Substance use in adolescents: if you don’t ask, they won’t tell

Adolescents presenting with substance use is increasingly commonplace. Fortunately, GPs are equally well placed to manage substance use with early intervention offering the greatest opportunity for positive behaviour change into adulthood. Effective approaches to prevention and intervention should be strengths-based, aimed at increasing protection, reducing risk factors and building resilience. Engaging the adolescent is crucial and success depends on tailoring brief interventions that are evidence-based, age appropriate and where possible, involve the family and community.
Cannabis is the most commonly used illicit drug in Australia; tobacco smoking the leading cause of preventable death; and alcohol the most common primary drug of concern, accounting for most drug-related hospital episodes in 2018.1 Equally concerning are the rising number of deaths due to methamphetamine and other stimulant use and the risk of overdose related to opioids, benzodiazepines and prescription medications.1 These are sombre statistics that tell a story of a burgeoning health crisis marked by early initiation, easy access, increasing risk-taking behaviours and polysubstance use.
The good news is that rates of tobacco smoking, regular cannabis use and drinking alcohol at harmful levels are dropping among adolescents and young people in Australia.2 Effective public health measures and a national strategy of harm minimisation for tobacco, alcohol and other drugs have demonstrated early successes across the board. However, the treatment models used over the past two decades have focused on adult substance use and addiction. Only recently have efforts shifted to investing in adolescents from a developmental science perspective, with the knowledge that early intervention in this group (aged 10 to 19 years) during a period of rapid growth, learning and adaptation will shape their long-term health trajectory. Dahl et al, in their review of adolescent health interventions, describe the distinctive attributes of learning, development and maturation during adolescence that ‘support acquisition of the culturally embodied knowledge, skills and self-regulating capacities needed to become independent and integrate into adult society’.3
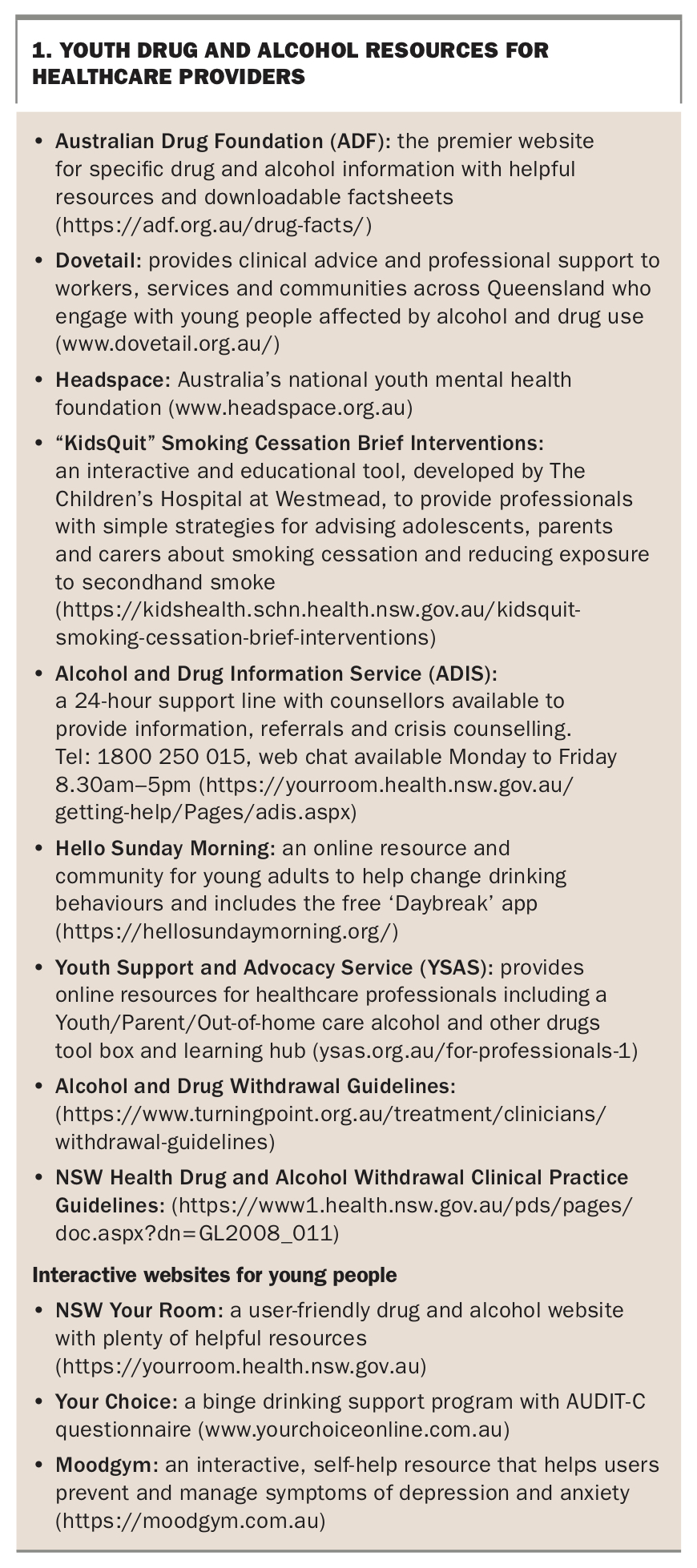
It is within this developmental context that GPs are aptly positioned to intervene early. The key message for primary care providers is to ask adolescents about their substance use and engage them early in treatment. Our own discomfort, lack of familiarity with or preconceptions of substances should not be a barrier to patients receiving appropriate care. To that end, it is important that clinicians appreciate what substances young people commonly use and how they work, that is, both their intended and unintended side effects. Box 1 provides useful drug and alcohol resources for healthcare providers.
{kind=link}
Assessment
Substance use is a spectrum that varies with an individual’s level of use and the dysfunction they experience as a result of their use. The use of alcohol and other drugs ranges from experimenting and social use (e.g. in social situations, weekends) to substance abuse, when the drug’s effects seriously interfere with health or occupational and social functioning. Continued use of psychoactive substances can lead to chemical dependency or addiction, with the inability to control use despite harmful consequences, maladaptive patterns of behaviour and features of tolerance and/or withdrawal.
Intervention is integral to elicit behavioural change. Primary intervention aims to prevent or delay the onset of alcohol and other substance use, and can take place outside of GP practices, including at school, hospitals and through community youth health services. Secondary intervention focuses on reducing problems early in the substance use spectrum and averting progression to possible substance dependence.
Setting the scene
Experimenting with alcohol and other drugs is commonplace during adolescence.1 Being conscious of this and using clear, open and nonjudgemental communication will improve your engagement with young people when talking about substance use. It is best practice to see the adolescent on their own and to establish confidentiality early in your consultation, except in exceptional circumstances such as disclosure of intention to self-harm or harm others. It may take several visits with the young person to earn their trust and, provided that they are safe, this is recommended. Parents and/or carers may present with concerns about the adolescent’s substance use. Consent to disclose information to parents/carers should be sought, unless the adolescent identifies risk of self-harm or harm to others, in which case safety planning must be developed. Building a therapeutic alliance from the start will confer positive results later and give young people the confidence to seek counsel with other sensitive health needs.
History and screening
Bridging questions are often helpful before launching into a focused drug and alcohol history, and the HEADSSS (Home, Education, Activities, Drugs, Suicidality and Sex) assessment is a good place to start.4 Ask individually about each substance group starting with tobacco, alcohol and cannabis, and progressing to drugs that are less commonly used such as amphetamines (speed, base, ice and ecstasy), cocaine, opiates, benzodiazepines, over the counter medications, inhalants and hallucinogens (such as LSD; lysergic acid diethylamide) and ketamine. Ascertain their pattern of use (e.g. daily, socially, on weekends), the age of onset and regular use, how they access drugs and quantify the amount consumed at any given time. Finally, ask the young person about when they last used and whether they have experienced symptoms of withdrawal or tolerance.
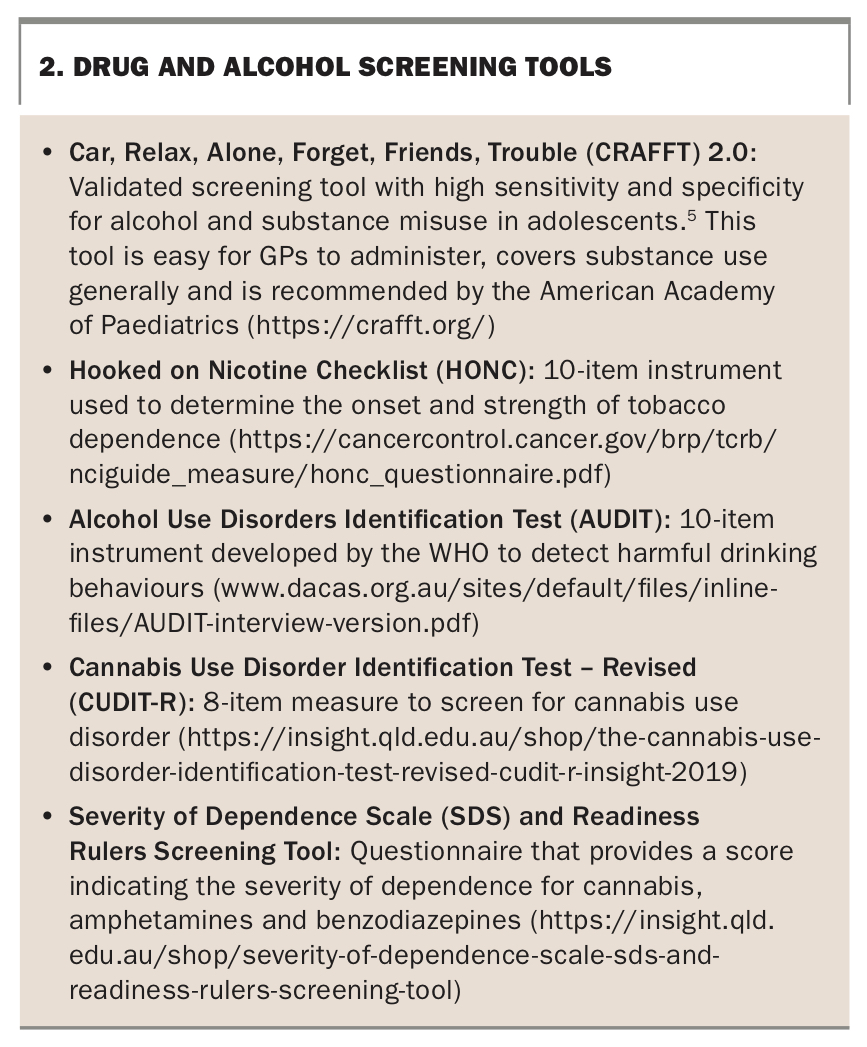
Several screening tools have been validated to identify harmful consumption of drugs and alcohol in adolescents and include the AUDIT (Alcohol Use Disorders Identification Test), CRAFFT (Car, Relax, Alone Forget, Friends, Trouble) and HONC (Hooked on Nicotine Checklist) screening tools (Box 2).5 These tools are administered via interview or are self-reported (e.g. in the waiting room of your practice) and will help to distinguish between social, problematic and dependent patterns of substance use.
{kind=link}
Mental health
It will be of no surprise to the readership that many young people who present with problematic substance use have comorbid mental health issues. Although GPs are adept at managing mental health in the community, it is particularly important to recognise the complex interplay between psychiatric disorders, substance use and access to both prescription and illicit drugs. Young people with neurodevelopmental disorders such as attention deficit hyperactivity disorder, oppositional defiant disorder, conduct disorder and mood disorder have a higher risk of problematic substance use and disproportionally present to youth drug and alcohol services.6 Although outside the scope of this review, addressing specific management of these comorbidities will improve outcomes, and referral to community mental health and paediatric services for assessment and intervention is recommended.
Risk assessment
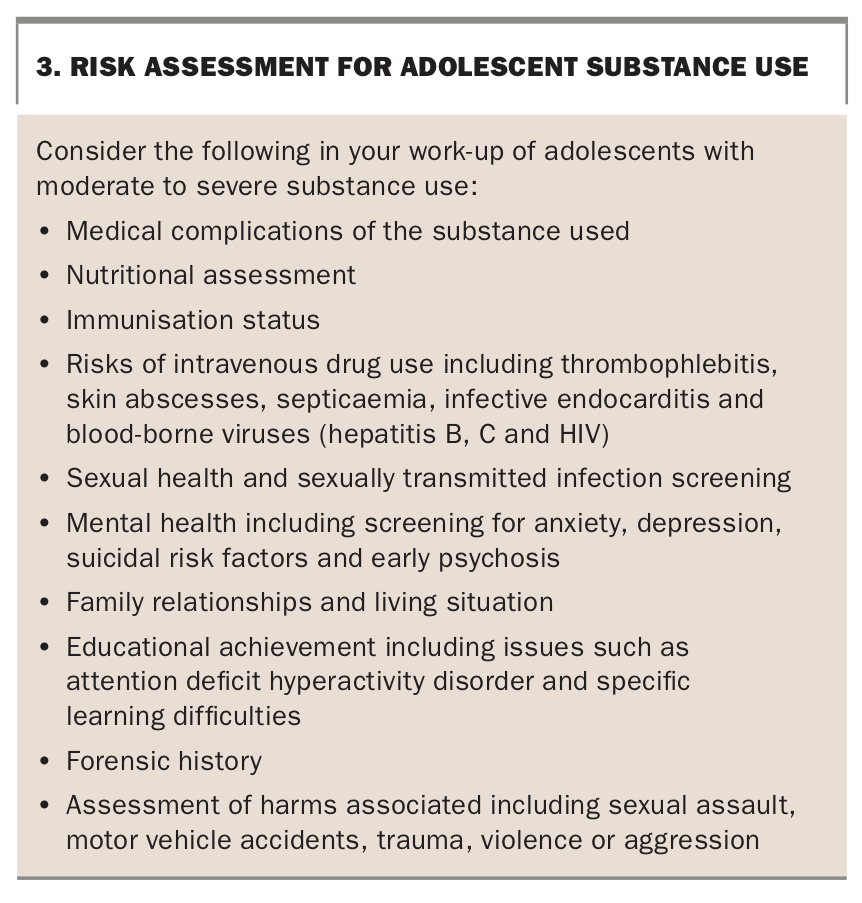
A comprehensive assessment including risk assessment (Box 3) should be performed for all adolescents and young adults presenting with substance use. Vulnerable young people, including those who are homeless or in out-of-home care; in the criminal justice system; victims of violence, child abuse or neglect; or those not engaging in work or education are particularly prone to substance use. When assessing the patient, consider age of first substance use, ease of access, parental supervision, safety of the young person and harms associated with specific substances.
{kind=link}
Adolescents who are in out-of-home care, or case managed by social services, nongovernment organisations or other youth agencies, add a further degree of complexity when trying to co-ordinate their care. Fostering interagency collaboration is crucial to ensure that the needs of the adolescent are met and treatment plans are followed. Missed appointments, unfilled prescriptions and frequent presentations to acute mental health and emergency services should raise concern. Additionally, some adolescents engage in risky or criminal activity, including unwanted or unsafe sexual activities associated with substance use. GPs and other healthcare providers are mandatory reporters for child protection concerns and need to be acutely aware of the child-at-risk reporting framework and the local guidance for the state or territory in which they practise.
Treatment principles
Adolescence is an opportune time for early intervention for issues related to alcohol and other substance use. The goals of assessment are to identify the harms and comorbidities associated with substance use and to formulate a treatment plan that is unique to the needs of the adolescent. Provision of evidence-based behavioural interventions, addressing child protection concerns and delivering care in a trauma informed manner are key treatment principles that GPs are well-equipped to perform.
Brief interventions
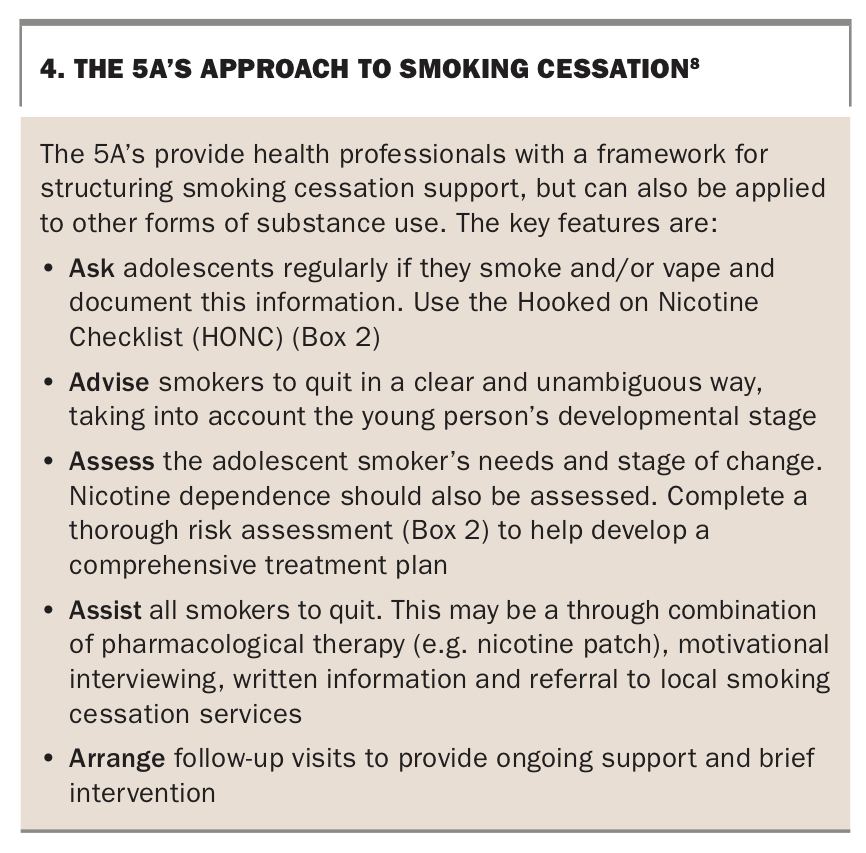
Brief interventions offer GPs the most value in influencing positive behaviour change and reducing harmful use.7 When successfully applied, a brief intervention is opportunistic, revisited at every contact and consists of informal counselling and drug psychoeducation. It is most appropriate early in substance use to reduce harmful consumption but can also be applied later to achieve harm reduction for individuals who are chronically using or drug dependent. Examples of brief interventions that are easy to follow include the 5A’s (ask, advise, assess, assist, arrange) approach (Box 4) and FRAMES (feedback of personal risk/impairment, responsibility, advice, menu, empathy, self-efficacy) (Box 5) model, and although specific to tobacco and alcohol, respectively, can be applied generally to other substances.8,9
{kind=link}
{kind=link}
Motivational interviewing/Motivational enhancement therapy
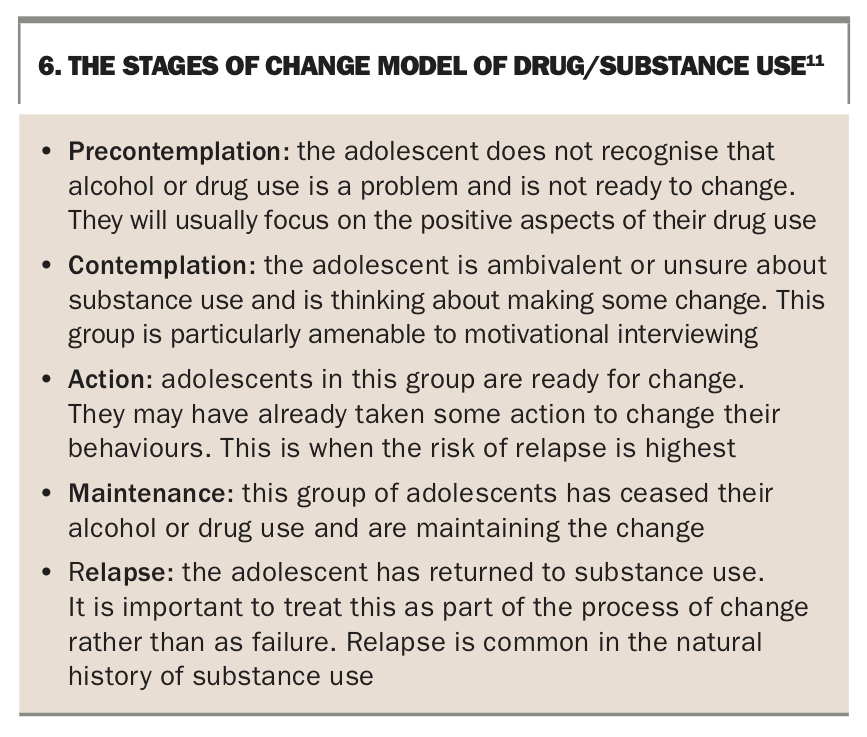
Motivational interviewing and enhancement therapy models are based on the assumption that ambivalence about substance use (and change) is normal and can be resolved by working with the person’s intrinsic motivations and values.10 A significant part of drug and alcohol assessment and intervention is understanding where the adolescent sits with regard to wanting to change their drug use (Box 6)11 and adopting an empathetic yet directive counselling style to provide conditions under which change can occur. We are mindful that the effect of this intervention is somewhat influenced by the developmental age of the adolescent and their capacity to make changes, particularly if there are issues related to substance use in their family and community. Younger adolescents are more likely to require additional supportive social and family systems (including parental/carer supervision) to assist with making changes.
{kind=link}
Harm minimisation
It is important to consider the actual harms associated with the use of a particular drug and how these harms can be reduced for the individual and society. This can include individual and physical harms (such as overdose, accident or injury associated with substance use) and impact on our society (such as increased criminal activity associated with substance use). A harm minimisation approach does not insist on abstinence as the only objective of treatment but on reducing the risks associated with substance use. Some examples of harm minimisation include educating young people on strategies to reduce harms from alcohol consumption, party safe campaigns and needle exchange programs to reduce risk of harms associated with intravenous drug use.
Individual cognitive behavioural therapy
Cognitive behavioural therapy is an evidence-based treatment approach for young people who present with substance use.12 Referral to psychosocial services that offer cognitive behavioural therapy and/or online modules (Box 1) will generally focus on emotion regulation and impulse control and entail the following:
- relaxation techniques
- anxiety management
- managing cravings
- relapse prevention
- counselling
- substituting substance use with healthier options
- spiritual fulfilment.
Family therapy
Family therapy has proven efficacy for adolescents with substance use problems by focusing on close relationships and validating the experience of all family members. Involving parents in treatment indirectly assists the adolescent by addressing parental concerns, influencing parenting style, building capacity and breaking unhealthy patterns of communication and interactions.13
Pharmacotherapy
Pharmacotherapy refers to the use of medications in substance abuse treatment in addition to other therapies mentioned. More commonly, medications are used to manage comorbid mental health issues, for the short-term alleviation of withdrawal symptoms and for patients at the more severe end of the substance use spectrum. Examples include nicotine replacement therapy for young people who are nicotine dependent, or medications such as acamprosate for chronic alcohol abuse. Our experience suggests that adolescents are more likely to benefit from pharmacological treatments when used adjunctively with individual and family interventions, and starting therapy is often a case-by-case decision. Medication to assist with withdrawal symptoms for the short term may be considered.
Tertiary intervention
Tertiary intervention strategies are aimed at achieving abstinence and reducing harm for young people at the severe end of the substance use spectrum. This intensive intervention requires referral to youth drug and alcohol services and adopts an assertive case management approach. Residential rehabilitation falls under this category and programs are specifically targeted to assist with breaking the cycle of drug use, re-engaging the young person in school, education or employment and promoting healthy social supports.
Conclusion
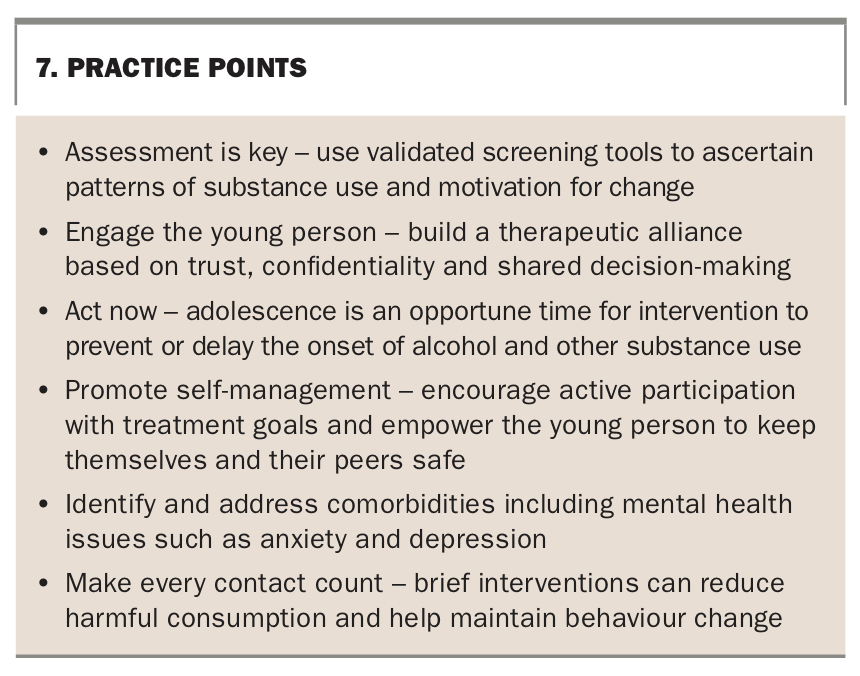
Investing in adolescents offers the greatest opportunity for positive behaviour change and successful attainment in adulthood. To do this well, we need to recognise the distinct developmental changes of adolescence, when this occurs and how their changing social roles and identity affect their learning and behaviours. The issue of substance use by adolescence is no different – ask the question, understand the problem and target treatments that are tailored to their needs (Box 7). Prevention and early intervention for adolescents with substance use offers the best chance to intercept that pivotal inflection point, when habits are formed and behaviours can change. MT
{kind=link}
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.