Acute pain in patients with substance use disorder: steps for successful assessment and management

Patients with substance use disorder presenting with acute pain may be challenging to assess and manage. Key steps are excluding serious pathology and instituting management that promotes comfort, reduces distress and minimises harm. As in other patients with acute pain, nonpharmacological and nonopioid treatments are first-line options. Opioids have only a limited role for more serious pathologies and in accordance with published guidelines and regulatory frameworks.
- Treating doctors should consider the possibility of substance use disorder (SUD) in all patients presenting with pain (‘universal precautions’).
- Strategies promoting a positive therapeutic relationship are crucial for successful assessment and treatment of all patients with SUD.
- Potentially serious pathology should be sought in patients presenting with SUD and acute pain, while considering that some drugs are associated with specific painful conditions and other effects that influence acute pain presentations.
- For all patients, nonpharmacological and nonopioid treatments should be maximised and opioids used sparingly, with use of atypical opioids preferred.
- Patients taking opioid agonist therapy for SUD should be assessed and managed similarly to other patients with SUD.
- The relationship between SUD and chronic pain is bidirectional; self-management approaches help patients with SUD and chronic pain deal with their chronic symptoms as well as cope with acute pain flare-ups.
- A patient’s level of risk, according to the presence of active drug use, mental illness and other comorbidities should guide referral to a primary care specialist or drug and alcohol facility.
In 2019, one in 25 Australians aged 14 years and older reported taking drugs available to buy from pharmacies for nonmedical reasons in the previous year.1 Within this group, the use of prescription analgesics (including opioids) fell compared with 2016, largely due to codeine rescheduling in 2018. Regulation of alprazolam also reduced its availability and nonprescribed use.2 Although overall use of alcohol and tobacco is declining, particularly in higher socioeconomic areas, alcohol remains the most common substance associated with substance use disorder (SUD).1 Illicit drug use is stable in lower socioeconomic areas but is increasing in wealthier areas.1 More than one in ten Australians report recent use of cannabis, with one-third of these using cannabis at least weekly.1 Past-year use of cocaine (2.5%) and ecstasy (3.0%) is increasing, while use of methamphetamine and other amphetamines, predominantly crystal meth or ‘ice’, is decreasing.1 The proportion of users taking multiple drugs has increased, raising risks of SUD and other harms. Those using prescription opioids frequently report they are unable to stop their use, even if they would like to do so.
There is significant concordance between SUD and chronic pain, with overlapping mechanisms in both conditions.3 Many individuals with SUD report long-term pain, and one fifth of those with chronic pain meet SUD diagnostic criteria.4,5 The range of patients seen in primary care includes those on opioid agonist therapy (OAT) and those in SUD recovery. This article addresses acute pain in the presence of SUD: screening for SUD, detecting serious pathology, and management, including for those with acute flare-ups of chronic pain conditions or treated with OAT.
Assessment of patients with SUD and acute pain
Consider the possibility of SUD in all patients presenting with acute pain
Treating doctors should consider the possibility of SUD in all patients presenting with pain (‘universal precautions’).6 Risk factors for SUD include family or personal history of SUD, history of childhood sexual abuse, concurrent psychiatric illness and younger age.3
Screening questionnaires (e.g. CAGE [cut down, annoyed, guilty, eye-opener] Substance Abuse Screening Tool; AUDIT [Alcohol Use Disorders Identification Test]; ASSIST [Alcohol, Smoking and Substance Involvement Screening Test]) may be used, although all tools rely on self-reporting and there are complex reasons why this may not occur.6,7
Clear signs of drug and alcohol misuse such as needle tracks, intoxication and withdrawal may also be present. In some Australian states, real-time prescription monitoring supports screening and decision-making (e.g. SafeScript in Victoria, which includes a clinical advisory service).8
The Prescription Shopping Program and MyHealth Record are other potential sources of information about individuals, although each has limitations.9 An overriding consideration is that SUD may occur in any patient, in any context.10
Ensure your approach reduces stigma and promotes clear expectations
Australians with SUD, especially injecting drug users, report negative experiences in both hospitals and primary care. This includes being ‘looked down on’, ‘treated like less than nothing’ and subjected to derogatory remarks.11,12 Many have found it difficult to access pain relief even when they present with clearly painful conditions.11 These recollections lower their expectations that they will receive the care that others take for granted, and may hinder them seeking treatment.12 The consequences are patient suspicion, distrust, late presentations and increasing drug use to cope.12 Of course, there are some with SUD who are drug-seeking and who are sometimes perpetrators of violence in general practices and hospitals, particularly when intoxicated or if they suffer comorbid mental illness.13,14 A further complicating factor is that pain-relief seeking may look like drug seeking, with resolution of behaviours once pain is adequately addressed (so-called pseudoaddiction).15
Some strategies to consider within the therapeutic relationship are:
- being open and nonjudgemental, with reassurance about the treatment approach
- empathy with therapeutic boundaries, including setting realistic expectations and clear limits16
- using a disease model of SUD, noting that it is due to pathological processes such as disruption of reward circuits in the brain so that drug use is intensely reinforcing, both physically and psychologically
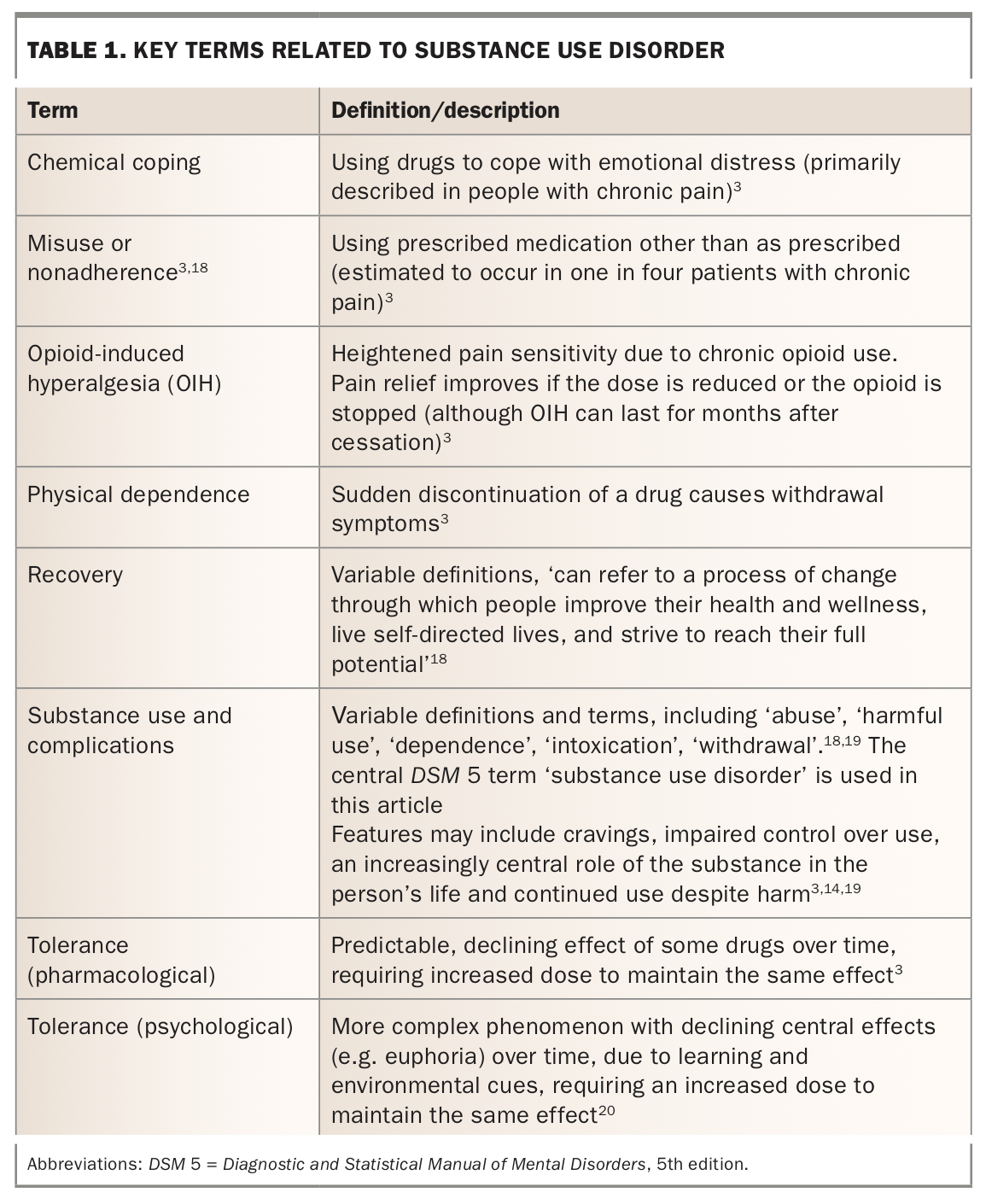
- applying terms appropriately, avoiding stigmatising terms (like ‘addiction’) and using person-first language (e.g. ‘a patient with SUD’)17 (Table 1)
- following practice policies on opioid prescribing and adherence to relevant professional guidelines (see below)10
- careful individualised risk assessment.
{kind=link}
Look for symptoms and signs of potentially serious pathology
A foundation of successful pain management is commencing disease-specific treatment, when relevant. The implications of SUD in terms of diagnosis in acute pain presentations include:
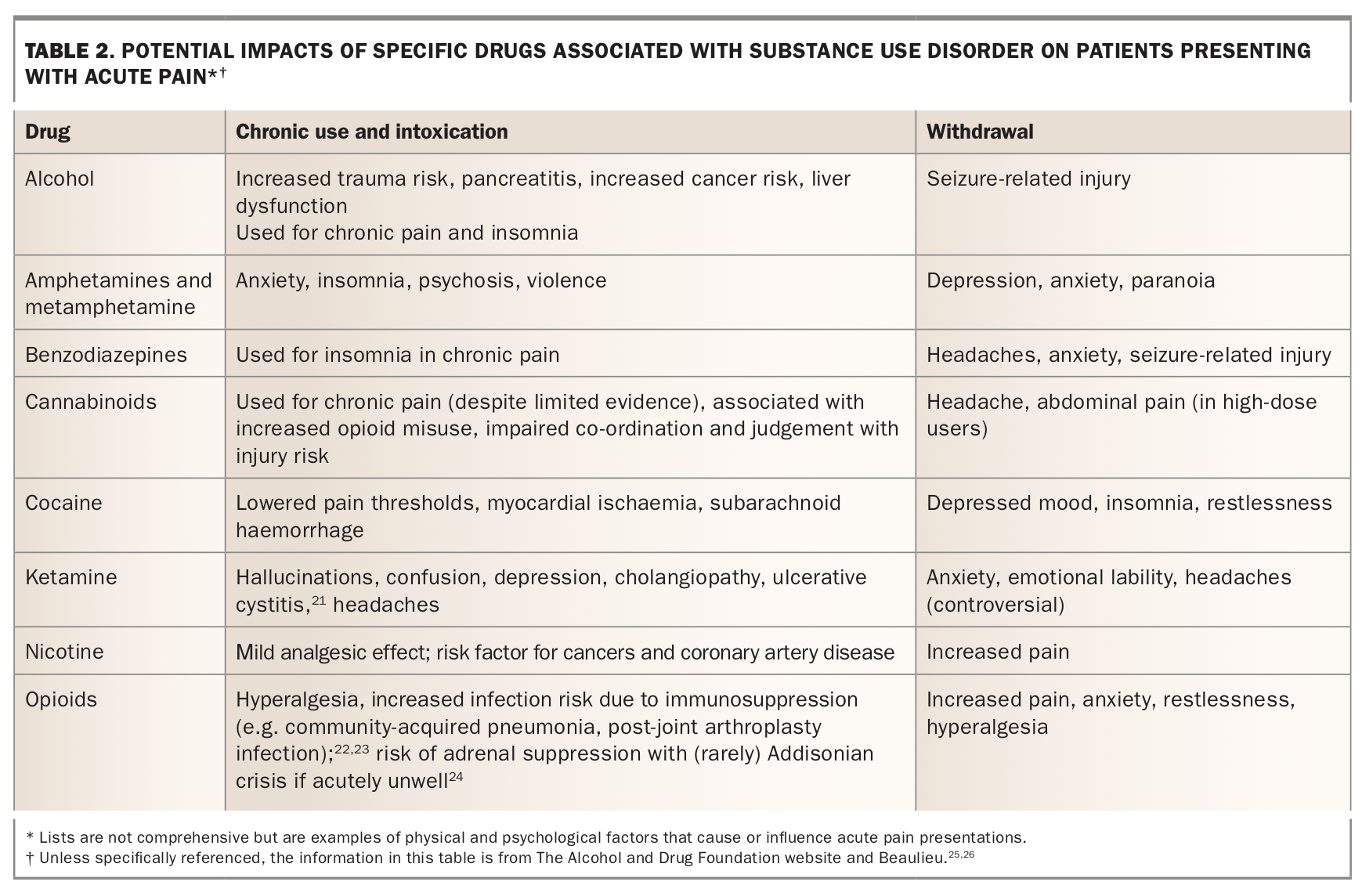
- Some drugs are associated with specific painful conditions and other effects that influence acute pain presentations, for example anxiety and sleep disruption (Table 2).
- Injecting drug use increases the risk of infections such as epidural abscess and discitis, limb ischaemia from inadvertent arterial injection and nonfatal drug overdose resulting in pressure injuries and venous thrombosis.27
- Long-term opioid use leads to poorer surgical outcomes, such as deep vein thrombosis and infection, so maintain a high index of suspicion for complications in a patient with opioid use disorder (OUD) who has undergone recent surgery (Table 2).28
{kind=link}
Management of patients with SUD and acute pain
For all patients, maximise nonpharmacological and nonopioid treatments
The first-line treatment options for acute pain in the presence of SUD, as for other patients, are nonpharmacological and nonopioid. The precise approach will be determined by circumstances, but options that can be considered include:
- following best practice professional guidelines on acute pain, e.g. for management of nonspecific low back pain in primary care (Box 1)29
- education and reassurance about the role of investigations, the reason for not prescribing opioids (as relevant) and the role of nonopioids
- addressing psychological contributors such as anxiety14
- use of simple analgesics, especially anti-inflammatories, with paracetamol only indicated in selected conditions14
- use of adjuvant agents for neuropathic pain, e.g. duloxetine (off-label use), amitriptyline (off-label use), gabapentin, pregabalin, carbamazepine (first-line for trigeminal neuralgia), recognising that pregabalin in particular is a drug of misuse as well as the risk of overdose with tricyclic antidepressants30
- use of disease-modifying agents in the presence of relevant diagnoses, e.g. for antimigraine treatment or prophylaxis
- nonpharmacological treatments – the NPS MedicineWise website has excellent supporting information on these31
- lifestyle-based management, as for other chronic conditions16
- providing symptomatic treatment for withdrawal symptoms, e.g clonidine (off-label use) provides symptomatic treatment for opioid withdrawal, mild analgesic effect and anxiolysis. However, side effects, particularly hypotension, can limit its use. OAT is often the best opioid withdrawal treatment.
The consultation also may present an opportunity to divert the patient towards harm minimisation and drug and alcohol treatment services, and for management of comorbid psychiatric disorders, as relevant.32
Use opioids sparingly and consider atypical opioids which are effective with lower risk
Opioid-related harms in Australia include three deaths and 150 hospital admissions per day.33 NPS MedicineWise promotes five reasons not to prescribe opioids:34
- adverse events
- limited evidence for efficacy
- opioid-induced hyperalgesia (Table 1)
- misuse risk
- comorbidities and drug interactions.
Recent TGA and PBS changes emphasise the role that prescribing for acute pain can have in persistent long-term use, requiring smaller pack sizes and promoting best-practice prescribing.35 For example, recent more restrictive TGA indications for the high-potency opioid fentanyl recognise the risks of significant misuse, diversion and overdose.35 Atypical opioids (tramadol and tapentadol) have multimodal action and are effective for neuropathic pain and in opioid tolerance (no tolerance to the nonopioid component).36 When compared with conventional opioids, they have reduced risk of misuse, diversion, doctor-shopping and overdose deaths.3,37,38 However, drug interactions and side effects, particularly with tramadol, should be considered.
If prescribing opioids, it is recommended to do so at the smallest dose for the shortest duration possible. The patient who is opioid-tolerant (due to heroin or prescription opioid use) may require higher opioid doses due to pharmacological tolerance (Table 1). There is also some cross-tolerance between cannabis and opioids, but not between most other drugs and opioids, so usual doses are appropriate in most other cases. Additionally, each presentation presents an opportunity to assist the patient to access definitive and effective treatment for their SUD (e.g. OAT) and for harm minimisation strategies such as take-home naloxone.14,39
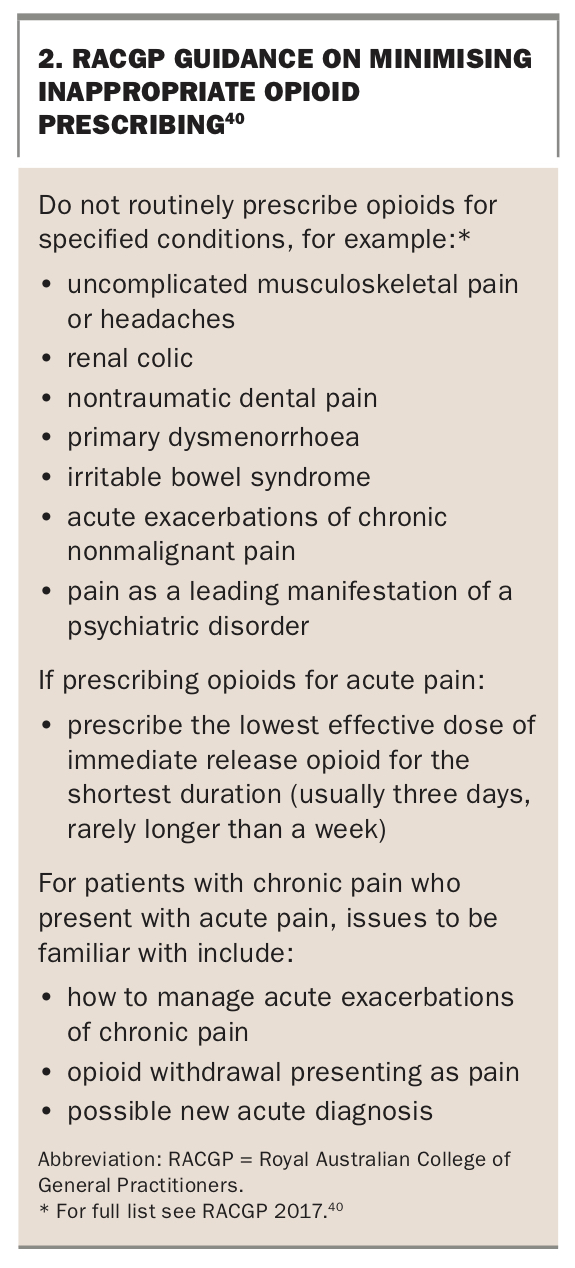
The Royal Australian College of General Practitioners (RACGP) provides guidance on how to avoid ‘unnecessary opioid prescribing’ in acute conditions and recommends that general practices adopt the approaches in Box 2.40 Acute treatment with opioids may lead to longer term problematic use, particularly in those with pre-existing SUD.14
{kind=link}
Patients taking opioid agonist therapy for SUD
In 2020, just over 53,000 Australians received OAT with methadone, buprenorphine, buprenorphine-naloxone and buprenorphine long acting injection (LAI).41 This is governed by state and territory-based legislation that often restricts dose, alterations and the prescription of other opioids, except by the registered prescriber.10 These patients should be assessed and managed in a similar way to other patients with SUD. OAT is associated with both opioid-induced hyperalgesia (influencing pain experience) and pharmacological tolerance (influencing opioid dosing should this be required, noting that relevant legislation must be considered). Communication between the practitioner treating the acute pain and the OAT prescriber is vital for optimal care.
The relationship between SUD, chronic pain and acute pain
In 2018, 3.24 million Australians reported suffering from chronic pain. Of these, one in 500 sees a specialist pain service each year.16 The remaining 499 in every 500 are managed in primary care, representing 20 to 40 per cent of all adult consultations.14 The relationship between chronic pain and SUD is bidirectional. Patients with chronic pain may display problematic medication use such as chemical coping and misuse (Table 1). Six in ten people with prescription opioid use disorder report suffering with chronic pain, often reporting that pain maintains their SUD.42 Anyone taking opioids on a regular basis has a high likelihood of pharmacological tolerance and experiencing withdrawal symptoms that may include pain (Table 2).
There is limited evidence that opioids are effective for chronic pain. Long-term opioid treatment leads not only to increased pain (probably from opioid-induced hyperalgesia), but also other adverse events,43 with four out of five patients who take opioids for at least three months experiencing related harms.33 Ceasing opioids often improves their pain experience, so opioid tapering should be considered, even when SUD is not suspected.44 The NPS MedicineWise website includes useful decision-support tools and videos to assist both opioid tapering and patient-driven goal setting and alternative chronic pain management plans.33
Self-management approaches, commonly used for other chronic conditions, help patients deal with their chronic symptoms as well as cope with pain flare-ups and even reduce their frequency.16 In some patients, an acute pain flare-up represents an opportunity (or ‘teachable moment’) to steer them toward more effective long-term approaches. However, for many the management of future flare-ups is probably best addressed when symptoms are relatively stable. Optimally, management is undertaken by the patient’s usual GP.14
If a patient with chronic pain has developed problematic drug use that meets the criteria for SUD, definitive and harm reduction treatments are indicated.16 These include staged supply, supervised dosing, engagement with the dispensing pharmacist and OAT.
When to seek advice
The RACGP recommends risk stratifying patients according to the presence of active drug use, mental illness and other comorbidities, and considering referral to a GP with advanced addiction medicine training or drug and alcohol facilities in the following cases:45
- comorbid serious psychiatric illness
- use of combinations of drugs – opioids and illicit drugs, opioids and benzodiazepines
- discharge from another general practice for ‘problematic behaviour’
- recently in a correctional facility
- high-risk behaviours.
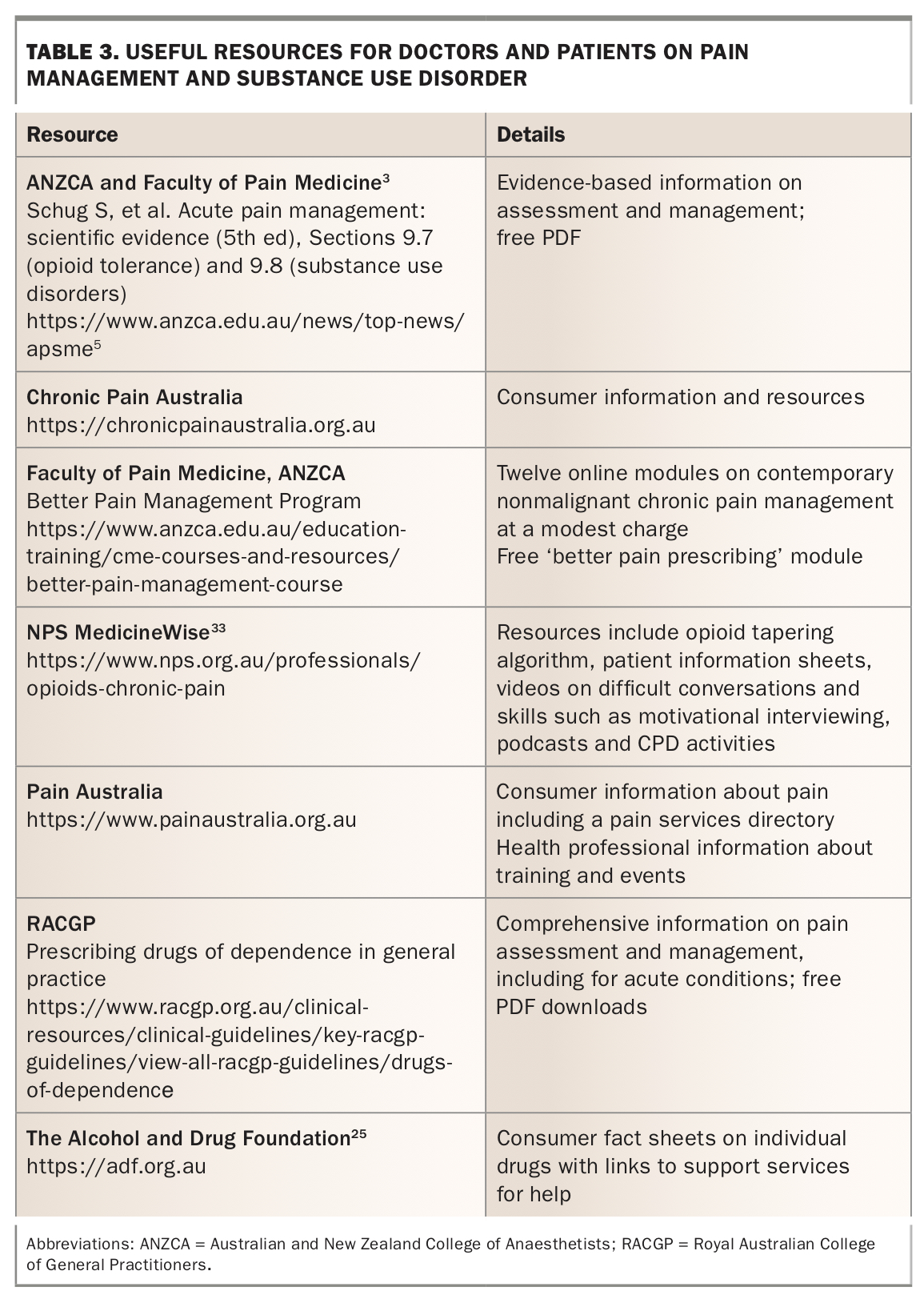
This is a significant challenge in rural and remote areas.45 All Australian states and territories have drug and alcohol clinical advisory services;10 and many organisations produce informative resources both for doctors and patients (Table 3).
{kind=link}
Conclusion
Patients with SUD who present with acute pain are challenging to assess and manage. Central to this is a nonjudgemental approach that engages the person in care. A list of Practice Points summarises the approach recommended in this article.
Although most presentations are not for serious pathology, careful assessment should exclude sinister and treatable conditions. Management can then focus on a multimodal approach, avoiding potential harm, and using first-line nonpharmacological and nonopioid treatments tailored to the individual’s situation. Opioids are required for severely painful conditions when referral for acute emergency care is planned. Otherwise, if they are prescribed this should be at the lowest dose and for the shortest reasonable duration, considering regulatory requirements. These acute presentations may present opportunities to improve chronic disease management, for example initiation of definitive treatment of SUD with OAT. MT
References
Guidelines/Drugs%20of%20dependence/Prescribing-drugs-of-dependence-in-general-practice-Part-C2.PDF (accessed August 2021).
Guidelines/Drugs%20of%20dependence/Prescribing-drugs-of-dependence-in-general-practice-Part-A.pdf (accessed August 2021).