Assessment of male infertility in primary care

Couples who have not conceived within 12 months should be assessed for infertility. Male factor causes of infertility are an important part of this assessment. History taking and clinical examination are key to identifying biological and environmental causes of male factor infertility, which include altered spermatogenesis, obstructive azoospermia, hypogonadotrophic hypogonadism and disorders of intercourse or ejaculation.
Up to 85% of couples attempting conception achieve pregnancy within the first six to 12 months. Assessment for infertility is recommended for couples who have not conceived after 12 months (and within six months for those with secondary factors affecting fertility).
Infertility should be assessed as a couple’s issue, and consideration of possible male factor infertility is essential, as it is solely responsible for subfertility in 30% of couples and a significant contributor in a further 20% of couples. Diagnosis and appropriate management of male factor infertility allows most men to have biological children.
Causes of male factor infertility
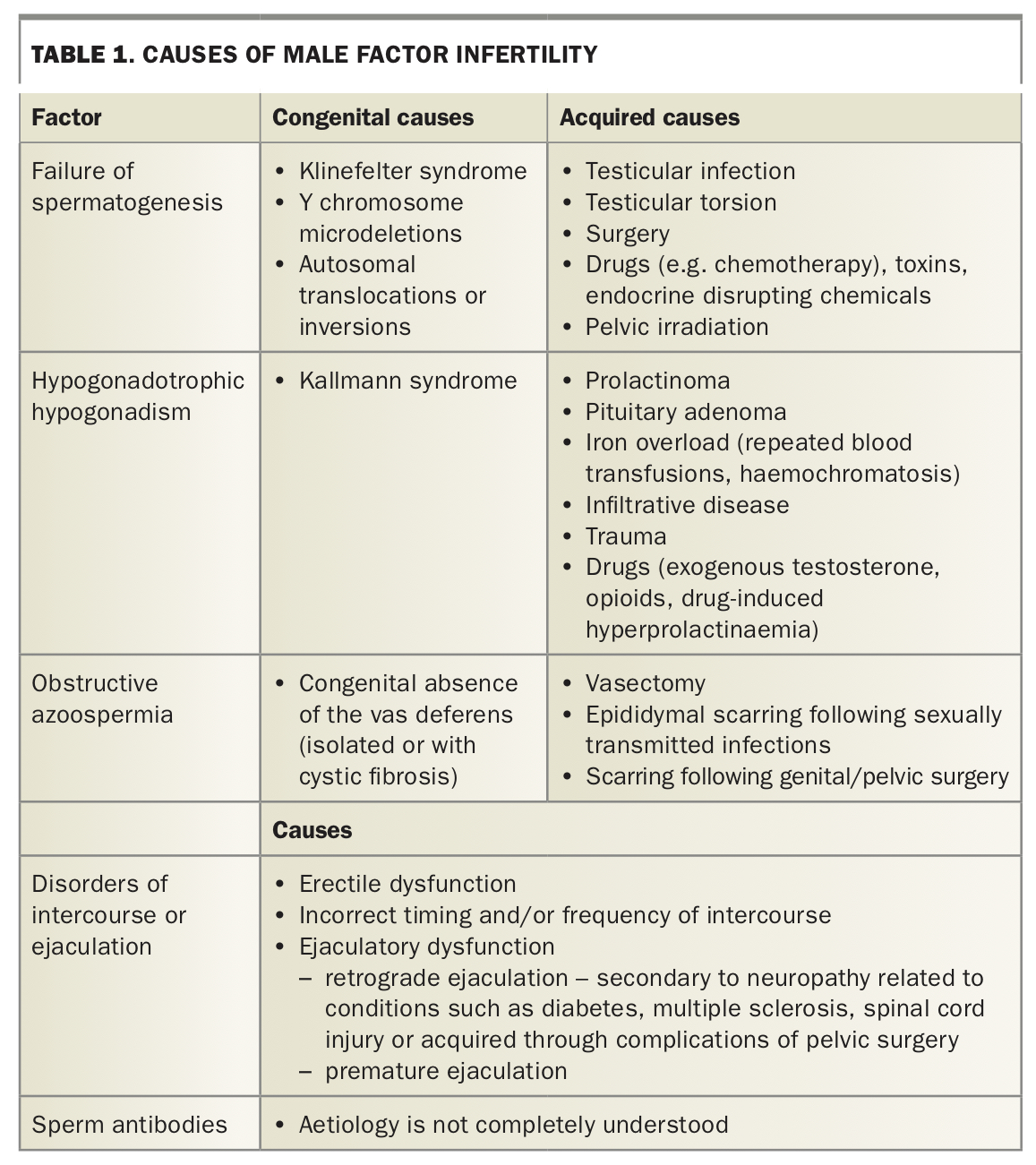
Male fertility can be affected by a multitude of factors, both biological and environmental. Optimal development of the male reproductive system relies on a number of processes that play out across fetal life, puberty and adulthood. These include the hormonal interplay between the hypothalamic-pituitary-testicular axis and appropriate testicular structure and function, especially the complex germ cell differentiation termed spermatogenesis. Potential causes of male infertility are listed in Table 1.
{kind=link}
Around 60% of male factor infertility is caused by impairment or failure of spermatogenesis. In most cases, no cause is found (idiopathic) but thorough patient review will identify specific causes important for proper counselling and management. These include genetic causes such as Klinefelter syndrome and Y chromosome microdeletions. Klinefelter syndrome is the most common chromosomal disorder affecting men and accounts for around one in seven cases of spermatogenic failure and azoospermia. It affects up to one in 500 men, although it remains undiagnosed in most cases. Acquired causes of impaired spermatogenesis include testicular injury from infection, orchitis, testicular torsion, or toxicity secondary to chemotherapy or radiation therapy.
Obstructive azoospermia results from obstruction of sperm outflow from the testis and occurs in around 30% of infertile men. This includes in men who have a congenital absence of the vas deferens associated with mutations of the cystic fibrosis transmembrane conductance regulator (CFTR) gene. Acquired causes include having a vasectomy or after infection or surgery at the bladder base. Other causes of infertility include failure to have timed ejaculatory intercourse and, in a minority of cases, endocrine causes such as prolactinoma or hypogonadotrophic hypogonadism.
Clinical evaluation
History
Assessment of male fertility begins with comprehensive history taking and examination. A woman’s age is the most important factor affecting pregnancy rates in couples. Similarly, age is also an important factor in men, with partners of men aged over 45 years having higher rates of miscarriage and longer time to conception. Taking a fertility history is important and includes asking questions about previous successful conception, duration of infertility and previous contraceptive use.
In addition to taking a general medical history, a targeted history for testicular or genitourinary problems is essential. This includes cryptorchidism, testicular cancer, testicular torsion and other testicular trauma, as well as previous vasectomy and pelvic or genital surgery. Sexually transmitted infections such as chlamydia and gonorrhoea may cause obstruction within the reproductive tract, especially if untreated, resulting in reduced fertility. Similarly, postpubertal mumps orchitis can cause severe spermatogenic failure – the key reason to ensure that adult men are vaccinated – and prostatitis, which may damage the reproductive tract or contribute to obstructive azoospermia.
Obesity is a significant contributor to male infertility through multiple mechanisms, including hormonal dysregulation, impact on sperm quality, reduced libido and erectile dysfunction. Excess weight can result in a relative excess in oestrogen levels and suppression the of hypothalamic-pituitary-testicular axis, leading to suppression of gonadotrophin releasing hormone and gonadotrophins, and subsequent reduction in serum testosterone levels. Counselling patients on the benefits of weight loss with regard to infertility through dietary intervention and regular moderate-intensity exercise is important for affected couples.
Identifying comorbidities such as iron deposition diseases (e.g. haemochromatosis and transfusion-dependent thalassaemia) is important and may direct subsequent assessment. Additionally, a family history of infertility is pertinent and may suggest an underlying inheritable factor.
Taking a coital history is important to elucidate the presence of sexual dysfunction as well as the adequacy of intercourse for conception, including frequency and timing. Couples should be advised to engage in sexual intercourse regularly (at least every second day) around the time of ovulation. Factors such as low libido, erectile dysfunction or retrograde ejaculation may prevent effective intercourse and thus impact on the likelihood of natural conception. Evaluation of cardiovascular risk factors, risk factors for neuropathy (e.g. diabetes) and clinical symptoms of hypogonadism should be considered.
Exposure to tobacco, alcohol, exogenous androgens and recreational drugs are also important factors in assessing male infertility. Tobacco smoking contributes to reduced sperm production and quality and may cause epigenetic changes in sperm, which has the potential to affect offspring.1 Excessive alcohol consumption has been associated with reduced sperm quality, hypogonadism and sexual dysfunction. Use of recreational drugs such as cannabis may impact sperm quality and, potentially, sexual function through effects on cannabinoid receptors in the hypothalamus.2,3
Exogenous androgens, including routine testosterone replacement therapy, suppress gonadotrophins and spermatogenesis. In the context of androgen misuse by eugonadal men, gonadotrophin and endogenous testosterone secretion and spermatogenesis are usually restored six to 12 months after androgen withdrawal, depending on the formulation and dose of androgen and duration of prior exposure.4 Importantly, testosterone therapy is contraindicated in androgen-deficient men desiring fertility treatment, even those who are symptomatic, because it will likely eliminate residual sperm production. In such cases, a fertility solution should be sought (e.g. by sperm storage or assisted reproductive technology) before testosterone therapy is started or considered. In men who are being managed with testosterone replacement therapy for hypogonadism, testosterone therapy will likely need to be stopped.
Lastly, exposure to endocrine-disrupting chemicals has increasingly been shown to have an adverse impact on fertility. These chemicals are found in certain plastics and pesticides and may contribute to reduced sperm quality and changes in reproductive hormone levels in young men.5
Clinical examination
General examination should include cardiovascular evaluation, assessment of body mass index and measurement of blood pressure. Counselling on lifestyle or more intensive intervention may be guided by these findings.
Clinical examination should assess for degree of virilisation and signs of androgen deficiency such as gynaecomastia. Genital examination is an integral component of clinical examination. This should include testicular volume measurement with the use of an orchidometer, as well as palpation for the vasa and scrotal masses. Information on clinical examination and other useful resources for both health professionals and men wanting further information on men’s health and fertility can be found on The Healthy Male (previously Andrology Australia) website (Box 1).
{kind=link}
Semen analysis
Semen analysis is the key investigation for assessment of male fertility and should be performed at a laboratory that complies with standards described in the WHO laboratory manual for the examination and processing of human semen.6 Men should be advised to abstain for two to seven days before collection and provide a sample onsite if possible. The sample should be evaluated within an hour of production. Care should be taken to ensure the sample does not deteriorate during transport due to lapse in time and changes in temperature. The first part of the ejaculate has a high concentration of sperm and therefore it is crucial that the whole sample is collected in order to retrieve an accurate sperm count. It is also important to ensure that the man is not unwell at the time of collection, as intercurrent febrile illness can have a significant impact on semen parameters. Because of variability between specimens, a subnormal semen analysis result should be confirmed with a repeat sample at least six weeks after the first collection. An algorithm for semen analysis is presented in the Flowchart.
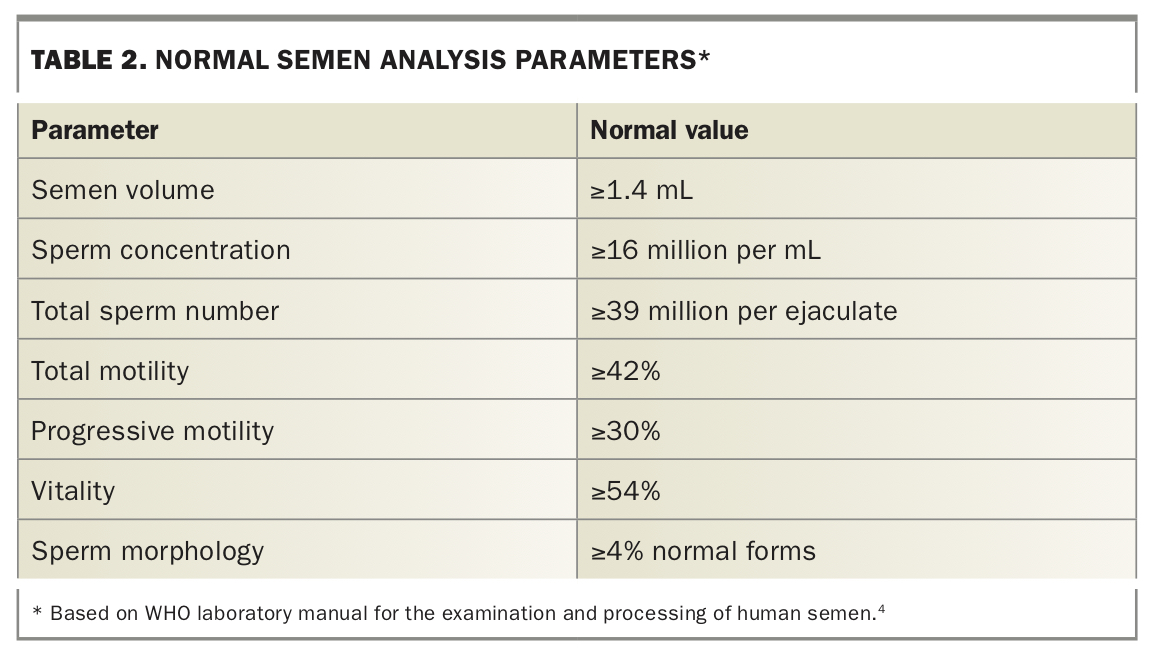
A semen analysis provides information on semen volume and sperm concentration, total number, motility (progressive and total) and morphology. It may also include information on sperm vitality, semen pH and the presence of sperm antibodies. The reference interval (fifth percentile of fertile men) values as defined by the WHO are outlined in Table 2.6 These values provide some guidance as to the chance of conception, for example, spontaneous conception over a two-year period occurs in around 30% of couples when the man has a sperm density of 1 to 5 million per mL and the woman is healthy. It is important to recognise that they should not be interpreted as ‘fertility cut off values’.
{kind=link}
Blood tests
Blood tests provide useful adjunctive information to semen analysis, with investigations being directed by history, clinical examination and semen analysis. Endocrine testing should include a morning fasting blood test for serum luteinising hormone, follicle stimulating hormone (FSH), total testosterone and prolactin levels. Serum gonadotrophin levels can differentiate between testicular failure and hypothalamic-pituitary dysfunction. Primary testicular failure is suggested by a low serum total testosterone level accompanied by elevated gonadotrophin levels. In contrast, secondary testicular failure is suggested by a low serum total testosterone level with low or inappropriately normal gonadotrophin levels. In the latter situation, further assessment of the pituitary may be indicated, including assessment of pituitary hormone function as well as pituitary MRI. Serum prolactin and thyroid function testing may reveal endocrine abnormalities that can be treated, with subsequent restoration of fertility. Hypogonadotrophic hypogonadism can be treated with gonadotrophin therapy, including human chorionic gonadotrophin (hCG) with or without FSH, although it may take up to two years to induce spermatogenesis.7 The only available version of hCG in Australia is not PBS listed for men. However, follicle stimulating hormone is PBS listed for men who are still azoospermic after six months of hCG use.
Genetic testing should be considered for men with idiopathic primary testicular failure, including karyotype testing and Y chromosome microdeletion testing for men with azoospermia or sperm concentration less than 5 million/mL. Identification of a Y chromosome microdeletion would provide a cause for male infertility, while the type of microdeletion may predict the likelihood of successful sperm extraction.8
In the setting of azoospermia, a normal serum FSH level is suggestive of obstructive azoospermia. In men with suspected obstructive azoospermia, testing for a CFTR gene mutation should be considered because of its association with bilateral congenital absence of the vas deferens.9 Importantly, obstructive azoospermia can occur without clinical manifestations of cystic fibrosis and in heterozygotic carriers. Identifying this gene mutation is important for genetic counselling as it may be inherited by offspring. In men with obstructive azoospermia, sperm can usually be harvested by testicular biopsy, and may then be used in IVF treatment to fertilise the egg via intra-cytoplasmic sperm injection (ICSI). In men with acquired obstructive azoospermia, microsurgical repair of the ejaculatory structures can be attempted, but is often not necessary.
Other Investigations
Scrotal ultrasound may be indicated to confirm abnormal clinical genital examination findings or in those with a history of undescended testes, as testicular cancer may be present in this population in the absence of palpable abnormalities. Findings from a scrotal ultrasound may include identification of clinically significant varicoceles, which can contribute to oligospermia.
A testicular biopsy will distinguish between obstructive (normal spermatogenesis) and nonobstructive azoospermia (NOA, severe primary spermatogenic failure). Microdissection testicular sperm extraction (microTESE), which involves detailed surgical dissection of the testes, is both a diagnostic and therapeutic procedure in men with NOA. MicroTESE allows retrieval of sperm in a significant proportion of men with NOA, and any harvested sperm can subsequently be used for ICSI.
Conclusion
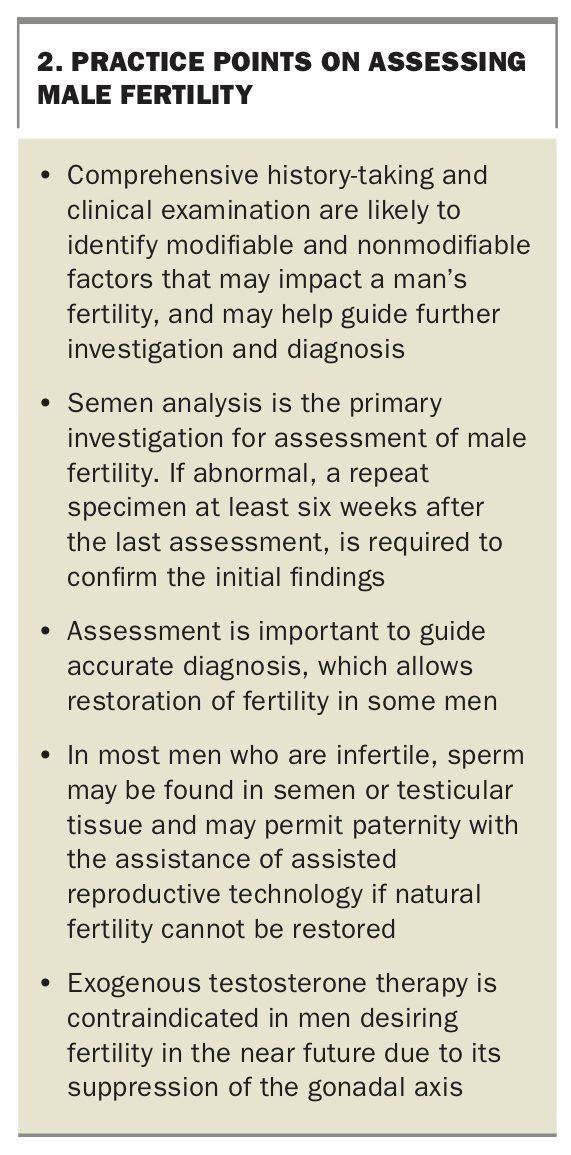
Male factor infertility is an important contributor to fertility and should not be overlooked as part of assessment of a couple’s fertility. GPs can help identify male factor infertility through history taking and assessment, and are well placed to offer counselling. Practice points on assessing male fertility are summarised in Box 2. MT
{kind=link}