Obsessive compulsive disorder in children and adolescents

Dr Perkes is a Senior Lecturer in the School of Psychiatry, School of Women’s and Children’s Health and School of Psychology, UNSW, Sydney; and a Child and Adolescent Psychiatrist in the Department of Psychological Medicine, Sydney Children’s Hospital Network, Sydney.
Associate Professor Farrell is an Associate Professor in the School of Applied Psychology, Griffith University, Brisbane, Qld.
Dr Guy is a General Practitioner at East Brunswick Medical Centre, Melbourne, Vic.
Professor Eapen is a Professor in the School of Psychiatry, UNSW, Sydney; and Head of the Academic Unit of Child Psychiatry, Liverpool Hospital, Sydney, NSW.
Child mental health
GPs are uniquely placed to detect and begin management – including exposure and response prevention therapy – of obsessive compulsive disorder in young people, guided by validated self-report measures and with the aim of achieving sustained remission.
- It is estimated that one in 50 children or adolescents has obsessive compulsive disorder (OCD).
- Self-reported screening aids detection of OCD, and self-reported measurements of symptom severity enable treatment monitoring.
- Evidence-based treatments, especially the first-line treatment of exposure and response prevention (ERP), have large effect sizes.
- Family-based therapy may be needed to treat family accommodation of OCD symptoms (i.e. facilitating or participating in a child’s symptoms).
- Pharmacotherapy is typically indicated when symptoms persist despite the use of ERP.
- Sustained remission is the goal of treatment.
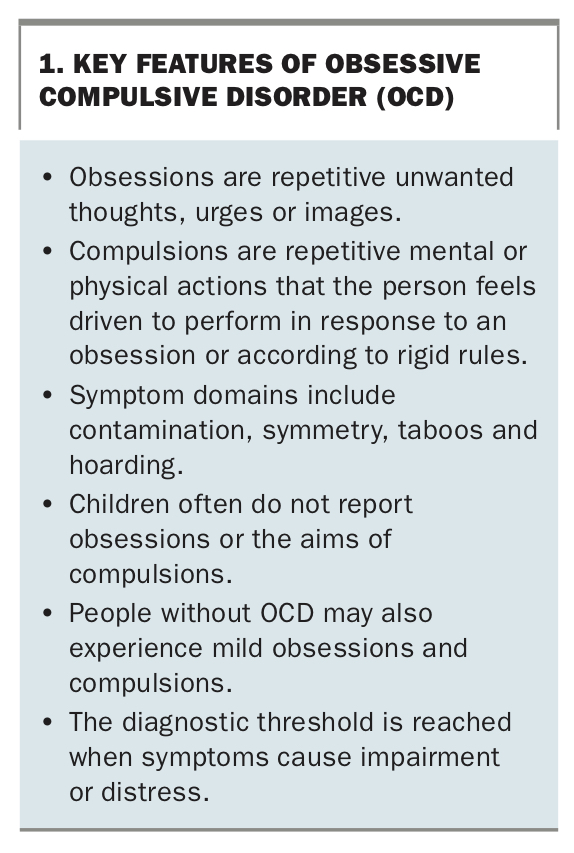
Obsessive compulsive disorder (OCD) is estimated to occur in one in 50 Australian children and is often chronic and impairing. The prevalence of 2 to 3% holds across the lifespan, with the illness remitting in some children while new cases emerge in adolescence.1 This pattern is reflected in the bimodal distribution of OCD, with peaks of onset around 11 and 18 years of age.1 OCD is characterised by obsessions (repetitive unwanted thoughts, urges or images) and compulsions (repetitive actions that the person feels driven to perform), either or both of which may be present (Box 1).
{kind=link}
As with other neurodevelopmental disorders, paediatric OCD often presents with comorbidities, such as attention deficit hyperactivity disorder (ADHD), and is more common in boys than girls.2 However, OCD in adults is reasonably equally distributed between the sexes.1 A subgroup of OCD with tics has a characteristically prepubertal onset in boys and is frequently associated with ADHD.3,4
OCD in children and adolescents often interrupts educational, social, emotional and cognitive development. It can also have a profound impact on home life, and family members may ‘accommodate’ OCD (by facilitating or participating in symptoms) with the good intention of alleviating distress. However, accommodation of OCD is associated with worsening of symptoms and poorer treatment response.5 Fortunately, family accommodation can be treated, and OCD treatment in general has one of the largest effect sizes in medicine.6
GPs are uniquely placed to aid with early detection and management of OCD in children and adolescents.
Assessment
Clinical presentation
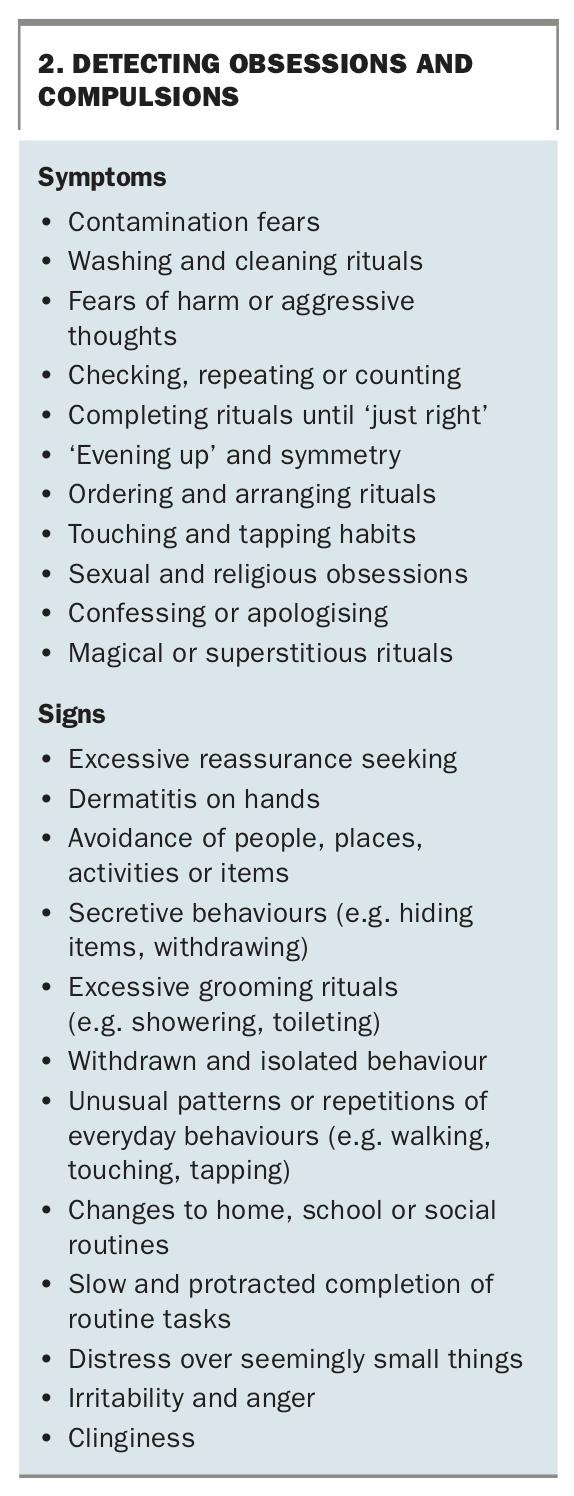
Young people with OCD present in various ways. However, they often do not voluntarily report their symptoms (Box 2). This secrecy is thought to arise from shame, confusion and acclimatisation in people with OCD. Combined with a lack of clinician confidence in assessment, symptom secrecy means that several years usually pass before OCD is detected. This often occurs when complications arise, such as a major depressive episode or school refusal. Owing to the prevalence of 2%, functional impairment and symptom secrecy, routine screening for OCD is indicated in children and adolescents presenting with emotional or behavioural distress. Increasing awareness among health and educational professionals, as well as parents, is therefore also crucial.
{kind=link}
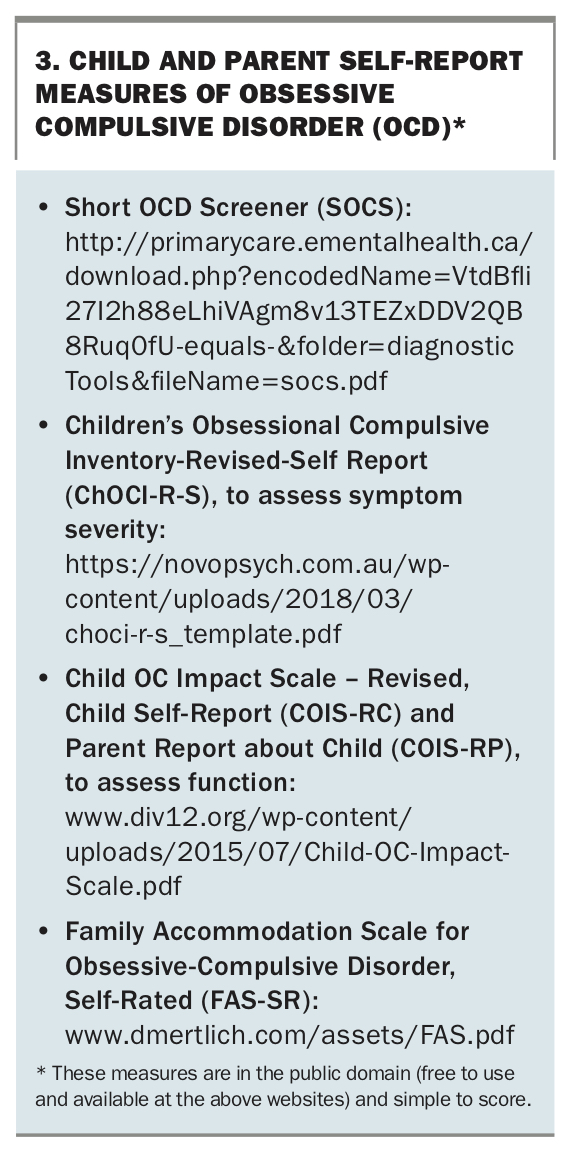
Validated self-report questionnaires are freely available and can be completed by children or parents to assess OCD symptoms between consultations (Box 3). This approach allows time for discussion of the results during a consultation and tailoring of specialist referrals to the child’s and the family’s needs (e.g. child-focused vs family treatment). Ongoing assessment with these measures enables monitoring of response to treatment, with the aim of sustained remission without relapse.
{kind=link}
Screening
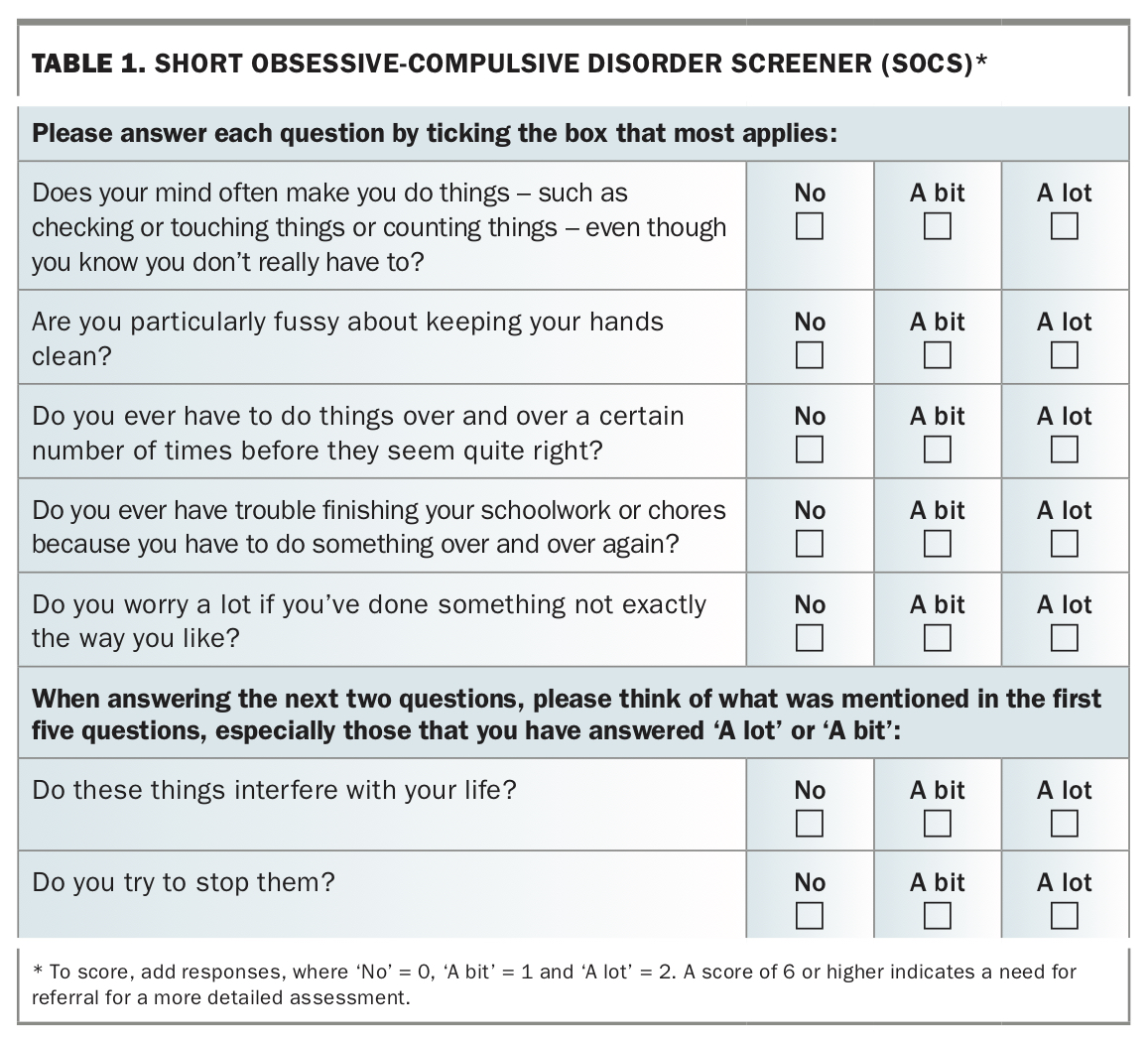
The Short Obsessive-Compulsive Disorder Screener (SOCS) is a seven-item self-report questionnaire validated for 9- to 19-year-olds (Table 1).7 Patients answer ‘no’ (0), ‘a bit’ (1) or ‘a lot’ (2) to five symptom-based and two impairment-based questions. The SOCS is scored by a simple sum, with a score of 6 or more indicating the need for referral for more detailed assessment (Box 3).
{kind=link}
Diagnosis
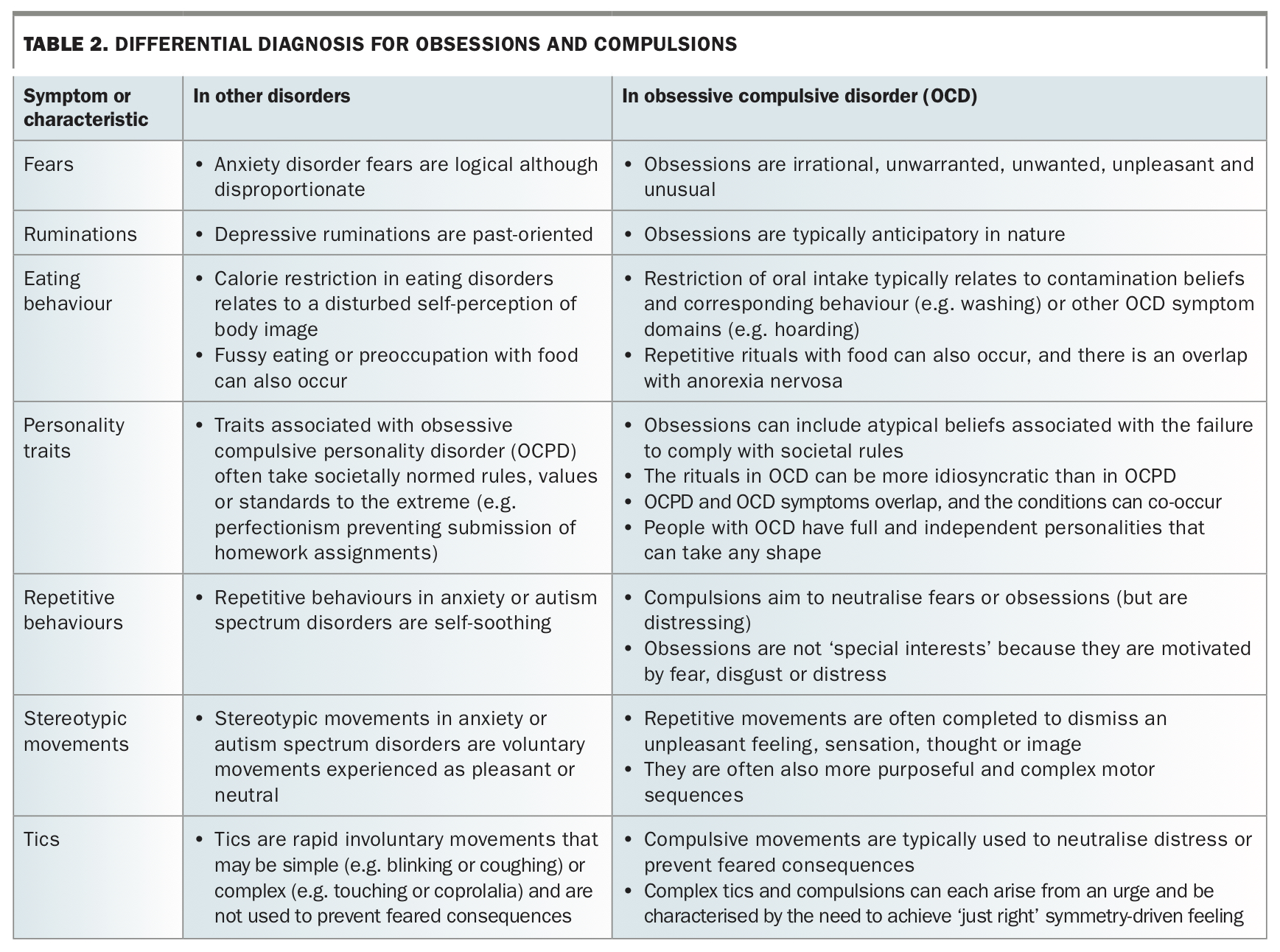
The diagnosis is made by clinical history and an examination to screen for symptoms (Box 2) aligning with the criteria (Box 1), while excluding differential diagnoses (Table 2). Creating time to listen to the young person and their family enables insight into their experiences, which is essential to differentiate symptoms. Asking a screening question before administering the SOCS can help to determine whether it is needed and normalise symptoms (e.g. ‘Lots of people do things, like counting or washing, or maybe think about things like pictures or numbers, over and over again even though it seems pretty silly and they don’t really want to. Has that ever happened to you?’). The patient should be offered the chance to talk without their parents in the room because children and adolescents are reluctant to disclose taboo symptoms (e.g. religious or sexual intrusions) in front of their parents. On the other hand, compulsions may be elicited from parents, who are able to observe these repetitive behaviours.
{kind=link}
OCD in childhood most often presents with both obsessions and compulsions. However, 40% of young people with OCD present with compulsions only, and a smaller proportion present with obsessions only.8 Assessment by a specialist clinician using a comprehensive semistructured interview schedule can elicit a higher-resolution definition of the illness.9
Severe and sudden-onset OCD preceded by an infection may herald paediatric acute-onset neuropsychiatric syndrome; in this rare instance, a specialist opinion should be sought.
Comorbidity
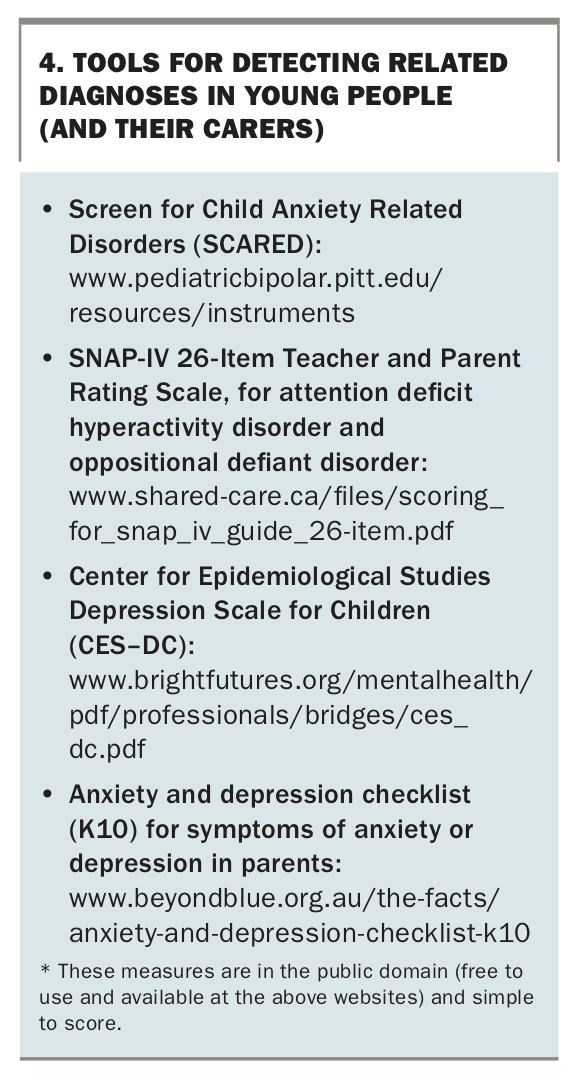
Comorbidities are common in children and adolescents with OCD and should be routinely screened for (Box 4). Genetically related neurodevelopmental disorders include ADHD and Tourette syndrome. Anxiety and depressive disorders, thought to be a psychosocial consequence, frequently accompany OCD. Oppositional defiant disorder and substance use disorders also commonly
co-occur and, as with other comorbidities, often require treatment to enable effective management of OCD.
{kind=link}
Family history
The risk of OCD is increased by having a first-degree relative with OCD, a tic disorder or ADHD.10 A family history of OCD also informs the psychosocial context for the patient (e.g. having a family member with OCD may compound symptom accommodation).
Management
Cognitive behavioural therapy
Cognitive behavioural therapy (CBT), including exposure and response prevention (ERP), should be offered to all young people with OCD because it is the only evidence-based nonpharmacological treatment. CBT shows large treatment effect sizes, low attrition rates and high rates of response (70%) and remission (53%).11 Components of CBT for OCD include psychoeducation, ‘externalising’ OCD, cognitive therapy strategies, ERP and relapse prevention. It is typically delivered in about 10 weekly face-to-face sessions of 60 minutes each, but there is emerging evidence supporting telephone, internet, group-based and intensive (e.g. daily) modes of therapy.12
Psychoeducation and externalising OCD are an initial and continuing part of CBT, with the goals of:
- assisting in understanding OCD as a medical condition, to destigmatise it, especially with regard to taboo (sexual, religious, violence) symptoms
- building rapport
- providing a rationale and enhancing motivation
- facilitating family ‘teamwork’
- describing how to do exposure within and between sessions
- warning of family accommodation of OCD.
Externalising OCD helps the family to work together against the illness by giving OCD a ‘nasty nickname’ to enable detachment from, and blame for, the symptoms. The family could develop a narrative to discuss and describe OCD, using the nickname to detect when OCD is ‘bossing’ the child around, as well as times when the child is in control of the OCD.
ERP – gradual exposure to feared stimuli without avoidance – is the active ingredient of CBT for OCD. ERP works by developing a symptom hierarchy and gradually exposing the child to the things that trigger their anxiety; this is done in incremental steps in a safe environment, assisted by the therapist. Despite its effectiveness, ERP is not widely implemented because of a lack of availability of trained therapists, funding barriers and low referrer awareness.
Family involvement is encouraged by a teamwork approach, with the child and family attending at least part of each therapy session together. The amount of family involvement in therapy, crucial in most cases, is often determined by the child’s age and the degree of accommodation. Family accommodation of OCD occurs in many forms; parents are taught to detect accommodation and helped to gradually reduce it, in collaboration with the child and therapist. Thus, having a support network – including GPs – trained in the rationale of therapy and delivery of exposure assists with therapy goals, including relapse prevention.
Pharmacotherapy
Persistent symptoms despite ERP are an indication for pharmacotherapy in children and adolescents with OCD. Illness severity is also a factor, and guidelines recommend the combination of ERP with pharmacotherapy as a first step in patients with severe to extreme OCD.13 However, a trial of ERP alone is often selected by parents and some doctors as first-line therapy, and this is reasonable in the context of symptom monitoring and with a review of progress at an agreed timepoint. The presence of a comorbid major depressive episode (common at initial clinical presentation) may tip the balance toward pharmacotherapy. Nonetheless, ERP should always be offered; the question is only whether and when pharmacotherapy should be used in combination with ERP. Financial and other equity issues that affect the availability of ERP are unfortunate and may be the real determinants of whether pharmacotherapy is offered.
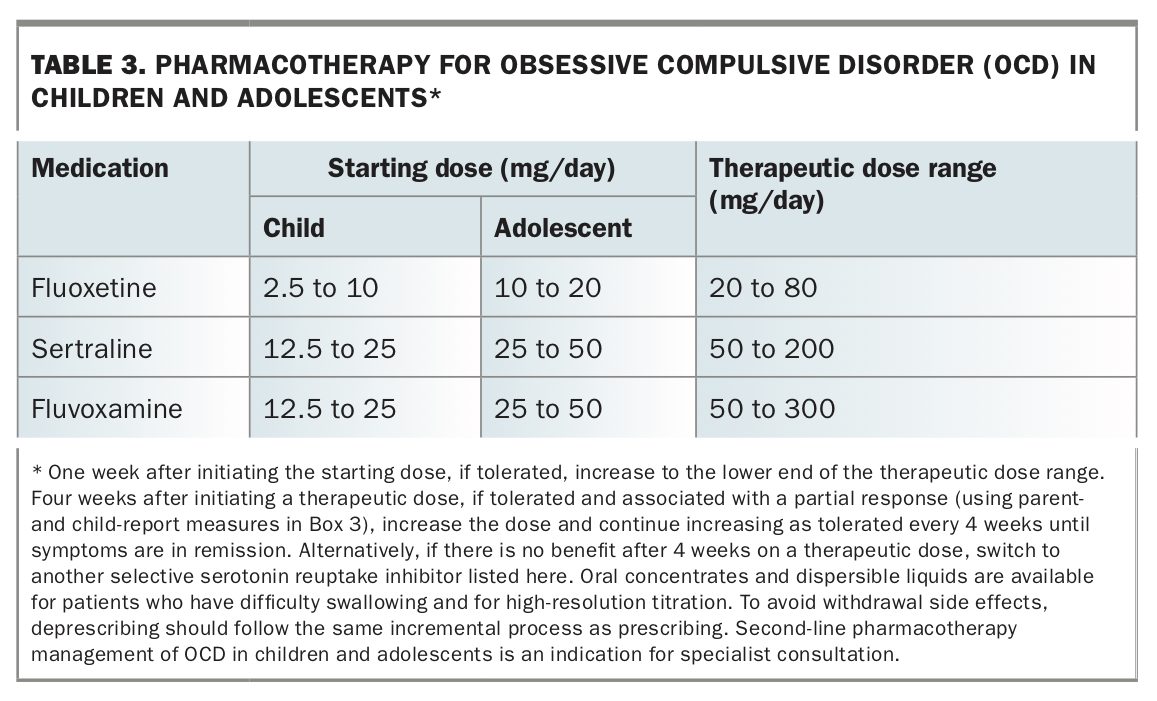
There are three selective serotonin reuptake inhibitors (SSRIs) that are clearly safe and effective for treatment of OCD in children and adolescents: fluoxetine, fluvoxamine and sertraline (Table 3).13,14 The clarity of evidence supporting these distinguishes pharmacotherapy for OCD from that for generalised, social and separation anxiety disorders in children, for which the evidence is more varied.14 Owing to its unique effectiveness in treating depression in children and adolescents, and because of the frequent co-occurrence of depression with OCD, fluoxetine stands out as a first-line pharmacotherapy for OCD.15 If there are pharmacokinetic interactions or intolerable side effects, another first-line SSRI should be recommended.
{kind=link}
Second-line pharmacotherapy (e.g. augmentation or substitution with clomipramine), if needed, is an indication for referral to a child and adolescent psychiatrist or other specialist with experience in using psychotropic medication. Paroxetine does show effectiveness for treating paediatric OCD but is not recommended because of its association with suicidal ideations and behaviour.15 Antipsychotic medication is supported by open-label trial evidence for treating paediatric OCD. However, with a high risk of cardiometabolic complications, careful monitoring is indicated, so it should not be commenced in general practice.16
Conclusion
OCD is common in children and adolescents, and years often pass before the condition is diagnosed and evidence-based treatment is offered. Fortunately, there are valid and reliable screening tools for OCD, and treatments show large effect sizes. By following best practice guidance for the assessment and management of OCD in general practice, we hope that the treatment gap can be closed. MT