Drowning: a practical review of prehospital intervention

Despite a recent decrease in drowning deaths, the number of drownings in Australia remains too high. Being reminded of key considerations for a drowning emergency is helpful preparation for health professionals who may take control at the scene.
As a GP doing shifts in the local emergency department (ED), you remember each case of drowning you have seen over the years. These cases are so distressing for all – family, friends, first responders, even ambulance, police and ED staff. You and your family enjoy the seaside, and at times you have helped in drowning incidents. It is an area of ongoing interest to you. After another near tragic case of a toddler who was found in the nick of time at the bottom of a backyard pool, you are happy to do a review of the topic for the ED education session.
Drowning terminology
The terminology used in drowning was based on the Utstein guidelines for uniform reporting of data from drowning-related resuscitation.1 It is now recommended that the all-embracing term ‘drowning’ be used and not other terms (e.g. ‘submersion injury’, ‘nonfatal drowning’, ‘wet or dry drowning’, ‘fresh- or saltwater drowning’) as they overlap and can be confusing.2,3
Emergency department and other hospital care of nonfatal drowning cases is not discussed in this article but is covered in the references provided.3,4
Epidemiology
In Australia:
- an average of 288 drowning deaths per year were reported between 2008/09 and 2018/194
- in 2017, 685 nonfatal drownings required hospitalisation3
- in 2019/20, there were 248 drowning fatalities, with males aged 25 to 34 years the most at risk5
- the age distribution of drowning is bimodal, with the peaks in children aged under 5 years and males aged 15 to 25 years3
- males accounted for 80% of drowning deaths in 2019/205
- First Nations Australians are four times more likely to drown than other Australians3
- among children who died from drowning in 2017, 52% were female and the most common location was a swimming pool.3
Good news
Recently, however, there has been some good news. In 2019/20 there was an 8% decrease in drowning deaths in adults in Australia compared with the previous year, and a 52% decrease in such deaths in children under 5 years of age.5 This may be due to increased regulation by councils of swimming pool fences and gates.
Possible effects of COVID-19 restrictions
The increase in local tourism because of travel restrictions due to the COVID-19 pandemic, as well as the highlighting in social media of idyllic, remote, photogenic (selfie) locations, may exacerbate water-related misadventure.6 These remote locations often have difficult access, no phone reception and no lifesaver capabilities, and attract groups with poor or no swimming or lifesaving skills. Also, there may be a cohort of children who have missed out on swimming lessons.
Risk factors and risk-taking
Risk factors for drowning include:2,3,5,7,8
- use of alcohol and/or drugs (alcohol has been implicated in 41% of drowning incidents in Australia3)
- lack of safety devices such as lifejackets (since 2004, only 4% of rock fisherman who died from drowning in Australia wore a lifejacket or a personal flotation device5)
- underestimation of swimming capabilities (most drowning deaths occur while swimming)
- unpatrolled beaches
- rip currents (these have contributed to 25% of coastal drownings in Australia since 20045).
Even at patrolled beaches, people often do not swim between the flags. For example, people may swim with their children at the ends of beaches near rocks, thinking it is safer because the waves are smaller, unaware that this is because of the strong currents around the rocks. Multiple tragedies sometimes occur when family members who are not competent swimmers jump in to save others.
Pathophysiology of drowning
Once fluid enters the airway of a drowning person, coughing occurs, and continued aspiration of fluid leads to hypoxaemia and apnoea. The sequence of cardiac activity is sinus tachycardia, bradycardia, pulseless cardiac activity and then asystole. An acute lung injury occurs by the water entering the airway, and bronchospasm of water into the alveoli then causes surfactant dysfunction, disruption of cell membrane integrity with atelectasis and low lung compliance. Aspiration of significant volumes can cause fluid and electrolyte shifts. Potential aspiration of gastric contents or foreign material should be kept in mind.2,3
Hypothermia occurs particularly with very young children or very cold water. Low water temperatures can be associated with better outcomes.2,3
Precipitating events
In children and young adults, precipitating events for drowning include hypoglycaemia, seizures, drug and alcohol use, arrhythmias, child abuse or neglect and nonaccidental injury. Precipitating events in adults include cardiac events, stroke, hypoglycaemia, suicide and head injury (e.g. sailors hit by the boat’s boom).
Treating a drowning patient at the scene
Basic life support
The DRSABCD action plan should be applied as detailed below. However, important precautions currently apply, as highly infectious COVID-19 disease is widespread (Box).
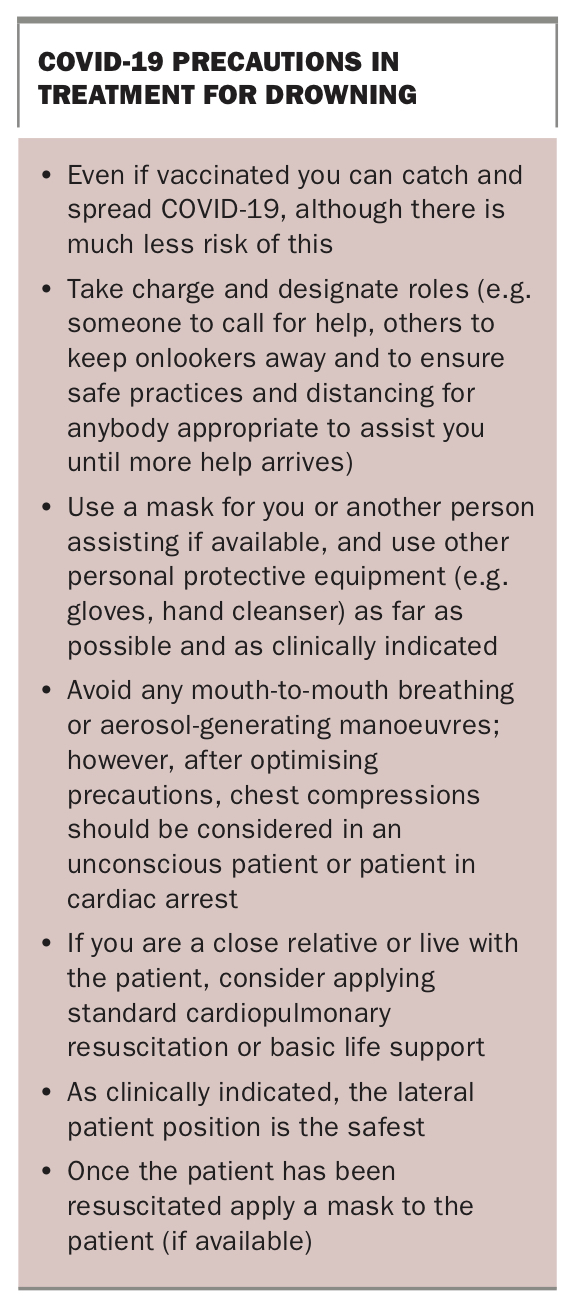{kind=link}
- Danger:
– recognise the person is in distress4
– be aware of danger and risks to the victim and rescuer
call for help
– provide flotation device4
– remove the victim from the water if it is safe to do so
- Response: is the victim conscious and responsive?
- Send for help
- Airway:
– open the patient’s airway; if there is fluid in the mouth/oropharynx briefly turn the person on their side for the fluid to drain out by gravity
– maintain neck alignment as much as possible and note the history (possibly a jump); however, less than 5% of drownings involve a neck injury
– note that Heimlich manoeuvres and longer drainage efforts have not been shown to benefit survival
- Breathing: two, and preferably five, rescue breaths are indicated if the patient is not breathing normally
- Circulation: apply 30 chest compressions to two breaths (30:2) aiming for at least 100 compressions per minute
- Defibrillation: attach an automated external defibrillator as soon as possible for unconscious adults who are not breathing, after drying the patient and removing sand as much as possible.
Hypothermia
Hypothermia is to be presumed in a case of drowning. To stop further heat loss:
- remove wet clothes
- dry the patient
- wrap the patient in dry, warm material.9
Key information
Notes should be made of what happened in the drowning event.4 These should include the following:
- details of any witnesses
- times, especially of submersion
- temperature of the water
- initial clinical state of the victim, especially conscious state, breathing, circulation and colour
- resuscitation efforts, length of time performed and responses
- ambulance rescuer arrival.
Examination
Examination of the victim includes:
- conscious state (Glasgow Coma Scale)
- vital signs as possible
- respiratory description, colour, cough, respiratory rate, any vomiting
- any obvious trauma – head or neck, fracture or lacerations.
On history or examination of any injury patterns, be aware of any distracting injuries which may suggest or distract from a cervical spine injury.
Prehospital care
Most self-extricated or rescued drowning patients do not require hospital evaluation or treatment. Only 0.5% require cardiopulmonary resuscitation, and only 6% of those rescued by lifesavers require hospital attendance.3,4
Potential factors assessed by health professionals that may allow for the patient to be released from the scene include:
- normal skin colour
- no cough
- normal respiratory rate and pulse oximetry result
- normal vital observations – temperature, pulse, blood pressure
- no shivering
- fully conscious
- dischargeable in the company of a responsible adult.
The following actions should be considered in the continued prehospital care of drowned patients:
- use high-flow oxygen
- early intubation with positive end-expiratory pressure (PEEP)
- despite fluid or pulmonary oedema, limit airway or tracheal suctioning
- cardiopulmonary resuscitation 30:2, unless the rescuer is unwilling to perform mouth-to-mouth breathing and chest compressions alone are applied
- administer drugs by intravenous or intraosseous routes
- treat hypotension with crystalloid fluids
- provide standard advanced life support (ALS) with special attention to reversible issues (e.g. hypoxia and hypothermia).
Conclusion
The risk of water-related misadventure in Australia is high because of the country’s temperate climate, the vast majority of its population living near water, mainly on the coast but also near rivers and inland waterways, and the increasing number of backyard pools. Successful education about drowning prevention (including the basics of life support) is essential and should be achieved. MT
COMPETING INTERESTS: None.