Recurrent painful intertriginous nodules

Hidradenitis suppurativa
Test your diagnostic skills in our regular dermatology quiz. What is the cause of these painful lesions occurring on a woman’s vulva and groin?
Case presentation
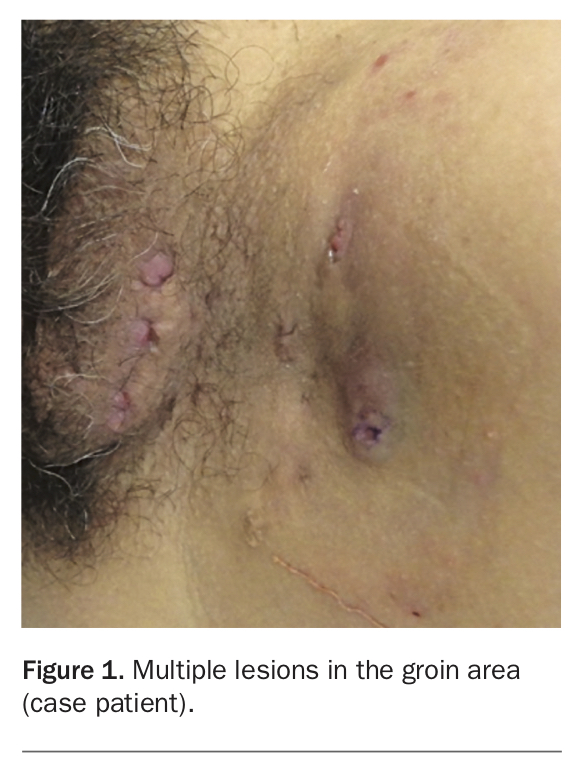
A 32-year-old woman presents with recurrent nodules and pustules on the left side of the vulva and extending to the groin (Figure 1). The lesions are painful and exude pus. She has been treated for the condition several times with antibiotics, despite bacterial swabs consistently returning negative results.
{kind=link}
Differential diagnoses
Conditions to consider among the differential diagnoses include the following.
- Recurrent furunculosis. Colloquially known as a ‘boil’, a furuncle is a deep bacterial infection of the hair follicle. It is most commonly caused by Staphylococcus aureus but Gram-negative bacteria can also cause anogenital furunculosis.1 Risk factors include crowded living environments, chronic S. aureus carriage in the anterior nares, obesity, diabetes mellitus, HIV infection, atopic dermatitis and chronic wounds, but recurrent furunculosis can occur in healthy individuals.1 Furuncles present as painful, erythematous, indurated nodules that can occur anywhere there is hair-bearing skin, but the lesions are most common on the face, neck, perineum and sites of trauma or friction.1 Patients are systemically well, although there may be associated regional lymphadenopathy.1 A bacterial swab for culture is indicated in each episode of recurrent furunculosis to guide systemic antibiotic therapy and ensure coverage for potential underlying methicillin-resistant S. aureus infection.
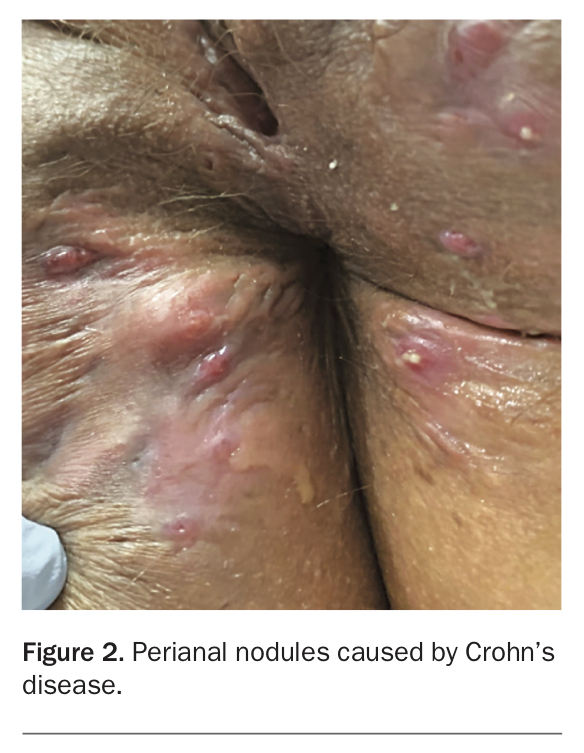
- Crohn’s disease (CD). A chronic inflammatory granulomatous disease affecting the entire gastrointestinal tract, CD is characterised by noncaseating granulomatous lesions that can cause debilitating strictures, fistulae and abscesses.2 CD commonly occurs between the second and fourth decades of life.2 Dermatological manifestations are the most common extra-intestinal finding, affecting up to 75% of individuals with CD and preceding intestinal diagnosis in 25% of cases.2 Cutaneous CD lesions are classified as granulomatous extension of gastrointestinal CD (e.g. perianal skin tags, fistulae, sinuses [Figure 2], oral aphthous ulcers), reactive lesions (e.g. erythema nodosum, pyoderma gangrenosum), or lesions resulting from CD-related chronic malnutrition (e.g. acrodermatitis enteropathica-like syndrome).2 Lesions may therefore be contiguous with the gastrointestinal tract in the perianal region or metastatic, occurring on other parts of the skin. Early contiguous CD lesions begin as erythematous papules that evolve into nodules that then ulcerate with purulent discharge.2 Metastatic CD is rare but can occur in the genital region where it is characterised by erythema and swelling; nongenital metastatic CD varies and can present as erythematous papules, plaques and nodules.2 Biopsy is diagnostic and shows noncaseating granulomas with multinucleated giant cells affecting the dermis that are negative for Gram, periodic acid schiff (PAS) and Ziehl-Neelsen stains.2
- Epidermoid cyst. Epidermoid cysts (inclusion cysts) are well-demarcated, pink to yellow fluctuant nodules with a central punctum indicating a keratin plug communicating with the skin surface. They can arise anywhere but commonly occur on the back, face and anterior chest wall;3 multiple epidermoid cysts can occur on genital skin. These nodular lesions commonly remain dormant but can grow, with subsequent rupture provoking a localised inflammatory response and resultant exudate.3 The cysts can arise in the setting of follicular occlusion (e.g. acne vulgaris) and drug treatments (e.g. BRAF inhibitors).4 Biopsy shows a true cyst – that is, a keratin-filled cyst lined by stratified squamous epithelium.3 Epidermoid cysts occurring in uncommon areas or in conjunction with lipomas, fibromas and pilomatricomas are seen in Gardner syndrome, a variant of the autosomal-dominant familial adenomatous polyposis – these patients require colectomy because of the risk of colorectal adenocarcinoma.3
- Mycobacterial abscess. Cutaneous infections caused by the Mycobacterium genus have diverse clinical presentations. They are classified by the causative organism:
– (i) Mycobacterium tuberculosis complex
– (ii) Mycobacterium leprae and Mycobacterium lepromatosis
– (iii) nontuberculous mycobacteria (which includes both slow and rapidly growing mycobacteria).5
Cutaneous tuberculosis (TB) is uncommon, with a prevalence of 2% in those with mycobacterial infection, and rarely coexists with pulmonary or extrapulmonary TB.5 Scrofuloderma is a worrisome harbinger of concomitant visceral and cutaneous TB and is due to localised cutaneous extension of an underlying TB-infected structure, most commonly a lymph node but it can also be a bone or joint.5 It presents with enlarging indurated subcutaneous nodules, most commonly on the neck, that ulcerate with subsequent sinus tracts exuding purulent or caseous discharge.5 Biopsy shows caseating granulomas with acid-fast bacilli, typical of mycobacteria.5 - Hidradenitis suppurativa (HS). This is the correct diagnosis. HS is a chronic inflammatory disease of the pilosebaceous unit resulting in follicular occlusion, rupture and resultant dermal abscess formation.6 HS occurs in intertriginous areas where there is an abundance of apocrine glands, such as the axillae, inguinal folds and perineal, anogenital and inframammary areas.6 Acute HS presents with multiple tender erythematous subcutaneous nodules and abscesses, which over time develop sinus tracts (double-ended pseudocomedones) and hypertrophic scars – these are visible in Figure 1.6 The sinus tracts express purulent, malodorous exudate, which is typically sterile.6 HS affects 1% of the population, commonly affecting individuals in their second and third decades of life, and has a predominance in females. However, there is a familial form of HS that has an autosomal-dominant mode of inheritance.6 It is one of four diseases in the ‘follicular occlusion’ tetrad – along with acne conglobata, dissecting cellulitis of the scalp and pilonidal cysts – and it is not uncommon for patients to be affected by multiple disorders within the tetrad.6 Other associations with HS include the autoinflammatory syndromes PASH (pyoderma gangrenosum, acne vulgaris, HS) and PAPASH (pyogenic arthritis and PASH); it is also associated with obesity, smoking and CD.6
{kind=link}
Diagnosis
HS is a clinical diagnosis. The aim of initial evaluation is to exclude differential diagnoses; this includes bacterial cultures to exclude acute bacterial infection, and biopsy to exclude cutaneous CD.6 Biopsy of a HS lesion shows follicular plugging and deep dermal fibrotic changes with mixed granulomatous/suppurative infiltrate.6 HS should be suspected for any chronic relapsing pustular condition of the intertriginous areas associated with scarring, sinuses and comedones, particularly if bacterial swabs do not return positive results on culture.
Management
HS is a chronic debilitating disease that has a significant psychosocial impact for affected patients. The Hurley staging system is used to classify the extent of the disease but is not reflective of disease activity.6 For Hurley stage I lesions (abscesses without sinus tract formation or cicatrisation), first-line treatment is antimicrobial agents (systemic and/or topical)6 and antiandrogen therapy; additional modalities include intralesional corticosteroids and oral zinc.6 Clindamycin has been shown to achieve reduction in abscesses and pustules and has synergistic benefits when used with other antibiotics (e.g. rifampicin, minocycline), while corticosteroids are useful for the acute management of inflammatory nodules.6 Higher tier treatment options are reserved for Hurley stage II lesions (separated recurrent abscesses with sinus tract formation and scarring) and stage III lesions (multiple interconnected tracts and abscesses within an area), which include CO2 laser ablation, immunosuppressive therapies such as adalimumab and surgical excision.6 Recommended lifestyle modifications for patients with HS include weight loss, smoking cessation and avoidance of tight-fitting clothing.6
There are significant clinical complications of HS, which include anogenital strictures and fistulae, anaemia, contractures, cutaneous squamous cell carcinoma, epidural abscess and osteomyelitis.6 HS is associated with metabolic syndrome and polycystic ovarian disease and patients should be appropriately screened.7,8
Outcome
This patient’s lesions were consistent with Hurley stage II HS. A biopsy was performed, with results showing nonspecific mixed granulomas. She was started on spironolactone 100 mg daily, which proved ineffective. A six-week course of rifampicin and clindamycin was initially effective, but unfortunately her lesions recurred six months later. She was later treated with adalimumab, with a good outcome. MT