual buprenorphine to treat opioid dependence, and long-acting depot buprenorphine may become available for prescription by GPs in the future. Further information on prescribing depot buprenorphine can be found in the NSW Clinical guidelines for use of depot buprenorphine (Buvidal and Sublocade) in the treatment of opioid dependence (complete and brief versions).2,3 We recommend that GPs who wish to prescribe opioids for patients with opioid dependence attend the relevant opioid pharmacotherapy therapy training in their state to extend their prescribing authority. For example, in NSW, the Opioid Treatment Accreditation Course (OTAC) is available either face to face or online (https://otac.org.au).
Conventional buprenorphine formulations
Buprenorphine is known to be effective in treating people with opioid dependence and reducing the use of illicit and pharmaceutical opioids.4 However, patients can have difficulty engaging with and remaining in treatment with conventional buprenorphine formulations because of the requirement for daily dosing at a clinic or pharmacy. The provision of takeaway doses increases patient convenience but also the risk of diversion. It is a complex clinical decision based on the frequency of medical assessment, presence of ongoing drug use and potential for diversion.5 Long-acting injectable buprenorphine is a new treatment option that avoids the burden of daily dosing while minimising the risk of diversion.
Long-acting buprenorphine formulations
Two extended-release injectable formulations of buprenorphine are available in Australia: Buvidal (Camurus) and Sublocade (Indivior).
Buvidal is currently TGA-approved for ‘maintenance treatment of opioid dependence, within a framework of medical, social and psychological treatment’.6 Buvidal was PBS-listed in September 2019. It is available in weekly and monthly formulations at a range of strengths.
Sublocade was registered by the TGA in July 2019 and is available on a limited basis in Australia through a clinical trial. Sublocade is registered in the US and is likely to become more widely available in Australia in 2020. It has been favourably assessed by the Pharmaceutical Benefits Advisory Committee but is not currently PBS-listed. Sublocade is available for monthly administration at two different strengths, 300 mg and 100mg.
Commencing long-acting buprenorphine
Before commencement of any pharmaceutical therapy in patients with a substance use disorder, a detailed medical history is required. This should explore all recreational substances used by the patient and their pattern of use, medical comorbidities, medications, psychiatric history and social situation, so that treatment can be provided within a biopsychosocial framework. Support for housing, welfare and legal issues is crucial to provide stability for the patient. Clients should also be offered counselling and behavioural interventions, and recommended appropriate self-help groups, such as SMART Recovery Australia. Regular review is important not just to review the dose of medication but also to ensure appropriate psychological and social follow up.
When commencing opioid agonist treatment, patients also need to be advised of the risk of respiratory depression and sedation, especially if they continue to use other opioids outside those prescribed.
Buvidal and Sublocade differ in their dosing regimens.
Buvidal dosing
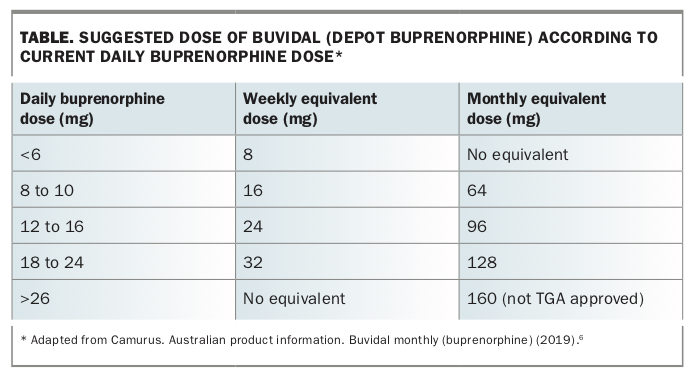
Buvidal is typically introduced after patients have been stabilised on sublingual buprenorphine for at least a week. It is first administered 24 hours after the last dose of buprenorphine. The suggested dosing regimen is based on the patient’s current daily buprenorphine dose (Table).6
{kind=link}
Buvidal is available in both weekly and monthly formulations. A recent study of patients transferring from sublingual buprenorphine to either weekly or monthly buprenorphine injections found no serious adverse events between the two.7 There are currently no clinical studies showing the superiority of either weekly or monthly dosing, and the choice is largely guided by patient preference. There is no monthly dosing equivalent for low daily buprenorphine doses (less than 6 mg), limiting the use of monthly injections in patients taking these doses.
Sublocade dosing
Recommendations on Sublocade administration are to start with loading doses of 300 mg monthly for the first two months, followed by 100mg monthly thereafter. However, patients taking low daily doses of buprenorphine can begin at a Sublocade dose of 100 mg. Some patients may require higher doses and can stay on the 300 mg dose for longer. There is no formulation of Sublocade for weekly administration. Sublocade appears to have a longer duration of action and achieve higher blood levels than Buvidal. There are no head-to-head trials directly comparing Sublocade and Buvidal.
Adverse events
All formulations of buprenorphine are known to cause respiratory depression.8,9 The product information advises caution using buprenorphine in patients with respiratory dysfunction caused by conditions such as chronic obstructive pulmonary disease, congestive heart failure or asthma. None of the clinical studies published so far on the injectable forms of buprenorphine has specifically assessed patients with these conditions.
A comparison of Buvidal with a placebo injection combined with sublingual buprenorphine found no significant difference in adverse events (see below).7 Adverse events seen in more than 5% of patients receiving Buvidal related to either the injection (site reaction and pain) or buprenorphine itself (headache, constipation and nausea).7
Sublocade at a dose of 100 mg or 300 mg was associated with a 5% or greater increase in absolute risk of constipation and upper respiratory tract infection than placebo.10 At a dose of 300 mg, it was also associated with a 5% increase in absolute risk of injection site reactions, although none were considered serious. The regimen of 300 mg doses followed by 100 mg doses had a 5% absolute risk increase in vomiting compared with placebo. Vomiting can be treated with a trial of an antiemetic such as metoclopramide.
Treatment issues
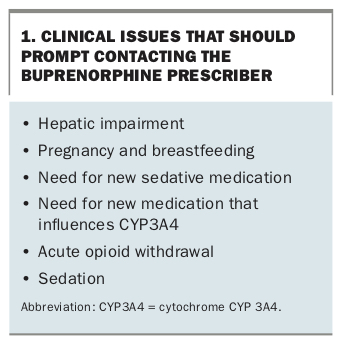
Medical issues related to the use of injectable buprenorphine should be managed by the prescribing doctor. However, nonprescribing GPs and other doctors may sometimes be the first to note a change in the patient’s condition that warrants discussion with the prescribing clinician (Box 1).
{kind=link}
Hepatic impairment
Buprenorphine is metabolised by the liver and is relatively contraindicated in patients with severe hepatic impairment or cirrhosis.5 Phase III studies of Buvidal and Sublocade excluded patients with liver function test results three times the upper limit of normal, or a serum bilirubin level 1.5 times the upper limit of normal.7,10 A change in hepatic function in a patient taking injectable buprenorphine should be discussed with the prescribing doctor as soon as possible, and the patient should be assessed regularly for signs of sedation.
Renal impairment
Renal impairment does not affect buprenorphine metabolism, and doses generally do not need to be modified. However, renal impairment can affect clearance of other medications leading to excessive sedation, so clinical monitoring is important if renal function deteriorates.
Pregnancy and breastfeeding
Patients who become pregnant while receiving injectable buprenorphine should discuss their treatment options with their prescribing doctor as soon as possible. Abruptly stopping opioid treatment runs the risk of opioid withdrawal or relapse, which both have potential complications for the fetus.11 Patients who become pregnant while receiving opioid substitution treatment should continue the treatment.
Although sublingual buprenorphine is considered safe to continue, there is a lack of safety data for injectable forms of buprenorphine. The decision to continue injectable buprenorphine requires discussion of the risks and benefits between the treating clinician and patient. Further, given the psychosocial complexities of substance use and pregnancy, we recommend referring pregnant patients to a specialist drugs-in-pregnancy service.
Breastfeeding is a complex issue for patients taking buprenorphine because of the lack of safety data and the proven benefits to the child of breastfeeding.6,11,12 Breastfeeding is listed as a contraindication to Buvidal in the product information. However, as in pregnancy, there is benefit in maintaining the mother on an opioid agonist for treatment of opioid dependence. Breastfeeding should be encouraged for any mother on an opioid treatment program. Clinicians may feel more comfortable prescribing standard forms of buprenorphine (i.e. tablets) while a mother breastfeeds. Where this is not possible, the risks and benefits of continuing depot buprenorphine should be discussed openly with the patient. Again, we recommend referral of postnatal patients to a specialist drugs-in-pregnancy service.
Opioid withdrawal
There is a risk of precipitated withdrawal when patients who have been using opioid agonists long term are transitioned to sublingual buprenorphine.5 This is due to buprenorphine’s high affinity for the opioid receptor, which leads it to displace other opioids such as heroin, coupled with its action as a partial agonist.13-16 Patients should therefore be stabilised on sublingual buprenorphine before initiation of injectable buprenorphine. This approach minimises the potential to precipitate opioid withdrawal. Any patient in precipitated withdrawal should be urgently discussed with the buprenorphine prescriber and referred to the nearest emergency department, unless the symptoms are trivial. Signs of opioid withdrawal include agitation, mydriasis, tachycardia, diaphoresis, vomiting, hypertension and piloerection.
Patients receiving depot buprenorphine may still develop withdrawal symptoms during treatment. If the patient reports these symptoms, clinicians should assess for signs of opioid withdrawal, although they are usually absent. For patients taking Buvidal, ‘top-up’ doses between regular injections are available. Supplemental dosing with sublingual buprenorphine is another option for patients receiving either depot formulation. More detailed recommendations are available in the NSW clinical guidelines for use of depot buprenorphine.2
Sedation
Although buprenorphine is known to cause sedation in opioid-naïve patients, it should not precipitate sedation in patients with opioid dependence.12 Sedation in a patient taking injectable buprenorphine may indicate use of other sedating agents, such as benzodiazepines, overestimation of the level of opioid dependence or a change in the patient’s drug metabolism, such as liver impairment. Clinicians should report to the buprenorphine prescriber if their patient appears overly sedated or has signs of harmful use of sedating drugs, such as alcohol, opioids or benzodiazepines. Care should also be taken when prescribing any sedative agents (see drug interactions). In general, coprescribing of psychoactive drugs should be avoided. If undertaken, it should be done in collaboration with the buprenorphine prescriber.
Pain management
Pain management is complex for patients taking buprenorphine, because of its potency and partial agonist action. Other opioid medications such as morphine and oxycodone have reduced efficacy in patients receiving buprenorphine. Pain management is beyond the scope of this article. However, like any other patients, people taking injectable buprenorphine who have acute pain should be assessed for the cause. A trial of nonopioid analgesics such as paracetamol and NSAIDs should be considered for those with mild-to-moderate pain. If these are inadequate then opioids can be trialled, but the patient is likely to require higher doses than an opioid-naïve patient because of tolerance. Furthermore, the treating clinician should have a plan for tapering the dose to avoid unnecessary escalation and risk of overdose.
Driving
Patients taking a stable dose of opioids are not considered at increased risk when driving provided there is no other problematic substance use.17 For patients starting buprenorphine treatment, the NSW guidelines state that plasma levels of buprenorphine accumulate for four doses of Buvidal and two (300/100 mg) and six (300/300 mg) doses with Sublocade.2 Patients should be advised not to drive until they have had at least this number of doses and have been reviewed by the prescribing clinician.
Drug interactions
Sedative drugs should be used with caution in all patients receiving opioid treatment, whether for opioid dependence or otherwise. This includes, but is not limited to, benzodiazepines, gabapentinoids (pregabalin and gabapentin), antipsychotics, tricyclic antidepressants and the ‘z-drugs’ zolpidem and zopiclone. It would be reasonable when prescribing any of these listed medications to discuss it with the buprenorphine prescriber first.
Buprenorphine can also cause drowsiness when combined with recreational drugs such as alcohol. Clinicians should familiarise patients with the Alcohol and Drug Foundation’s guidelines on alcohol and recommend avoidance during treatment initiation.18 Ongoing use of other opioids will also cause sedation and risk overdose and needs to be monitored at every review of every patient receiving buprenorphine treatment so that treatment can be tailored accordingly. Other problematic recreational substances for patients with opioid dependence include benzodiazepines and gabapentoids.19 Around 10 to 20% of patients in opioid treatment programs are either high-dose or erratic benzodiazepine users, placing them at risk of overdose and impaired cognition.5 Gabapentoids are increasingly being used to modify the effects of opioids, placing patients at risk of sedation and overdose. Clinicians should try to work with patients to control all recreational substance use as part of their wider biopsychosocial treatment.
Naltrexone is commonly used to treat alcohol dependence. However, because of its action as an opioid antagonist, it cannot be used concurrently with buprenorphine or any other opioid.
Buprenorphine is metabolised by cytochrome P450 3A4 (CYP3A4). It can therefore be affected by CYP3A4 inducers, such as carbamazepine, rifampicin and phenytoin, and CYP3A4 inhibitors, such as azole antifungals (ketoconazole) and protease inhibitors (e.g. ritonavir). In general, these interactions are not clinically significant because of the relatively flat dose–response curve for buprenorphine.
There is increasing evidence of a risk of serotonin toxicity in patients taking opioids, including buprenorphine, in conjunction with serotonergic drugs such as selective serotonin reuptake inhibitors (SSRIs, e.g. escitalopram), migraine therapy (e.g. sumatriptan) and tricyclic antidepressants (e.g. amitriptyline).20,21 The hallmarks of serotonin syndrome are fever, tachycardia, confusion and increased muscle tone. We recommend caution in prescribing serotonergic drugs for patients taking injectable buprenorphine and regular patient review.
Conclusion
The new long-acting depot formulations of buprenorphine provide another option for treatment of opioid dependence that may be more convenient for patients while minimising the risk of diversion. GPs are likely to encounter increasing numbers of patients receiving this treatment and can readily manage common issues that arise.In future, long-acting buprenorphine may become available for GPs to prescribe. Key resources for GPs managing patients receiving long-acting depot buprenorphine are summarised in Box 2. MT
{kind=link}