ADHD in children – what the GP can do

Although treatment of attention deficit hyperactivity disorder (ADHD) usually involves specialist input, the GP plays an important role in assessment and arranging nonpharmacological treatment while waiting for a paediatric appointment. Assessment of a child showing typical ADHD features of inattention, hyperactivity or impulsivity focuses on whether the behaviour is out of proportion to his or her developmental level and whether it is causing functional impairment.
Attention deficit hyperactivity disorder (ADHD) is a common condition of childhood, affecting about 7 to 11% of school-aged children.1 ADHD typically runs in families. It is often associated with other conditions, such as learning difficulties or premature birth.2 Although ADHD is considered a categorical diagnosis – a person either has it or not – the features of ADHD are continuously distributed in the population. It is a lifelong condition, although the symptoms change with different stages of development.
Children with ADHD typically have difficulty concentrating and may also be hyperactive and impulsive.3 Difficulties with concentration may mean that the child becomes distracted every few minutes. Easy or interesting tasks might be manageable, but completing a more challenging task might require an unsustainable level of effort. ADHD disproportionately affects children with learning difficulties, who have to overcome greater challenges to make progress.
For a child showing features of inattention, hyperactivity or impulsivity, the GP needs to evaluate whether the child’s behaviour is out of proportion to his or her developmental level and whether it is causing functional impairment. Although a diagnosis of ADHD opens up the possibility of highly effective treatment, social stigma can be attached to the diagnostic label.4
Assessment for ADHD
A GP may need to evaluate a child for ADHD for the following reasons:
- parental or school concern about ADHD
- the child shows concerning behaviour in the GP’s surgery
- a parent requests a paediatric referral for ADHD assessment
- a parent requests a referral for ADHD therapy.
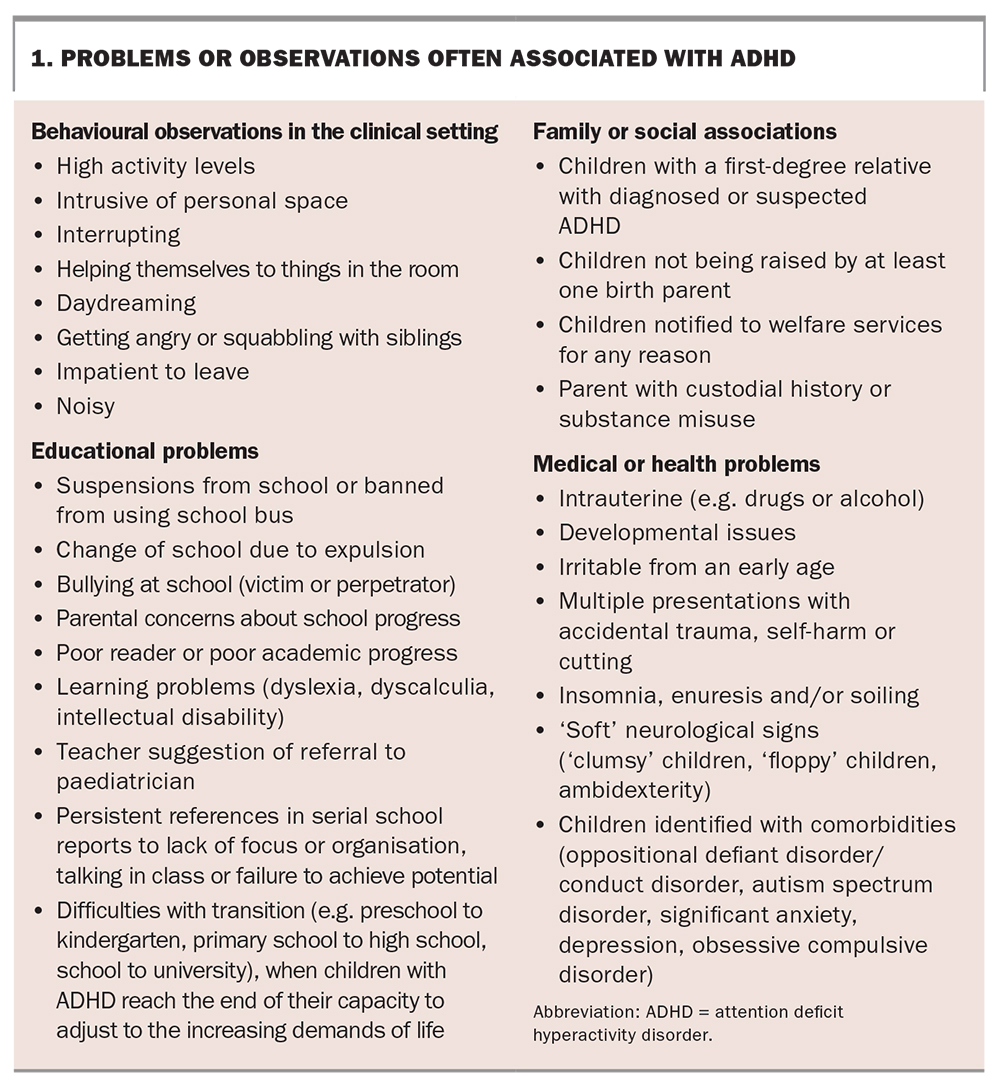
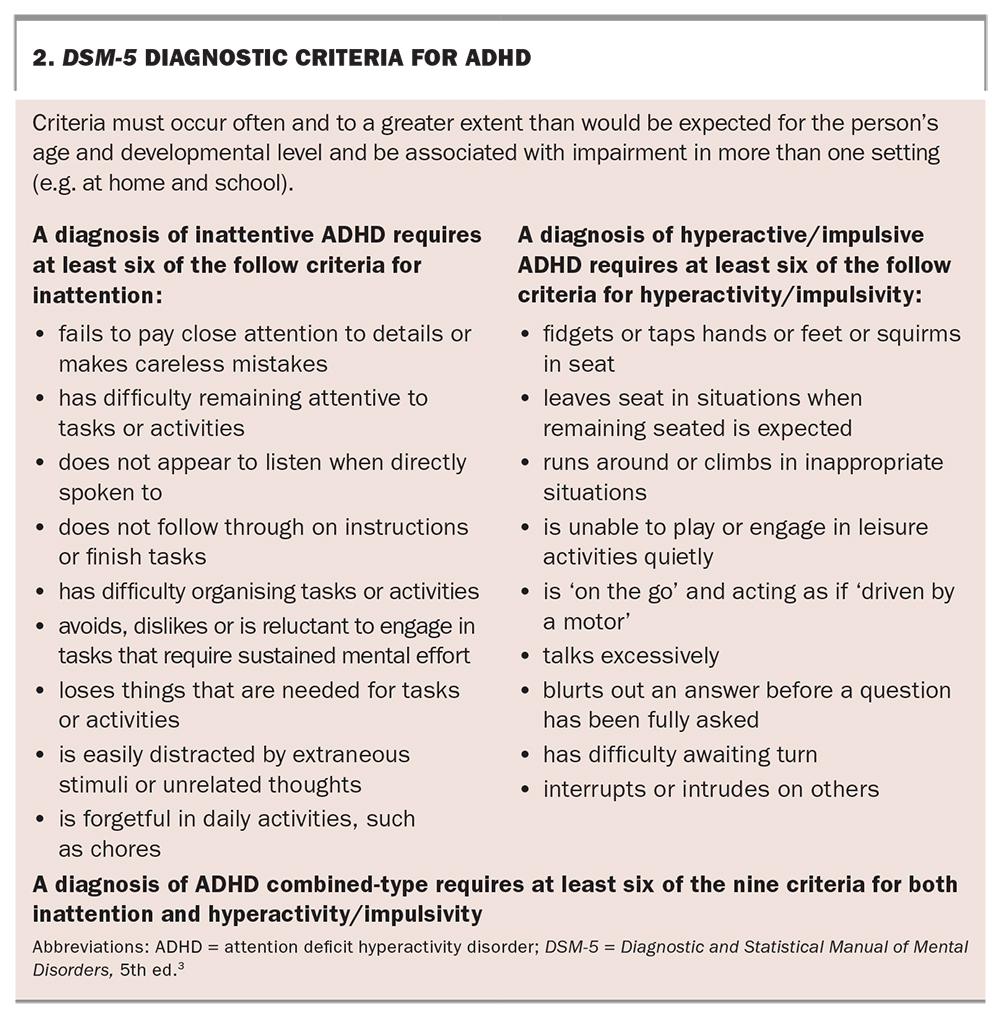
The GP may suspect ADHD based on aspects of the child’s history or clinical observations, such as those listed in Box 1. Repeated nonattendance at appointments is also very common in families with ADHD. A diagnosis of ADHD is based on the Diagnostic and Statistical Manual of Mental Disorders, 5th ed (DSM-5) criteria (Box 2).3
{kind=link}
{kind=link}
Exploring functional impairment in ADHD
One challenge in diagnosing ADHD is that the characteristic behaviour is not specific – most children will display ADHD-type behaviour some of the time – and its symptoms may be subtle. The GP’s history taking should focus on the following domains of functioning, not just symptoms. The problems in functioning then become the targets for therapy.
Underachievement in relation to ability
Children with ADHD typically struggle more as the challenges of schoolwork increase. This may lead to academic decline; for instance, from average or above-average performance in early primary school to being at the bottom of the grade in high school. Understanding a child’s early development is important: a child with ADHD may appear ‘smart’ in preschool and show unexpected difficulties with the increasing demands of starting school. It is therefore a good idea to ask about the child’s academic achievement and progress.
Generating unreasonable levels of stress or disruption at school
A child who cannot concentrate on his or her schoolwork will become bored and may look for entertainment, such as talking, playing or making noises. A hyperactive child may have difficulty remaining seated in class. An impulsive child may keep calling out and interrupting the class.
Questions that the GP can ask the child’s parents or guardians include:
- Has the child been in trouble at school, with detentions or suspensions?
- Are there any special classroom arrangements in place, such as sitting the child at a table near the teacher?
Generating unreasonable levels of stress or disruption at home
A child with ADHD may find concentrating on routine tasks at home, such as getting dressed or doing homework, to be too much effort. Note that being able to concentrate on technology does not count because the child is constantly stimulated by this, without having to make any creative effort.
Questions that the GP can ask the child’s parents or guardians include:
- How long does it take the child to perform routine tasks at home, such as getting ready in the morning, and how many reminders are needed?
- How long does homework take, and how long should it take?
- For what proportion of the time spent on homework is the child actually working?
- How often is the parent feeling stressed?
- Is the child unable to concentrate on playing without a companion and therefore constantly seeking attention?
Significant problems with peer relationships
As children develop and progress, communication skills become increasingly important for sustaining strong friendships. These skills involve listening, processing the information and responding appropriately – all of which require mental effort. Children with ADHD often find it easier to talk about themselves and impose what they want to do. Being bossy may be tolerated in the early years of school, but bossy children can become increasingly ostracised. A teenager may lose concentration and withdraw to the edge of the group. Children with oppositional defiant disorder (ODD) as well as ADHD may show unpredictable spite or anger.
Questions that the GP can ask the child’s parents or guardians include:
- Has the child had any problems with an irritable mood or negative outlook?
- Does the child have friends in the playground and ‘sleepovers’ with other children?
- Does the child show signs of school refusal?
Poor self-esteem
Children with ADHD have to try harder than other children to succeed. This increased effort may be unsustainable. A child with ADHD might keep unintentionally getting into trouble because of his or her inability to stop and think before speaking or acting. Poor self-esteem can then lead to negative feelings and behaviour. A demoralised child is more likely to give up than to try harder. Therefore, poor self-esteem in a child with suspected ADHD can be considered a red flag for prioritising diagnosis and treatment. The GP can ask the child’s parents or guardians if the child seems to be overly self-critical or lacks self-worth.
‘Typical’ ADHD
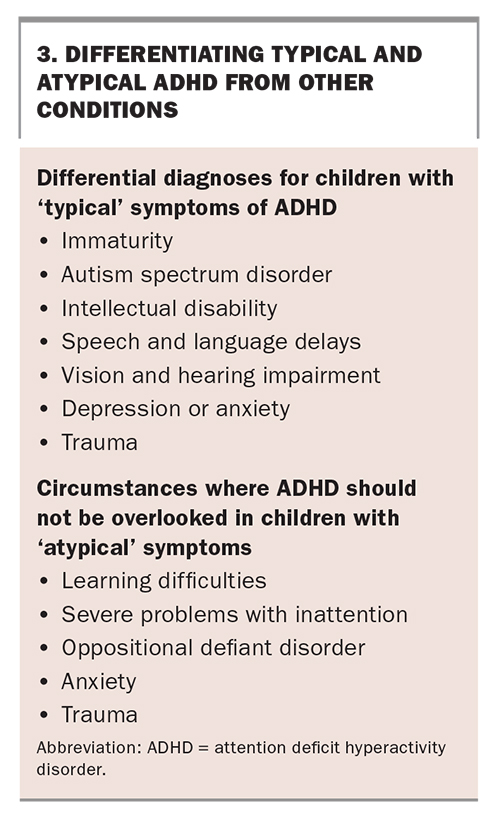
The typical symptoms of ADHD can often be masked or mimicked by, or coexist with, other conditions, so it is important to consider coexisting conditions or alternative diagnoses to ADHD (Box 3).
{kind=link}
Immaturity
The features of ADHD are common in young children. Children mature at different rates. If a young child shows signs of ADHD but appears to be managing tolerably well, it is often better to watch and wait while starting behaviour management strategies. A child with ADHD typically behaves like a child 30% younger than his or her chronological age. Such a child may cope better in a younger peer group. The deciding factor for identifying that a child has ADHD is often that they continue to have problems as they settle into school.
Autism spectrum disorder
ADHD and autism spectrum disorder often coexist, and their associated problems with social communication may look similar. If both diagnoses are being considered, it often makes sense to treat the child for ADHD first and assess whether he or she shows any improvement with medication. In children with autism spectrum disorder, the social problems will persist despite a reduction in the symptoms of ADHD. Behavioural interventions to deal with the problems in functioning are important for either condition and do not require full diagnostic clarity before being implemented.
Specific learning difficulties and intellectual disability
Children with ADHD who are struggling academically may learn more efficiently once their ADHD is treated. However, if the child does not then start to catch up with his or her peers, further appropriate investigation for other learning difficulties, such as speech and language or psychometric assessment, should be undertaken.
Speech and language delays
ADHD may mask a receptive language delay, because in both conditions a child may not follow what is being said. Without formal testing of language skills, it can be difficult to determine whether the child is not listening or not comprehending.
Vision and hearing impairment
A child with a hearing impairment will have to concentrate harder than other children to follow what is going on. This may lead to mental fatigue and loss of concentration. Similarly, a visual impairment will make reading and written work more difficult. Therefore, it is important to test both vision and hearing in children showing these problems.
Depression or anxiety
Children who are depressed or anxious often have difficulty concentrating. Either of these conditions may coexist with and be exacerbated by ADHD and may abate when the ADHD is diagnosed and treated. The time course is often a helpful way to differentiate between ADHD and depression because concentration deficits caused by ADHD should be consistent and longstanding, whereas those caused by depression are more likely to be of recent onset or to run a fluctuating course.
Trauma
Behaviour associated with a background of emotional trauma, abuse or neglect may resemble ADHD, with poor concentration, anxiety and emotional withdrawal or irritability. However, trauma and ADHD often coexist, particularly in families with transgenerational ADHD.
‘Atypical’ ADHD
As some children with ADHD have atypical symptoms, it is important not to overlook a possible diagnosis of ADHD in the following circumstances (Box 3).
Learning difficulties
Deficits with concentration disproportionately affect tasks that are difficult or mentally challenging. Therefore, a minor degree of ADHD will have a more pronounced effect in a child with learning difficulties. A child who is already behind in his or her learning may learn more effectively if the ADHD is identified and treated.
Severe problems with inattention
A child with severe ADHD may be daydreaming or ‘zoned out’ for much of the time. This affects the development of all skills, including social and communication skills. The parent or healthcare professional may have the misconception that such a severe problem could not be caused by ADHD, and the child must therefore have autism spectrum disorder. This misdiagnosis deprives the child of ADHD medication, which might otherwise enable the child to be alert and communicative for a greater proportion of the time.
Oppositional defiant disorder
ODD is common in children with ADHD, occurring in about 40% of those with ADHD combined-type.5 ODD is unusual without ADHD.6 However, ODD can mask ADHD: if a child refuses to attempt any mentally demanding tasks, the child’s teacher may not know that concentration is a problem. ODD can be extremely disabling but often abates with ADHD medication.7 Therefore, it is important to carefully look for the features of ADHD in any child with ODD, particularly if the problems are longstanding.
Anxiety
Anxiety is common in children, affecting about 7%.8 ADHD often exacerbates anxiety in a child who is constantly worried about failing. An anxious child may try particularly hard to not get into trouble at school, which may mask the effects of ADHD, with the stress of the effort coming out as irritability as soon as school finishes. Therefore, it is important to remember that bad parenting is not the only reason for a child to appear to be ‘perfect’ at school while showing features of ADHD that cause high levels of stress and disruption within the family.
Trauma
ADHD often coexists as a problem that requires specific diagnosis and treatment in traumatised children.
Management of ADHD
Management of ADHD in children usually involves a combination of pharmacological and nonpharmacological interventions. The latter include behaviour management and additional learning support, as well as occupational therapy and speech pathology when indicated. Nonpharmacological intervention can be started early, without a diagnosis.
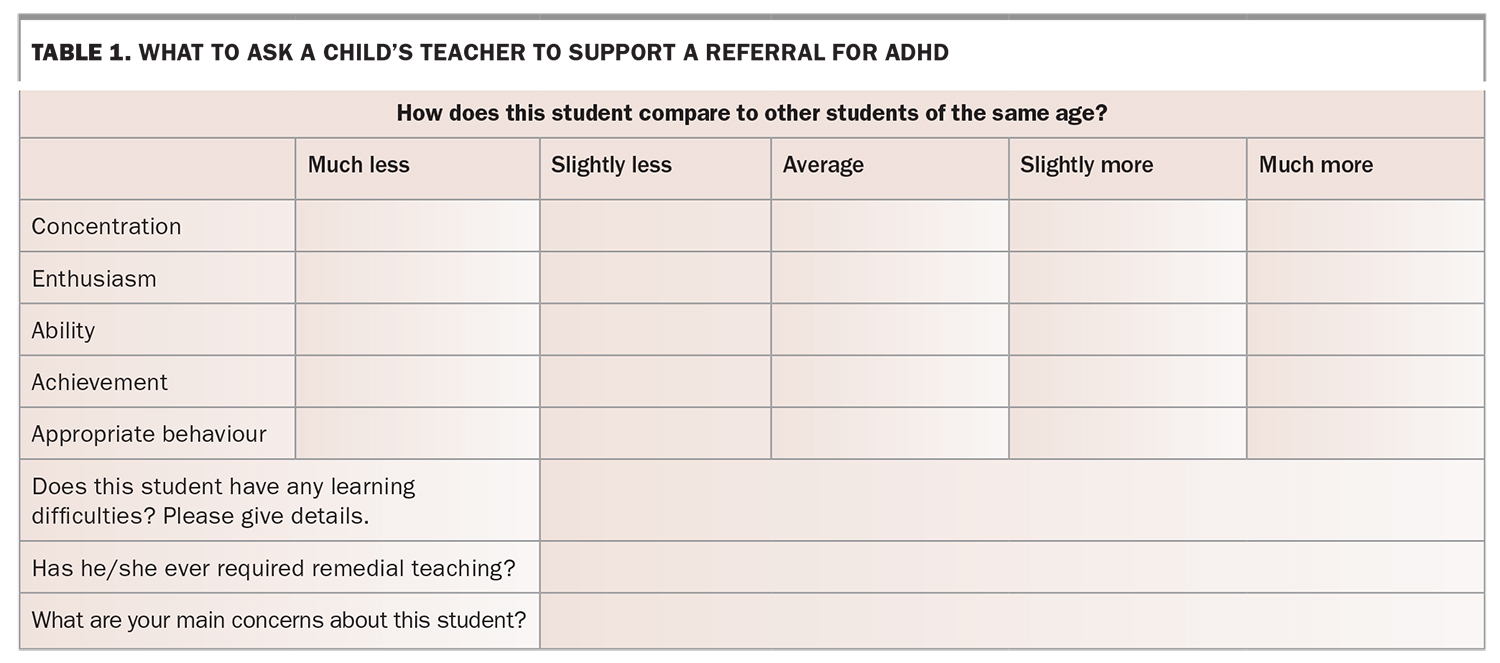
A child may be brought to the GP for the specific purpose of requesting a specialist referral. Paediatricians often have long waiting times for appointments and high consultation fees. A well-constructed referral that highlights the major areas of dysfunction and includes questionnaires, such as Conners 3 (www.pearsonclinical.com.au/products/view/92) or the Vanderbilt ADHD Diagnostic Rating Scale (https://psychology-tools.com/test/vadrs-vanderbilt-adhd-diagnostic-rating-scale), completed by parents or guardians and the child’s classroom teacher, can save everyone significant time, effort and money. The GP can give parents a letter to pass on to the child’s teacher, which asks the teacher to complete an enclosed symptom rating scale (Table 1) and provide any other relevant information, such as a checklist indicating which of the DSM-5 diagnostic criteria the child meets at school, which can then support the referral.
{kind=link}
Although many children with ADHD respond best to a combination of medication and nonpharmacological intervention, not all children need specialist treatment. Even for those who do require stimulant medication, the GP can arrange other interventions while the child is waiting for a paediatric assessment. If the child responds well to such interventions, medication and a formal diagnosis may be deferred or even unnecessary.
Management in general practice
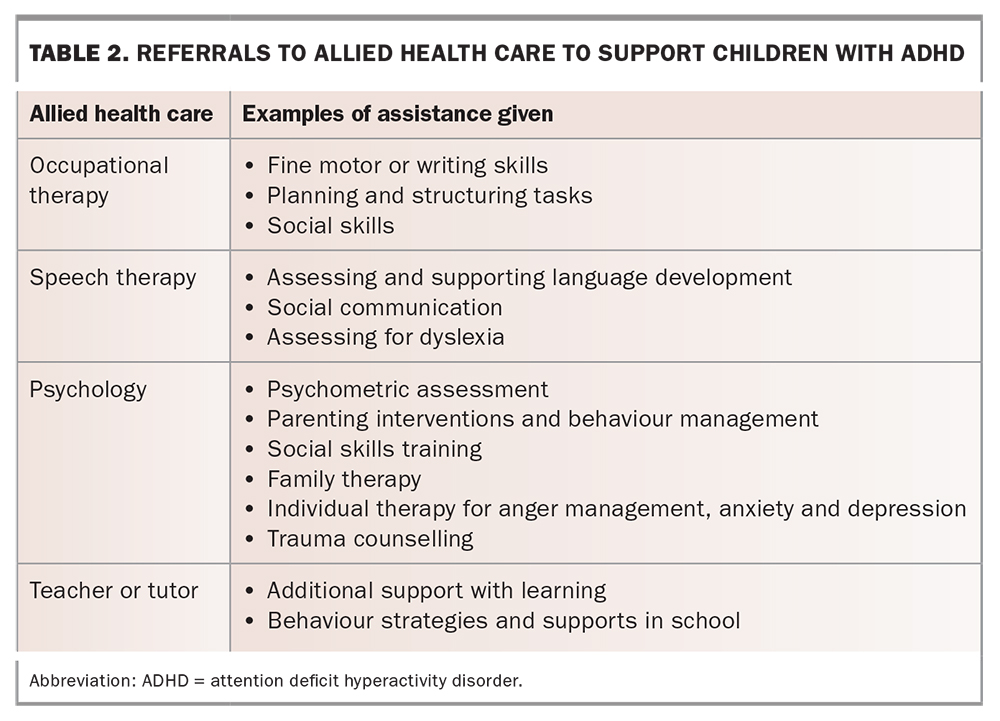
There are several Medicare-supported mechanisms for managing ADHD in igeneral practice, which can include the involvement of allied health professionals (Table 2). Case conferencing can be useful for gathering information from at least two other professionals involved in the child’s care in a notional multidisciplinary care team. These can include health or allied health professionals, educators or community workers providing social support.
{kind=link}
Mental Health Treatment Plan
If ADHD (or any other mental health condition) is diagnosed, the patient can access Medicare-supported psychological therapy or occupational therapy using a Mental Health Treatment Plan. This involves a consultation (either 20 to 40 minutes or more than 40 minutes) to set up the plan, followed by 10 therapy sessions initially and the possibility of a further 10 sessions.
Team Care Arrangement
If there is no mental health diagnosis, or if the child needs a referral to another allied health therapist, a Team Care Arrangement can be used to access five allied health sessions a year. This involves patient input and two multidisciplinary team members, as well as the GP. The allied health professional providing the therapy would be one team member, and the child’s teacher could be the other – a teacher filling out a behavioural questionnaire demonstrates direct communication.
GP Management Plan
A GP Management Plan can be used for a patient with a chronic condition that will last at least six months. The Medicare item number to prepare the plan can be claimed every 12 months, with a further rebate that allows the GP to review the patient every three months to co-ordinate management. Patients can also access allied health care with a GP Management Plan.
The use of templates (available from the Department of Health) is encouraged to better demonstrate Medicare compliance.9 Occasionally, parents will present to the GP because a speech pathologist or occupational therapist has told them to get a referral from their GP, without advising them that the Medicare requirements for a Team Care Arrangement or Mental Health Treatment Plan must first be met. This process takes time and thoroughness to avoid problems if a random Medicare audit takes place.
Family support and education
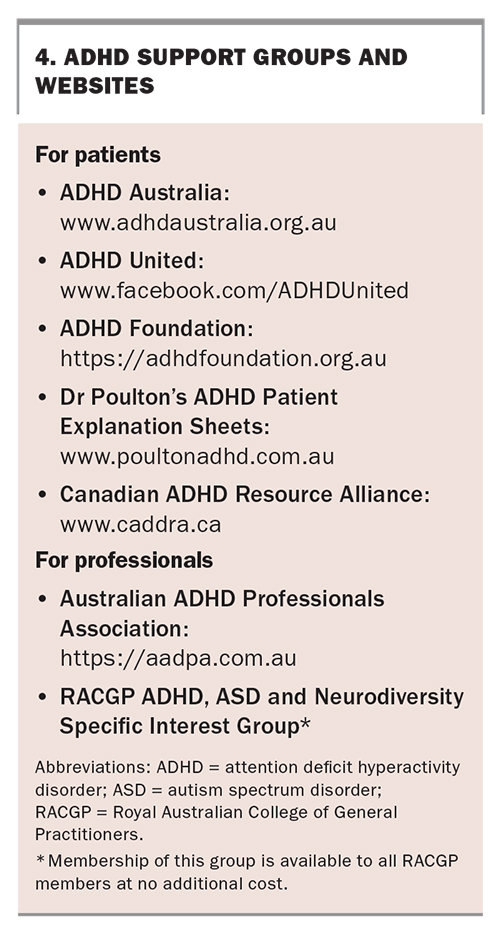
Community ADHD support groups and ADHD websites are good sources of information for patients and parents.10 These include ADHD Australia, ADHD United and the ADHD Foundation (Box 4).
{kind=link}
Medication for ADHD
For children who need medication for optimal treatment of ADHD, gaining access to an appropriate specialist can be a considerable problem. Stimulants are the most commonly prescribed medications for ADHD but are restricted because of their potential for misuse, and it is unusual for GPs to be permitted to prescribe them.
Restrictions in accessing ADHD treatment are increasingly recognised as an Australia-wide problem. In NSW, the Henry Review recommended trialling new models of integrated care for ADHD involving GP prescribing.11 In the future, restrictions on GP prescribing would need to be eased to allow the GP to take on a greater role in ADHD management.
In the meantime, GPs can prescribe the nonstimulants atomoxetine and guanfacine using a private prescription. Alternatively, clonidine is cheap and can stabilise the situation.
Stimulants
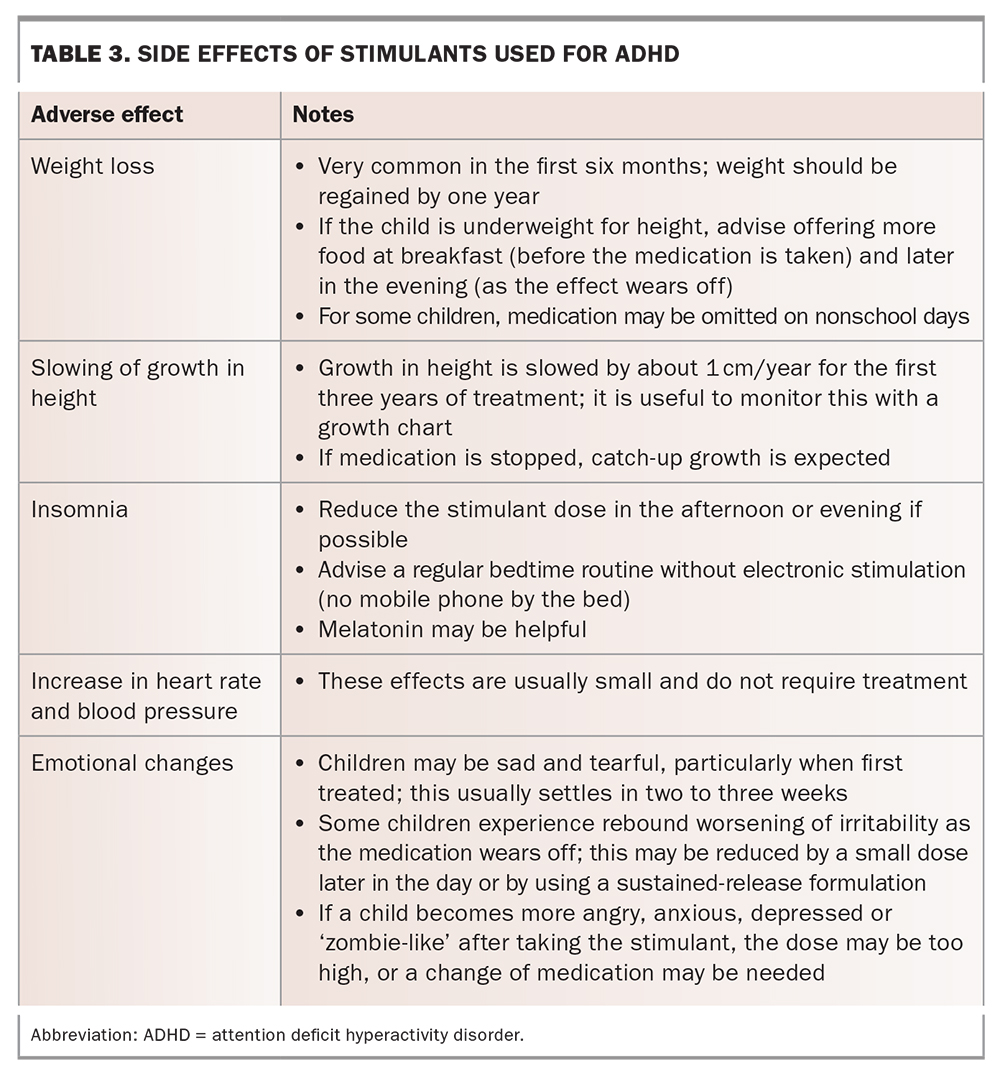
In Australia, the stimulants generally prescribed for ADHD are methylphenidate, dexamfetamine and lisdexamfetamine. GPs can monitor medication efficacy and side effects with the parent and child and by requesting reports and ratings from the child’s teacher. Stimulant side effects are outlined in Table 3.
{kind=link}
Most children with ADHD show an obvious positive response to medication, with an improvement that may be immediate and dramatic. Stimulant medication is often so effective that, once treatment starts, a child who had been behind in his or her learning may catch up quite rapidly, particularly in the early years of school. Therefore, a few months’ delay in starting pharmacological treatment may not have any detrimental long-term effect.
Atomoxetine
This is a selective noradrenaline reuptake inhibitor. Prescribing atomoxetine is similar to prescribing a selective serotonin reuptake inhibitor. It can be prescribed by GPs, as it does not have the misuse potential of stimulants.
Alpha-2 adrenergic agonists
The alpha-2 adrenergic agonists guanfacine and clonidine can also be prescribed for ADHD. Guanfacine is effective for treating ADHD as monotherapy or in combination with a stimulant. It is an antihypertensive agent, so blood pressure should be monitored. Guanfacine is available as an extended-release formulation for once-daily dosing. Clonidine has similar effects but does not last as long and is often more sedating.
Conclusion
Despite ADHD being a condition that usually involves specialist input, the GP can fulfil a valuable role in assessment and arranging nonpharmacological treatment. GP referral to a specialist that includes a detailed description of the child’s problems, with reports and ratings from parents and teachers, can help with triaging and reduce delays in starting pharmacological treatment. MT
COMPETING INTERESTS: None.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.