Viral exanthems: unravelling viral rashes

Common causes of viral exanthems in Australia include herpesviruses, enteroviruses, parvovirus B19, varicella, measles and rubella viruses and mosquito-borne alphaviruses. The cause can often be diagnosed clinically from the rash distribution and morphology, confirmed only when necessary with serological or PCR tests. Most viral exanthems are self-limiting, requiring supportive care alone.
- Viral exanthems are common, and detailed history taking and examination of the morphology and distribution of the rash are essential to determine the cause.
- Viral exanthems such as varicella and rubella can cause significant complications in pregnant women, so early diagnosis and treatment are key.
- Viral exanthems can be diagnosed clinically, and clinicians should think critically before ordering molecular and serological testing.
- Certain viral exanthems, such as Ross River virus disease, must be notified to the appropriate public health unit as per state or territory guidelines.
- High vaccination rates are crucial to reduce the incidence and morbidity of viral exanthems such as measles.
Viral exanthems in children and adults are a common presentation to GPs. Viral exanthems can be triggered directly by an infectious pathogen (infectious exanthem) or indirectly by an immune response (parainfectious exanthem).1 Although some viral exanthems are benign and self-limiting, early diagnosis is paramount in patients with severe systemic infection and in those who are pregnant, immunocompromised or require time off work or school, and before immunisation.2 The diverse morphologies of viral exanthems can be a diagnostic challenge. Knowledge of the different patterns of viral rashes and their epidemiology are crucial to identifying their aetiology.
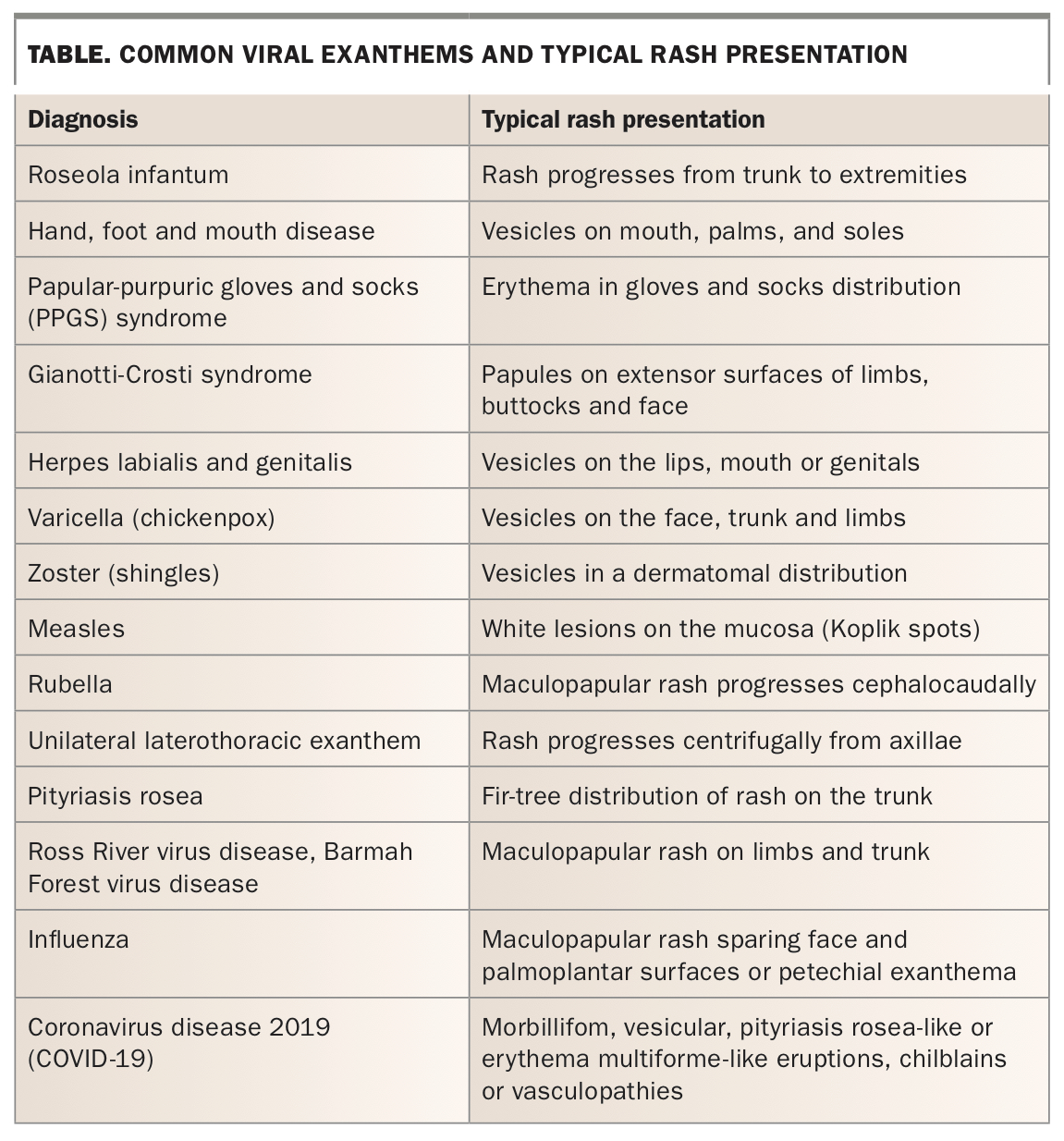
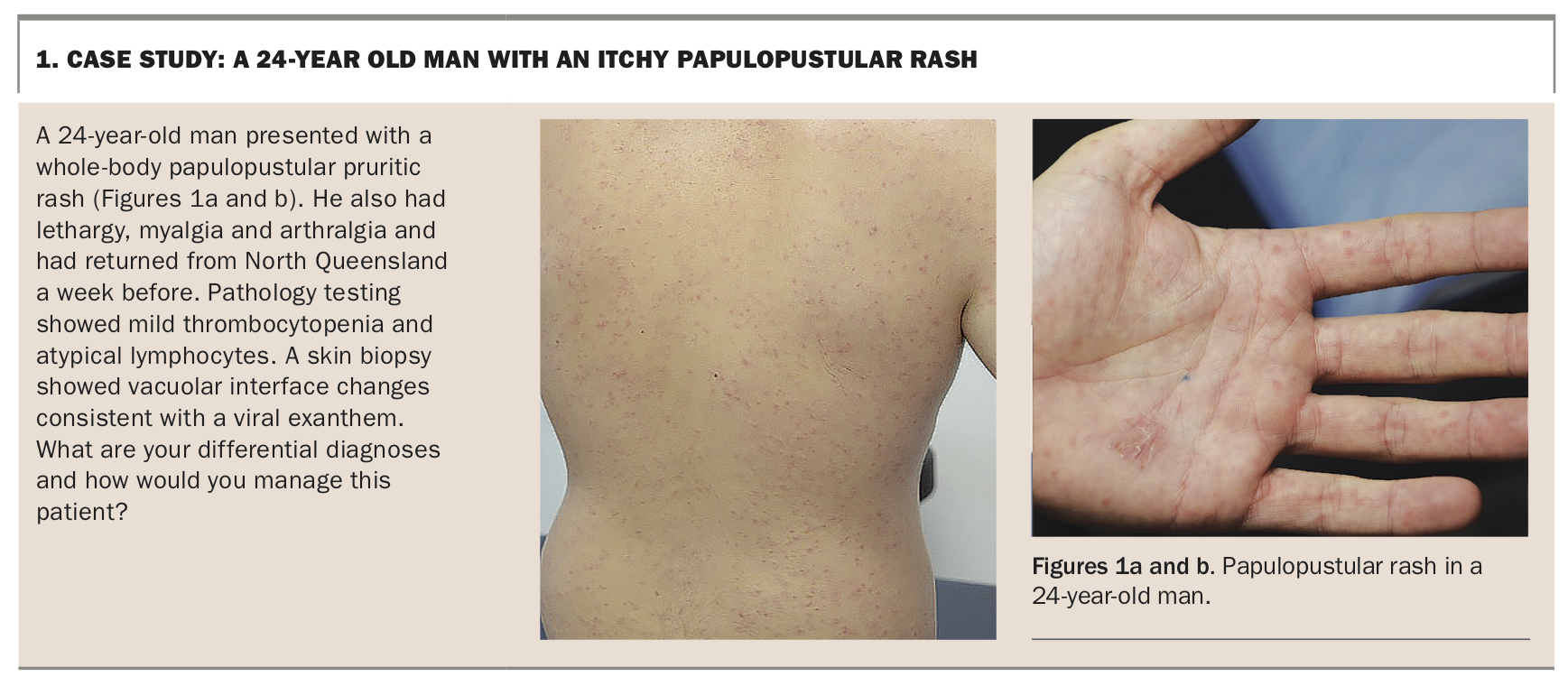
In this article, we provide a diagnostic framework for viral exanthems based on the rash distribution and morphology (summarised in the Table). However, it should be noted that the different viral exanthems are not limited to any particular distribution or morphology. Further, presentations can be atypical, especially in patients who are vaccinated or immunocompromised. We also outline the common causes, investigations and management of viral exanthems. A case study of a viral exanthem is outlined in Box 1.
{kind=link}
{kind=link}
How to differentiate viral and nonviral exanthems
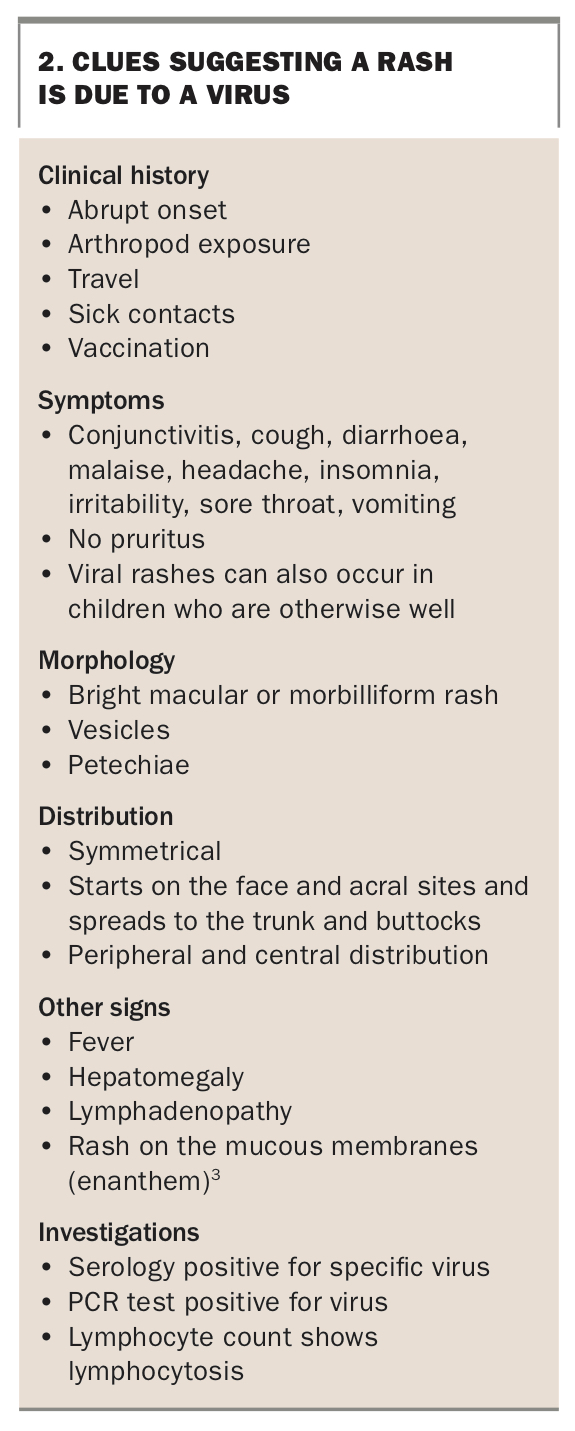
Viral and nonviral exanthems have some distinguishing features. However, identifying the cause can be difficult as viral rashes can be a ‘great imitator’ for other diseases, and presentations can be atypical. Clues that suggest a rash is viral are listed in Box 2.3 Differential diagnoses that should be considered include systemic adverse reactions to drugs, bacterial toxins, malignancy, allergic contact dermatitis and other diseases.4
{kind=link}
Although many viral exanthems in children are accompanied by coryzal symptoms, the diagnosis can generally be made clinically. Before ordering respiratory viral tests, clinicians should critically assess the need for them, considering issues such as their clinical utility, accuracy and finite resources.5 Similarly, clinicians should think critically before ordering molecular and serological testing.
Rash progressing from trunk to extremities - roseola infantum
Roseola infantum (exanthema subitum, sixth disease) is a benign, febrile exanthem of childhood caused by human herpesviruses (HHV) 6 and 7. HHV-6 and HHV-7 are ubiquitous among humans, and nearly 100% of the population is infected by the age of 3 years. Primary infection often manifests as a mild illness, sometimes even asymptomatic. HHV-6 and HHV-7 are transmitted by salivary contact and via the placenta.6
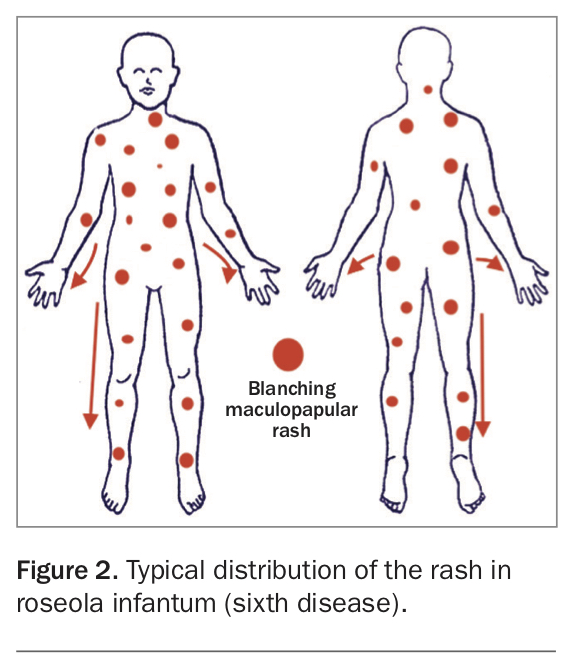
Roseola infantum starts with a high fever lasting three to seven days. After the fever subsides, a faint, rose pink, blanching skin eruption appears suddenly. Discrete, irregular, circular or elliptical macules or papules occur on the neck and trunk and can spread to the face and extremities (Figure 2). The rash lasts one to two days. Diarrhoea, upper respiratory symptoms and cervical lymphadenopathy can develop. Febrile seizures, hepatitis and encephalitis are rare sequelae.
{kind=link}
Recognition of the distinctive clinical course is usually sufficient for diagnosis of roseola infantum. However, the gold standard for diagnosis is the detection of seroconversion and actively replicating HHV-6 or HHV-7 in peripheral blood through culture. PCR testing of body fluids and tissues can also be used to detect viral DNA and quantify viral load.
Roseola infantum is self-limiting, and supportive care involves antipyretics and maintenance of hydration. Antivirals can be effective in immunocompromised children.4
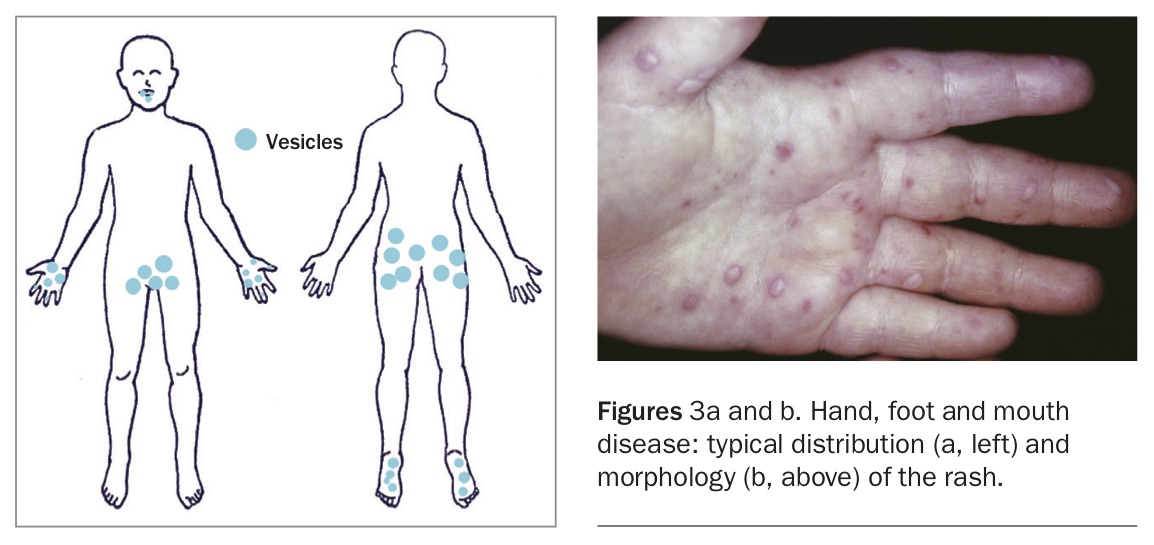
Vesicles on mouth, palms and soles - hand, foot and mouth disease
Hand, foot and mouth disease (HFMD) is the most common manifestation of human enterovirus infection. It is usually caused by coxsackievirus A6 or A16 or enterovirus 71. HFMD should not be confused with foot and mouth disease, which affects cattle, sheep and pigs. HFMD mostly affects children younger than 5 years and has a peak incidence in summer. HFMD is spread by the faecal-oral or oral-oral routes, and outbreaks are common in childcare centres.
Patients with HFMD usually have a prodrome of fever, malaise, coryza, reduced appetite and sore mouth occurring one to two days before the rash. Classic HFMD presents as a localised eruption of vesicles and painful ulcerations in the oral cavity, followed by erythema and pruritic greyish vesicles on the digits, palms, soles, buttocks and genital area (Figures 3a and b). Atypical HFMD has been reported, with a widespread vesiculobullous and erosive eruption favouring the perioral, acral and buttock regions. Enterovirus infection with a fulminant course has also been noted to cause acute flaccid paralysis in South East Asia and Australia.4
{kind=link}
Enteroviral exanthems can usually be diagnosed clinically, but the differential diagnoses of erosive or bullous disorders and eczema herpeticum in children must be considered in atypical presentations. Diagnosis can be confirmed by PCR testing of blister fluid, throat swabs and stool samples.
The rash of HFMD can last days to weeks. Treatment is supportive, including rehydration and pain relief for sore throat, such as salt water gargles, mouthwashes or throat lozenges that do not contain benzocaine for children aged over 6 years.7 Avoiding fruit juices high in acid such as orange juice and lemonade can minimise irritation of mouth sores.8
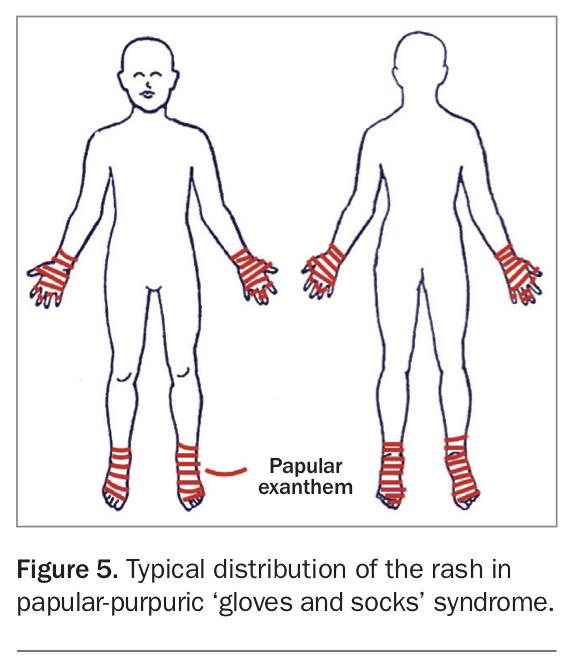
Erythema in gloves and socks distribution - papular-purpuric gloves and socks syndrome
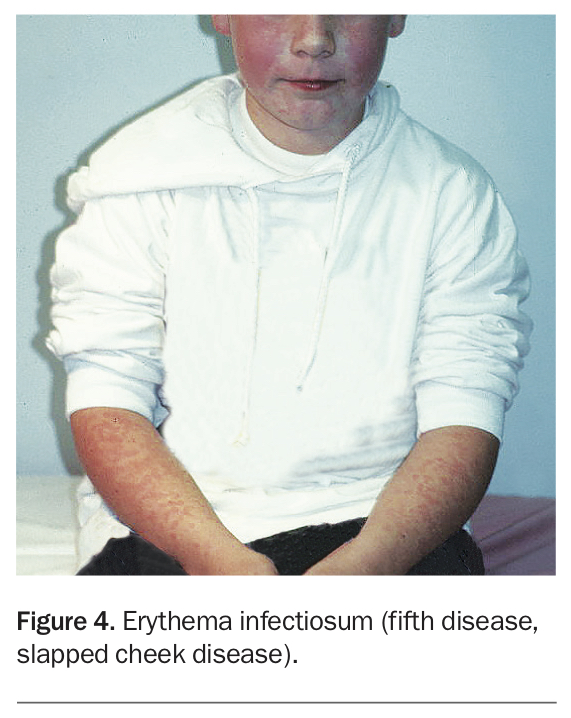
Parvovirus B19 infection is associated with several exanthems, including erythema infectiosum (also known as fifth disease or slapped cheek disease, Figure 4) and papular-purpuric ‘gloves and socks’ syndrome (PPGSS). PPGSS mainly affects adolescent girls and young adults. It is contagious during the exanthem stage and can be transmitted via respiratory droplets, blood products and in utero.
{kind=link}
The rash in PPGSS is typically a pruritic, burning, intensely erythematous, papular exanthem on the hands and feet that is sharply demarcated at the wrists and ankles (Figure 5).9 Oedema can limit hand mobility. The oral mucosa can be involved, with vesicles, erosions and aphthous ulcers. Systemic manifestations include fever, lymphadenopathy and arthralgia.
{kind=link}
The diagnosis of PPGSS is based on the clinical presentation. Differential diagnoses include urticaria, Kawasaki disease, idiopathic palmoplantar hidradenitis and early stage vasculitis. PPGSS is generally self-limiting and resolves spontaneously in one to two weeks. Symptomatic treatment is recommended, such as adequate rest and maintenance of hydration.7
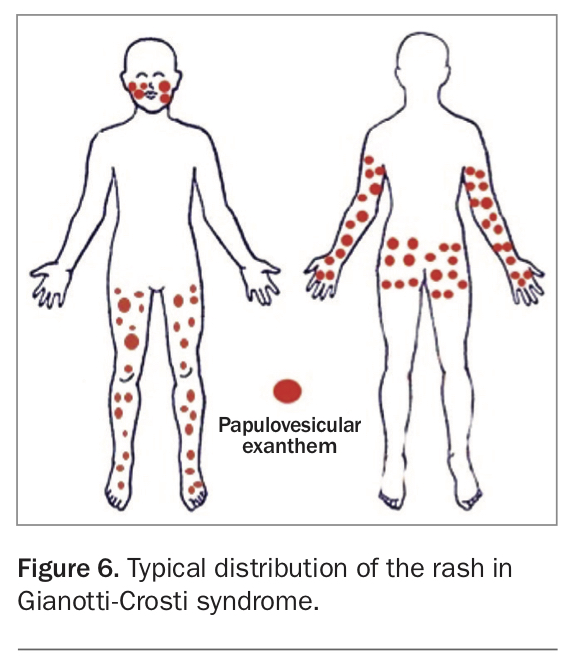
Papules on extensor surfaces of limbs, buttocks and face - Gianotti-Crosti syndrome
Gianotti-Crosti syndrome, also known as papular acrodermatitis of childhood, is a parainfectious exanthem. It is associated with a range of viruses, including hepatitis B virus, cytomegalovirus, Epstein-Barr virus, enterovirus, parvovirus B19 and HHV-6.10 It has also been seen after hepatitis B vaccination.11
Gianotti-Crosti syndrome usually manifests in children aged between one and six years as an asymmetrical papular or papulovesicular exanthem on the cheeks, extensor surfaces of limbs and buttocks (Figure 6). Patients can also have a prodrome of fever and upper respiratory tract symptoms. There is no associated pruritus, hepatitis or lymphadenopathy.
{kind=link}
The diagnosis of Gianotti-Crosti syndrome is clinical, and many children do not require specific tests; however, a skin biopsy may be required in challenging cases. Differential diagnoses to be excluded include atopic dermatitis, drug-induced exanthem, lichen planus and Henoch-Schonlein purpura. Hepatitis serology should be assessed in patients who are not vaccinated against hepatitis B. A specific diagnosis is reassuring to parents, as the intensity of the rash in Gianotti-Crosti syndrome can be alarming.12
Gianotti-Crosti syndrome resolves over three to four weeks. Treatment is supportive.
Vesicles on lips, mouth or genitals - herpes labialis and genitalis
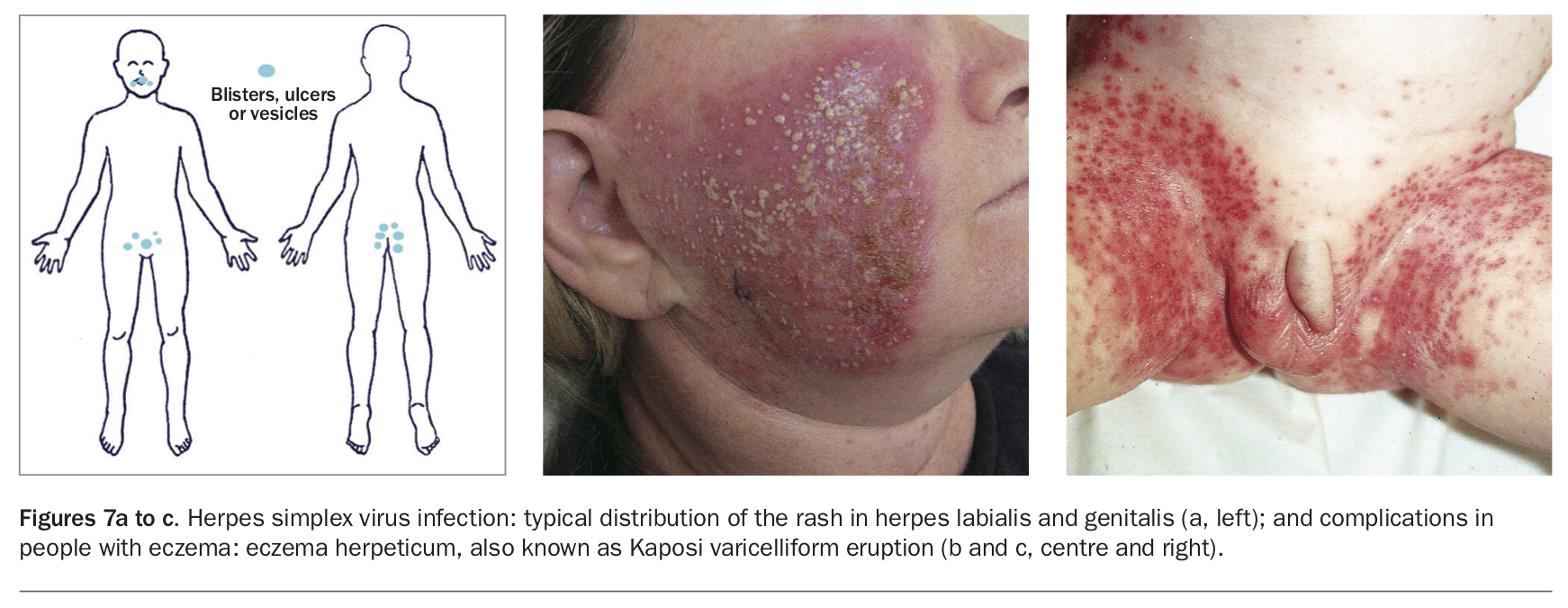
Herpes labialis and genitalis are caused by herpes simplex virus (HSV) type 1 and type 2. These viruses infect through direct contact of mucosal surfaces or abraded skin. The viruses become latent in the dorsal root ganglia for an indefinite period and can reactivate and multiply at the nerve root, then travel through the nerve to the skin or mucous membrane. HSV-1 usually causes herpes labialis, and primary infection occurs during childhood or adolescence.13 Genital HSV is transmitted in most cases during periods of asymptomatic viral shedding. A prodrome of localised pain, tingling, burning, tenderness, paraesthesia, lymphadenopathy, headache, fever, anorexia or malaise precedes lesion formation by hours to days.
HSV-1 and HSV-2 typically cause blisters, ulcers or vesicular lesions on an erythematous base; these eventually erode and crust (Figure 7a). Vesicles can occur at a single site or affect multiple anatomical sites after autoinoculation or in disseminated disease, where oedema, fissures or pustules can develop. The duration of genital lesions ranges from less than one week for recurrences to up to three weeks for primary infection. HSV infection is associated with eczema herpeticum (also called Kaposi varicelliform eruption) in people with atopic dermatitis, herpes gladiatorum in athletes and erythema multiforme (Figures 7b and c).14 Complications of genital HSV infection include enhanced HIV transmission, psychosexual morbidity, neuropathic bladder in the initial episode and neonatal herpes.
{kind=link}
Herpes simplex recurrences vary in symptom severity and frequency, but most are asymptomatic or have minimal features. Local trauma and systemic stimuli such as immunosuppression or fever can trigger reactivation of latent HSV.15
Diagnosis of HSV infection usually relies on the history and physical examination findings; however, a PCR test of a swab of the base of the ulcer or deroofed vesicle can be useful to diagnose asymptomatic or subclinical cases.
Treatment should be commenced as soon as possible for an initial episode and for moderate-to-severe recurrences of HSV infection. Primary oral mucocutaneous herpes can be treated with a topical anaesthetic such as benzydamine 1% gel or lidocaine 2% viscous solution for minor cases. Patients with severe oral mucocutaneous herpes can be treated with oral valaciclovir 1 g twice daily for seven days. Minor recurrences of oral mucocutaneous herpes can be managed with episodic antiviral therapy comprising aciclovir 5% cream five times daily for five days. For severe recurrences, oral valaciclovir 2 g twice daily for one day can be used.
The recommended treatment of genital herpes primary infection is oral valaciclovir 500 mg twice daily for five to 10 days. Recurrent genital herpes can be treated with episodic therapy with valaciclovir 500 mg twice daily for three days, or suppressive therapy with valaciclovir 500 mg daily for six months. The choice between episodic or suppressive therapy depends on the frequency and severity of recurrences and psychosexual complications. Patients with frequent recurrences or immunosuppression may require higher doses of antiviral treatment. Antipyretics, saline baths and topical lignocaine can help relieve symptoms. Pregnant women, immunocompromised patients and patients with allergies to antiviral agents require specialist advice.15
Exposure to HSV and varicella-zoster virus (see below) can cause viral keratitis, which is a medical emergency. Patients require urgent referral for sight-saving management.
Follow up of patients with genital herpes is recommended to complete sexual health screening, counsel about prevention and provide further sexual health education. This should cover the importance of abstaining from sexual activities when lesions or the prodrome are present and use of condoms. Herpes is not a notifiable condition.
Vesicles on the face, trunk and limbs - varicella (chickenpox)
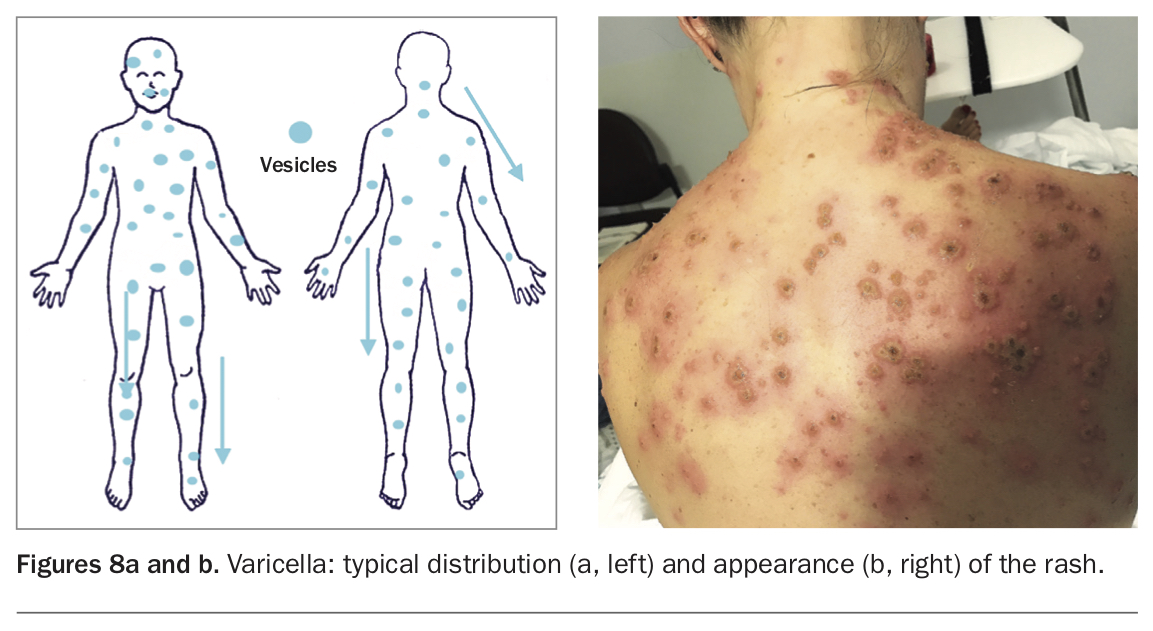
Primary infection with the varicella-zoster virus (VZV) causes varicella (chickenpox), during which the virus becomes latent in ganglionic neurons. VZV is highly infectious and spreads by the airborne route, with skin vesicles the main infectious source. The incidence of varicella is highest among children aged 1 to 9 years, and during winter and spring. VZV vaccines have greatly reduced the incidence, morbidity and mortality of VZV infection; however, the rise of antivaccine movements and the increase in immunocompromise in the population means that ongoing efforts to prevent and treat VZV infection are essential.16
Cough, coryza, fatigue and fever can be experienced in the prodrome of VZV infection, which is followed by a generalised cropping, vesicular, pruritic rash. The rash spreads cranially to caudally, and can involve the scalp and oral mucosa (Figures 8a and b).7 The vesicles can become haemorrhagic. Serious complications of VZV infection include bacterial sepsis, pneumonia and neurological and haematological complications.
{kind=link}
Clinical diagnosis is the mainstay for VZV infection; however, PCR testing of swabs from skin vesicles, saliva and cerebrospinal fluid can confirm the diagnosis. Differential diagnoses include other herpesvirus or enterovirus infections or drug intolerance.
Varicella is usually self-limiting in otherwise healthy children. Treatment of uncomplicated cases of varicella in children is symptomatic, including taking lukewarm baths with baking soda or oatmeal, calamine lotion to reduce itch and paracetamol. Immunocompetent children with pre-existing skin disease should be treated with oral valaciclovir 20 mg/kg up to 1 g, eight-hourly for seven days.
Adults have a higher risk of adverse outcomes and should be treated with oral valaciclovir 1 g, eight-hourly for seven days. Antiviral therapy should also be started in people with severe varicella (intravenous aciclovir 10 mg/kg, eight-hourly), people who are immunocompromised, pregnant women and newborns with congenital varicella syndrome. Preventive measures include VZV vaccination and administration of VZV immunoglobulins in high-risk patients.7
Vesicles in a dermatomal distribution - herpes zoster
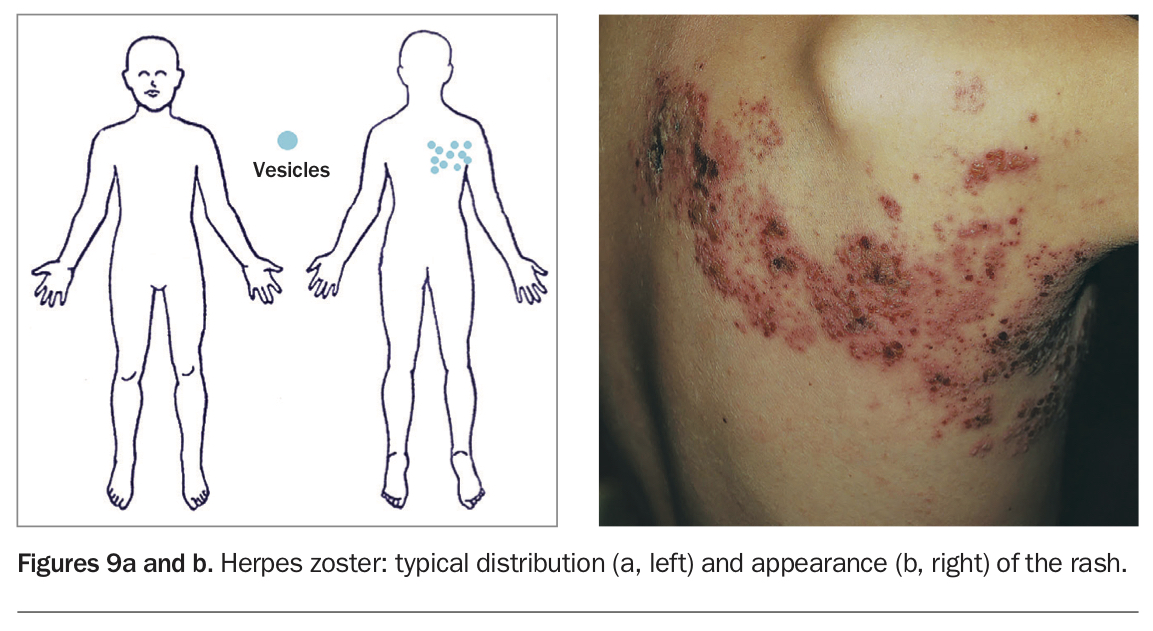
Herpes zoster, also known as shingles, is caused by reactivation of VZV. Because of waning immunity, the incidence and severity of zoster rises with increasing age. By the age of 85 years, over half the population will experience at least one episode of zoster.
Zoster is characterised by a two to three-day history of burning pain, followed by a localised eruption of vesicular lesions in the dermatomal distribution of the infected sensory nerve.17 The T1 to L2 dermatomes are those most affected (Figures 9a and b). Atypical presentations can occur, including a disseminated rash, minimal rash or no rash.17 The rash heals over two to four weeks but can result in scarring and permanent pigmentation. The pain can be severe, and persistent postherpetic pain is common. Zoster paresis, neuralgia, meningoencephalitis and vasculopathy can be complications of zoster and may occur without a rash.16
{kind=link}
Zoster can almost always be diagnosed clinically. Confirmatory tests include PCR, immunohistochemistry and viral culture of the vesicular fluid. Important differential diagnoses include contact dermatitis, herpes simplex and (for pain) cholecystitis, acute appendicitis and renal calculi.
A seven to 10-day course of oral antiviral therapy is recommended for patients with zoster, especially those who are immunocompromised, aged over 50 years and have lesions involving the face and eye. Treatment is most effective when started within 72 hours of rash onset. Patients should be advised to keep the rash clean and dry and avoid irritating products to prevent delayed healing and superimposed bacterial infection.18 Additionally, patients should cover the rash and maintain hand hygiene to prevent VZV transmission, and avoid contact with pregnant women, children who have not had varicella or VZV vaccine and people who are immunocompromised. Patients who have eye involvement or who are immunocompromised should be referred to a specialist.
White lesions on the mucosa (Koplik spots) - measles
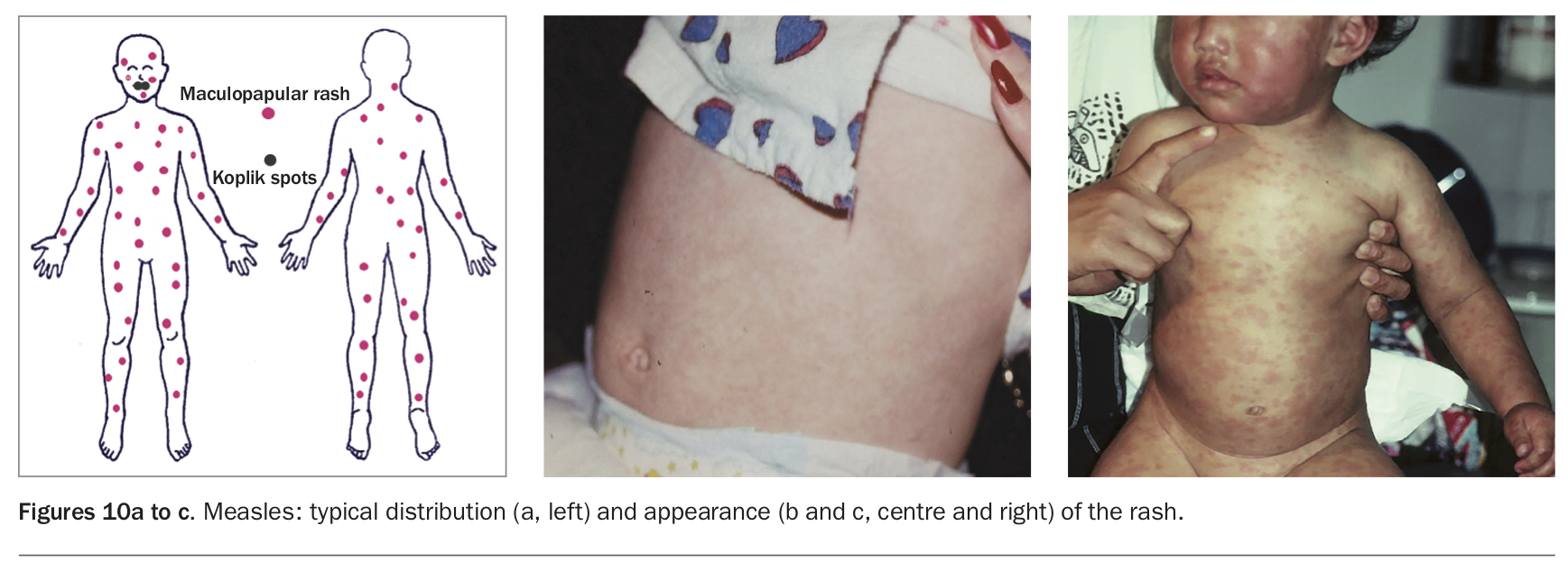
Measles is a highly contagious disease caused by measles virus and was the first immunosuppressive infection to be discovered. Measles was the leading cause of child morbidity and mortality before the development of measles vaccines in the 1960s. Measles typically begins with a fever and at least one of the three Cs: cough, coryza and conjunctivitis.12 Small white papules, known as Koplik spots, can appear on the buccal mucosa one to two days before the rash. A confluent maculopapular nonitchy rash first appears on the face and behind the ears and then spreads to the trunk and extremities (Figures 10a to c). The rash may be diminished in vaccinated children. The infectious period begins a few days before onset of the rash and lasts for several days. In uncomplicated cases, recovery can take one week. Possible complications include pneumonia, laryngotracheobronchitis, otitis media and keratoconjunctivitis.
{kind=link}
Measles can be recognised clinically; however, diagnosis can be challenging in the early stages of the disease and in immunocompromised and poorly nourished children. Testing for measles virus-specific serum IgM antibody can be confirmatory; however, antibodies are not detectable until at least four days after rash onset. Detection of viral RNA through PCR testing of throat, nasal, nasopharyngeal and urine samples is a more reliable diagnostic test. Other diseases that may be confused with measles include rubella and human parvovirus B19, enterovirus and HIV infection.
Management of patients with measles includes supportive therapy, correction of dehydration and nutritional deficiencies and monitoring for secondary bacterial infection.19 It is crucial to follow local communicable disease guidelines on notification and contact management.
Maculopapular rash with cephalocaudal progression - rubella
Rubella, also known as ‘three day’ or ‘German’ measles, is caused by rubella virus. This virus spreads through the respiratory route and is a candidate for global eradication because humans are the only known host. Rubella outbreaks occur in spring, and the mean age for rubella among unvaccinated children is 5 to 9 years.
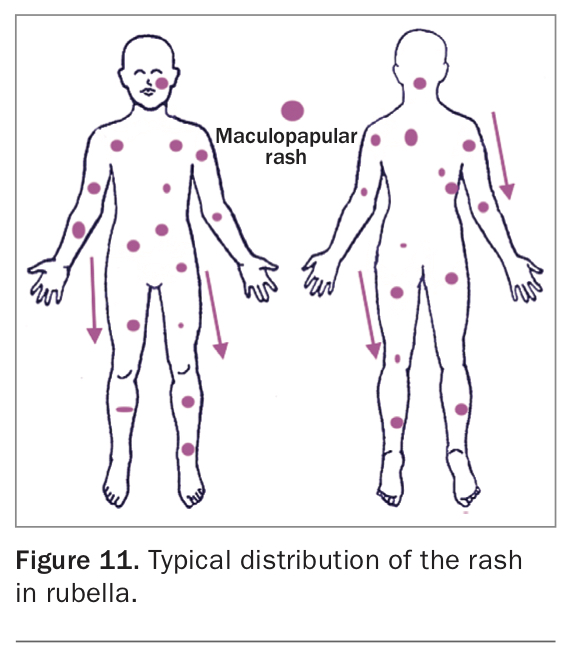
The clinical manifestations of rubella are mild and appear in only 50% of infected cases. A five-day prodrome of fever, headache and upper respiratory tract symptoms is associated with a cephalocaudal progression of a rose-pink coalescing maculopapular eruption (Figure 11). The rash disappears in one to three days. Symmetrical lymphadenopathy mainly affecting occipital and postauricular lymph nodes is also a prominent feature.1 Severe complications include haemolytic anaemia, thrombocytopenia, pericarditis, myocarditis and encephalitis.2 Rubella just before conception or during early pregnancy causes fetal defects in up to 90% of cases.20
{kind=link}
Acute rubella can be diagnosed by a positive PCR test for rubella virus or demonstration of rubella-specific IgM seven to 10 days after onset of the rash (in the absence of recent rubella vaccination), or a fourfold rise in rubella IgG antibody concentrations between paired acute and convalescent sera spaced at least a fortnight apart (in the absence of recent rubella vaccination). It should be noted that a high proportion of IgM-positive results will likely be false positives given the low incidence of rubella in Australia. Differential diagnoses include adenovirus and parainfluenza virus infection and drug-induced exanthems.21 Treatment of rubella is supportive, including bed rest and maintenance of oral fluid intake.
Women planning pregnancy should be tested serologically for rubella immunity, so they can be vaccinated before conception if necessary. The detection of rubella-specific IgM in pregnant women needs to be confirmed in a reference laboratory, and repeat testing for IgG seroconversion may be required. Women diagnosed with rubella during pregnancy should be referred promptly to an obstetrician for counselling about the risks of intrauterine rubella infection and follow up. Prenatal rubella can be diagnosed by detection of viral RNA in a chorionic villi biopsy specimen, amniotic fluid or fetal blood.1
Rash with centrifugal progression from axillae - unilateral laterothoracic exanthem
Unilateral laterothoracic exanthem (asymmetric periflexural exanthem of childhood) is presumed to be caused by a virus, although the aetiology has not been proven. It typically affects children of European background aged one to five years. There is a female preponderance, and the condition occurs more frequently in the winter and spring.22
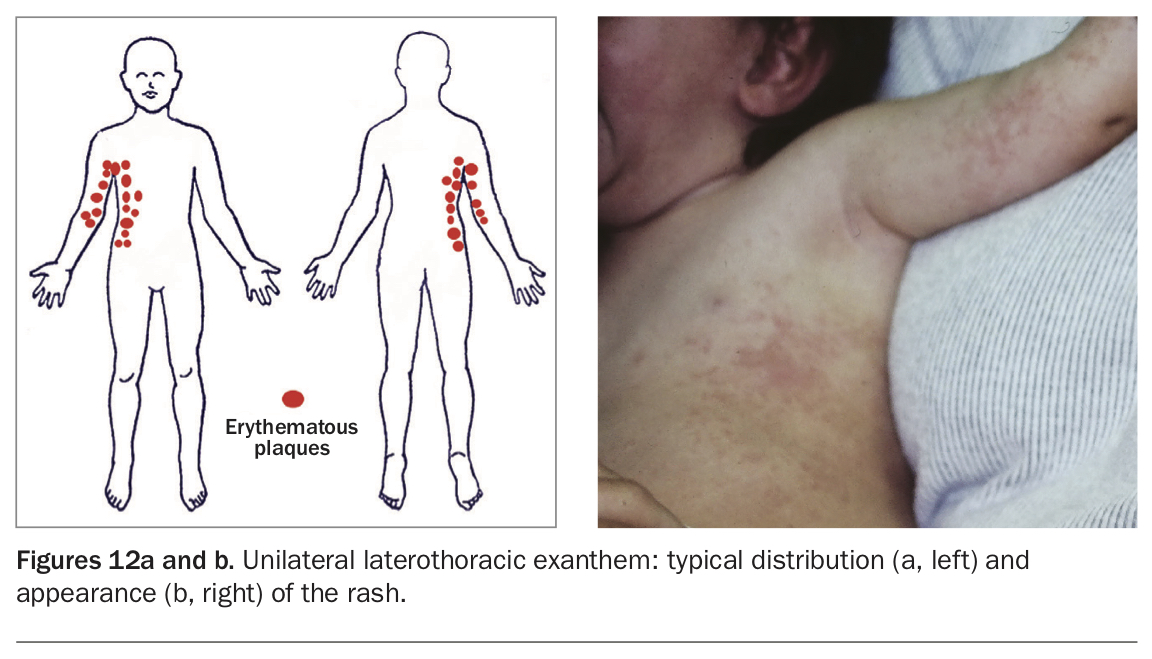
The eruption starts around the axilla or inside of the elbow and spreads along the affected side. The rash is usually limited to one side of the body (Figures 12a and b). The lesions coalesce to form large erythematous oedematous plaques accompanied by itching. There can be a surrounding pale halo in the early stages of the eruption, which later becomes scaly. A prodrome or concomitant gastrointestinal or upper respiratory symptoms may develop. Unilateral laterothoracic exanthem is a self-limiting disease with no sequelae and resolves over three to six weeks.
{kind=link}
The diagnosis of unilateral laterothoracic exanthem is fundamentally clinical, and a skin biopsy is not usually required. Differential diagnoses include Gianotti-Crosti syndrome, miliaria, scabies, fungal infection and atypical pityriasis rosea. Supportive treatments include oral antihistamines and topical bland emollients and soothing lotions.23 Topical corticosteroids are not effective.12
Fir-tree rash on the trunk - pityriasis rosea
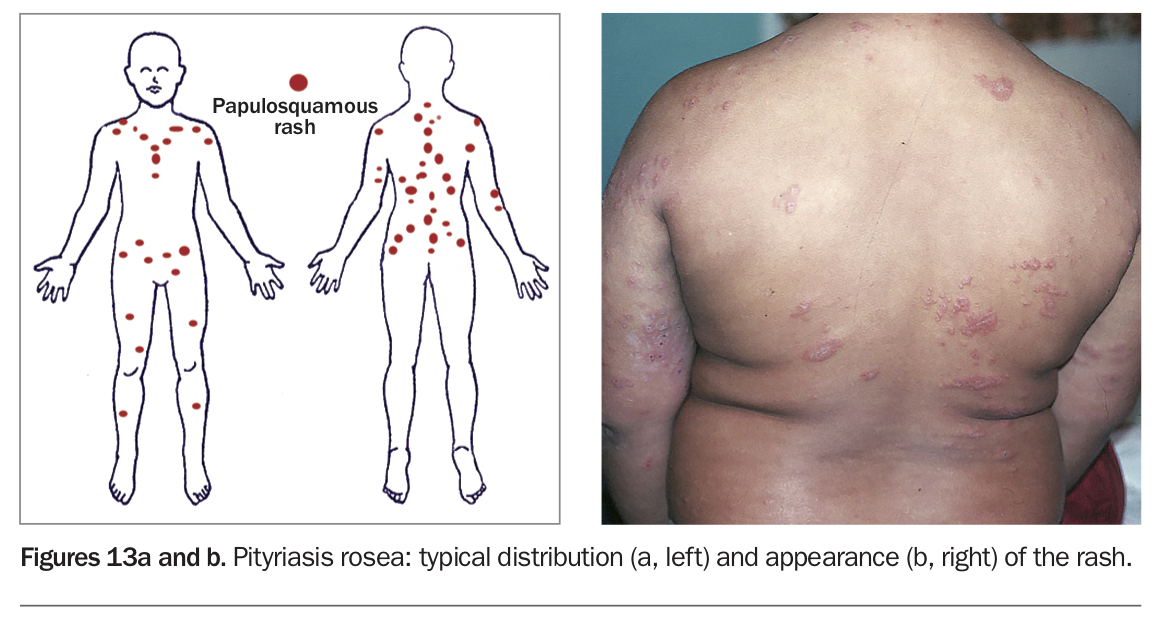
Pityriasis rosea is an acute self-limiting exanthem with an unknown aetiology, although possibly caused by HHV-6 and HHV-7. It commonly affects adolescents and young adults. Pityriasis rosea typically starts with a single erythematous, scaly plaque, known as the herald patch. This is followed by a secondary eruption consisting of smaller papulosquamous lesions along the cleavage lines of the trunk in a ‘Christmas tree’ or ‘fir-tree’ pattern, which last for days to weeks (Figures 13a and b).2 Atypical presentations include unilateral, inverse, lichenoid, vesicular, papular, purpuric, erythema multiforme-like and urticarial rashes.24 Postinflammatory hyper- or hypopigmentation may result. Up to 60% of patients experience prodromal symptoms or pruritus.
{kind=link}
The diagnosis of pityriasis rosea is clinically challenging, and skin biopsy shows nonspecific changes. A pityriasis rosea-like eruption has been linked to certain medications, including lamotrigine, metronidazole, terbinafine, isotretinoin, ACE inhibitors and clonidine. Differential diagnoses such as guttate psoriasis and secondary syphilis should be considered.9
Treatment is symptomatic, and patients should be reassured that the condition is not contagious. If symptoms are severe, topical menthol or a corticosteroid can be trialled. If the rash persists for more than three months, or if symptoms are severe or diagnosis is uncertain, referral to a dermatologist is recommended.
Other viral exanthems
Ross River virus disease
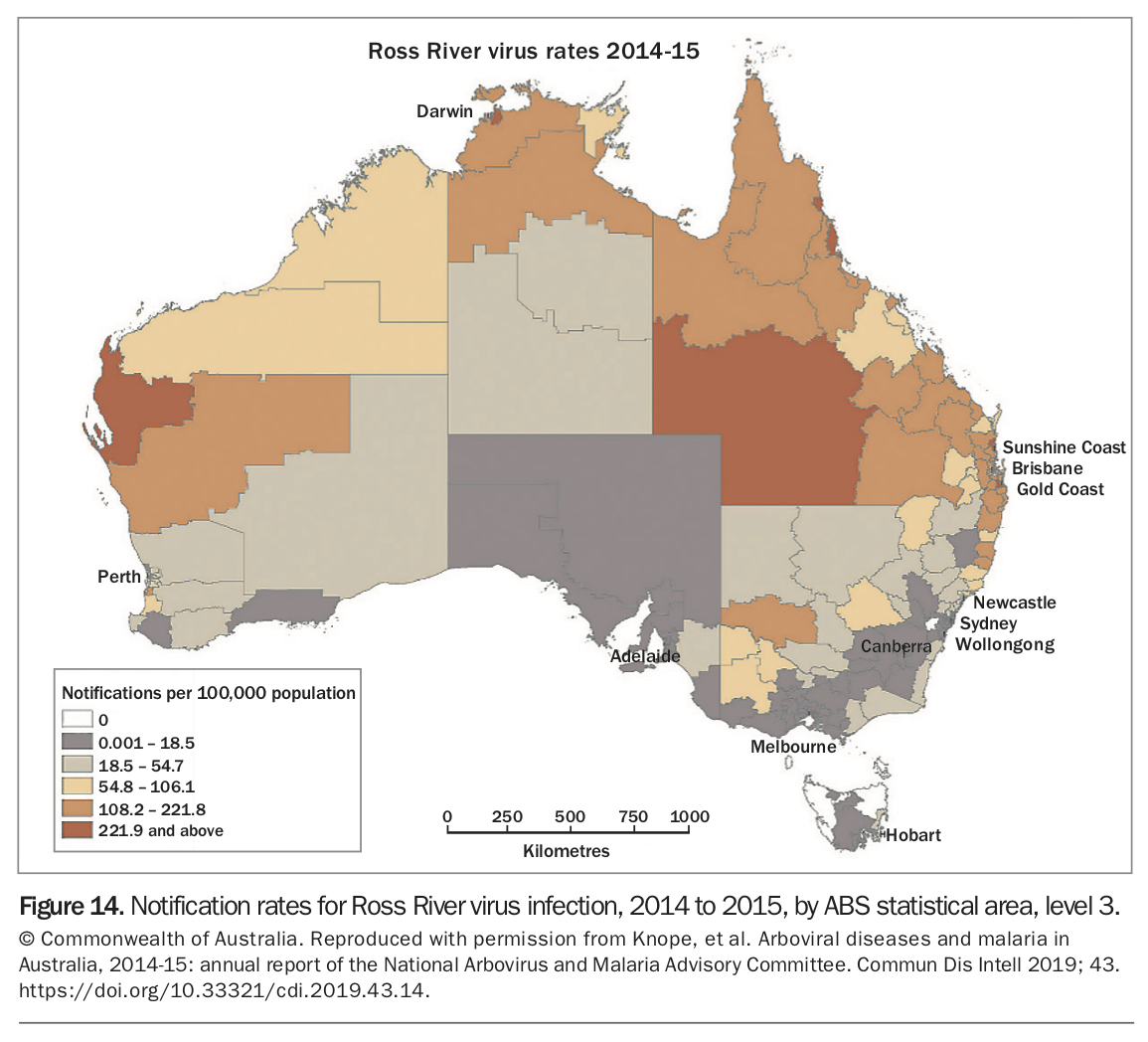
Ross River virus (RRV) is a mosquito-transmitted alphavirus that causes epidemic polyarthritis and arthralgia, known as RRV disease. RRV is endemic in Australia, particularly northern Australia (Figure 14) and Papua New Guinea and has caused epidemics in the Pacific Islands.25 Risk factors for outbreaks are increased rainfall and high maximum tides.
{kind=link}
RRV disease commonly affects adults aged 25 to 44 years, with men and women equally affected. The incubation period is generally seven to nine days, and infection is subclinical in 30% of cases.26 Symmetrical joint pain and lethargy are common complaints, with other symptoms including myalgia and headaches. A rash appears in 40% of patients, which is generally maculopapular affecting the limbs and trunk.14 There are also case reports of associated splenomegaly, haematuria, glomerulonephritis, meningitis and encephalitis. Arthralgia can take five to seven months to resolve.
Differential diagnoses include infectious mononucleosis, Barmah Forest virus disease, rubella, Q fever and other rheumatic conditions. Diagnosis is confirmed by seroconversion, with a change in paired serology results (IgM and IgG) consistent with transient IgM followed by long-term IgG (see the case study in Box 3).27
{kind=link}
Management of RRV disease is supportive, including rest, NSAIDs and physical interventions such as massage and physiotherapy.1 In the acute phase, patients’ functional ability may be significantly impaired, and many require support with activities of daily living. RRV cases require notification to the appropriate public health unit as per state or territory guidelines.25
Barmah Forest virus disease
Barmah Forest virus (BFV) is another alphavirus endemic in Australia. It causes BFV disease, characterised by epidemic polyarthritis and myalgia. It is the second most common mosquito-borne disease after RRV disease.28
The incubation period of BFV disease is five to 15 days. BFV causes a rash in 90% of cases; the rash is more florid than that in RRV disease. It appears with the onset of illness and spreads cephalocaudally. The rash may be maculopapular, purpuric or vesicular.14 Patients with BFV disease tend to have less joint swelling than those with RRV disease. BFV infection can also be asymptomatic.
Because of the overlap in symptoms with RRV disease, patients are generally tested for both BFV and RRV. BFV disease is confirmed in the same way as RRV disease and is also notifiable. Clinically appropriate symptomatic treatment such as NSAIDs or paracetamol should be administered while waiting for confirmation.27
Influenza
Influenza is a common respiratory disease caused mostly by influenza A and B viruses. It is transmitted from human to human. The health impact of influenza is generally mild in healthy individuals. However, certain groups are at higher risk of developing severe disease and complications, including people of advanced age, infants, those of Aboriginal and Torres Strait Islander origin or patients who are immunocompromised, have a chronic condition, are obese or pregnant and those who smoke.
An exanthem is uncommon in influenza, found in only 2% of cases, but is more likely in children. A confluent maculopapular rash sparing the face and palmoplantar surfaces was detected in patients infected with the novel influenza A (H1N1) 2009 pandemic strain (influenza A [H1N1]pdm09). Petechial exanthems can also occur, and influenza A can trigger Gianotti-Crosti syndrome.12
Influenza should be considered in children who present with a fever and rash, especially if they have respiratory symptoms during the ‘flu season’.14 Administration of the latest influenza vaccine around March or April every year confers the best protection against influenza.29
Coronavirus disease 2019 (COVID-19)
Since December 2019, coronavirus disease 2019 (COVID-19) has caused significant morbidity, mortality and financial impact worldwide. It is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), and transmission is via respiratory droplets and potentially aerosols. SARS-CoV-2 enters cells by binding to angiotensin-converting enzyme-2 (ACE-2) receptors, which are found in many parts of the body, including mucosal sites, the endothelium of dermal blood vessels and epithelial cells in eccrine glands. This distribution possibly explains the cutaneous manifestations observed in patients with COVID-19.30 Skin involvement has been reported in 0.2 to 24% of cases, although the true prevalence is difficult to ascertain.31
There is great heterogeneity in COVID-19 cutaneous presentations, possibly because of different immune responses to the virus. Cutaneous presentations include morbilliform, vesicular, pityriasis rosea-like and erythema multiforme-like eruptions, chilblains and Kawasaki-like disease in children.32 Vasculopathy-related lesions such as livedo reticularis, retiform purpura, ulcerations and necrosis have been seen in hospitalised patients with COVID-19. These lesions are hypothesised to be caused by the increased clotting tendency from complement activation.31 Herpes zoster is also increased in patients with COVID-19.33 Vesicular eruptions can be an early cutaneous sign, whereas chilblains can be a late sign.
It is important to include skin eruptions as clinical features of COVID-19 and to perform a full skin examination when evaluating patients with suspected COVID-19.30
Conclusion
Viral exanthems are polymorphous in their clinical presentations. Diagnosis can be challenging, especially in patients with unusual presentations or in those who are vaccinated, with potential for the vaccine to contribute to cross-reactivity or complement activation protection, or immunocompromised. Clinical diagnosis of viral exanthems depends on the distribution and morphology of the rash, geographic location of the case and exposures. Most exanthems are self-limiting and are treated with supportive care. MT
Acknowledgement
The authors wish to thank Professor Gayle Fischer, Royal North Shore Hospital, Sydney, for providing the clinical photographs in Figures 3 to 13.