Real-time prescription monitoring: how it can help safe prescribing of high-risk medicines

Dr Wilson is a Staff Specialist in Addiction Medicine at Drug and Alcohol Services, South East Sydney Local Health District; Conjoint Lecturer at the School of Public Health and Community Medicine, UNSW Sydney; and a GP in Sydney, NSW.
Mr Hargreaves is Program Manager, Real Time Prescription Monitoring Program, eHealth NSW, Sydney, NSW.
Drug safety
Prescription drug abuse

Real-time prescription monitoring (RTPM) of high-risk medications such as opioids and benzodiazepines is available or in development around Australia. Six case scenarios explore how RTPM can help GPs prescribe safely, including responding to a new patient or inherited patient requesting opioids and reassessing their own patient taking high-risk medications.
Real-time prescription monitoring (RTPM) is being implemented around Australia, under the oversight of state and territory governments. These programs seek to decrease the risks and harms of high-risk prescription medicines such as opioids and benzodiazepines. RTPM can help prescribers and pharmacists make informed decisions about prescribing and dispensing. It can also inform clinical decisions about the level of support patients require to help manage their medical conditions.
This article focuses on prescriber experience and presents common case scenarios of patients prescribed high-risk medicines. These scenarios are designed to help prescribers think through their approach to management with the assistance of RTPM.
Case 1. A new patient requesting opioids
Josephine, aged 49 years, is new to your practice and arrives late on a Friday afternoon as a ‘walk in’. She says, ‘I know you’re busy, doctor, and I won’t take much of your time. I just need a repeat script for my oxycodone’.
She explains she had to travel without notice to assist her father, who is unwell, and her prescription has run out. Her GP in her home town is not available to help. She has a letter from a medical specialist in another city, listing her medications as:
- oxycodone 5 mg as required, one to two daily
- oxycodone modified release (MR) 20 mg twice daily
- fentanyl 12 mcg/h transdermal patch
- diazepam 5 mg three times daily
- pregabalin 150 mg twice daily.
Your heart sinks as you hear her story and read the list. It is too late in the day to ring the specialist, and you have no idea how safe her medication use is.
Many GPs have experienced the ‘heart sink’ that occurs with a case such as this. Although the prescribed medicines may be appropriate, when the patient is unknown, corroborative information is often limited to help make an informed prescribing decision.
Around the world, drug-induced deaths from prescribed and nonmedical use of high-risk medicines have increased.1 In Australia, opioids caused three out of five drug-induced deaths in 2020, and benzodiazepines were also often implicated in these deaths.2,3 Most of these deaths were accidental.2 Overdose risk is increased by concurrent use of other sedatives, including benzodiazepines, stimulants, sedating antidepressants, antipsychotics, gabapentinoids and nonpharmaceutical sedatives such as alcohol.2,4 Some of these deaths resulted from unco-ordinated supply of medicines, including prescriptions for multiple high-risk medicines obtained from multiple prescribers.2,5,6
Prescribers often find themselves in a difficult position with not enough information to assist their prescribing decisions. The national Prescription Shopping Information Service (PSIS), although helpful, provides information on only a small number of patients who are obtaining a large amount of PBS medicines from multiple prescribers.7 Further, this information is often incomplete and out of date.
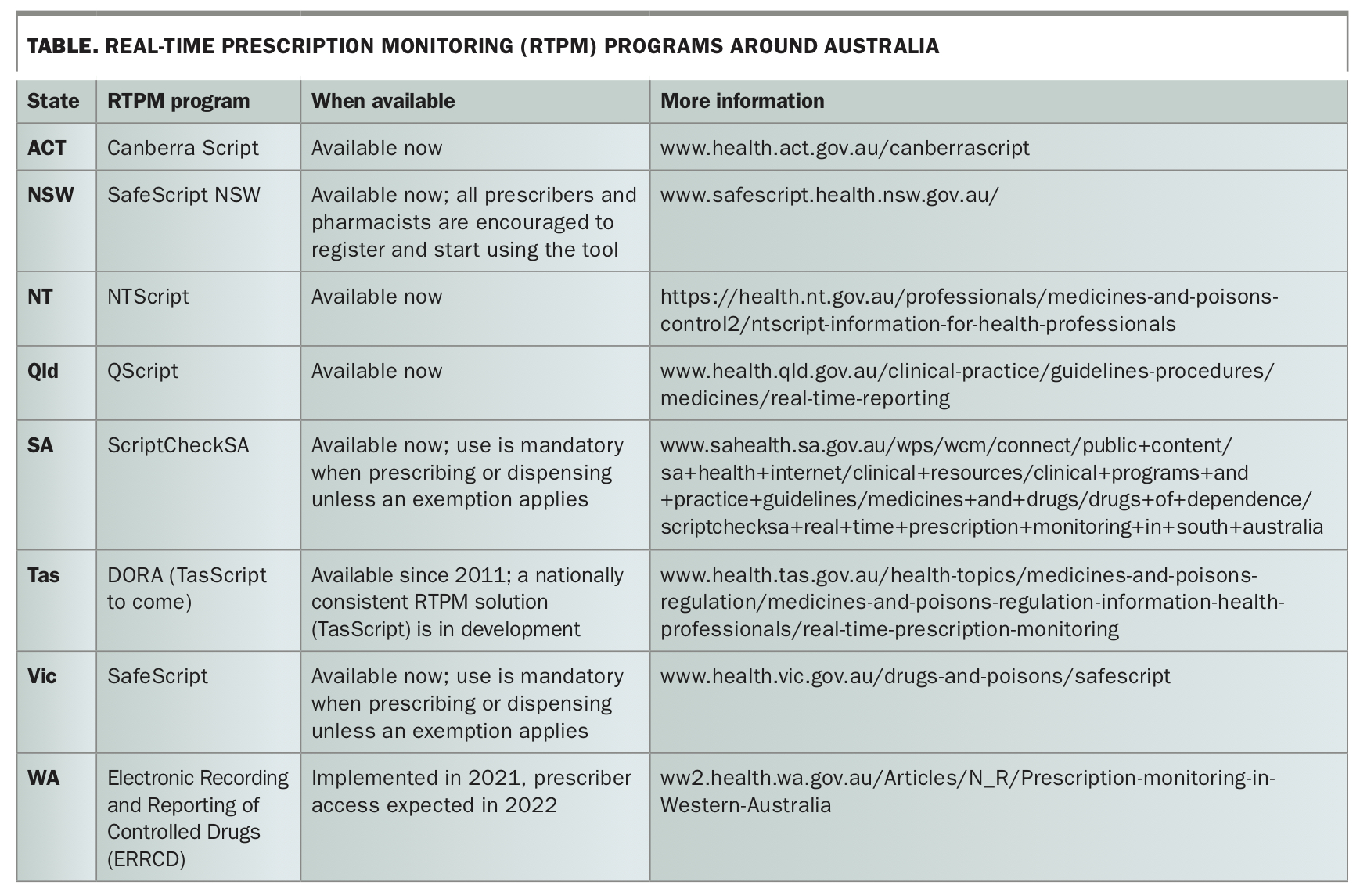
The Australian government has developed several initiatives to minimise the harms caused by prescription medicines. These include the upscheduling of alprazolam and most codeine-containing products, and changes to labelling, PBS listing and indications for opioids. This has also led to a commitment to provide RTPM. In some states, RTPM has been available for years, whereas in others it is still in development (Table).
{kind=link}
RTPM programs differ slightly around the country. However, the common goal is to provide Ahpra-registered prescribers and pharmacists with up-to-date information on high-risk prescribed medicines, both PBS and non-PBS (private), that the patient has accessed at the time of writing or dispensing the prescription.
What makes a medicine high risk?
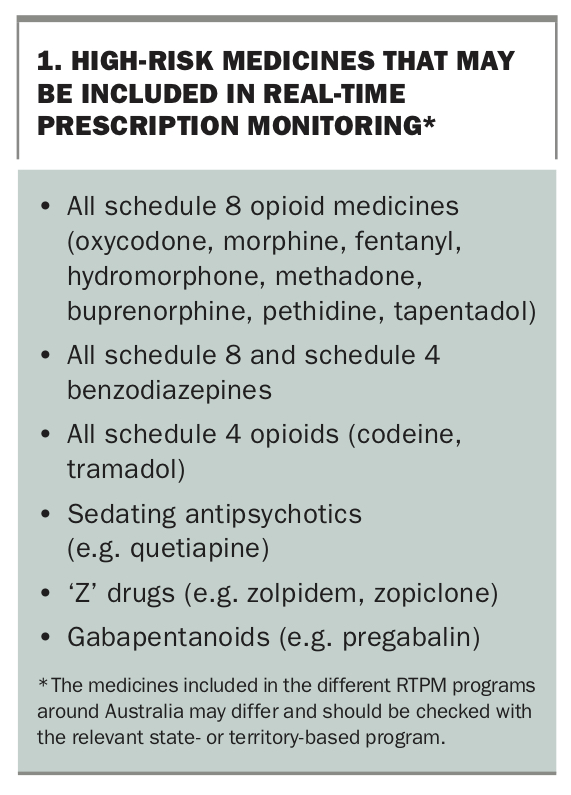
High-risk medicines are psychoactive; they act on the central nervous system, altering mood, perception, consciousness and behaviour. They include opioid analgesics, stimulants, antipsychotics, mood stabilisers, anxiolytics, hypnotics and antidepressants. Some of these are higher risk and are included as part of RTPM (Box 1). Their use can be complicated by dependence and addiction, leading to compulsive, risky medication use at higher doses and for longer than planned, with unsuccessful attempts to cut down and accompanying withdrawal symptoms. Simultaneous use of multiple medications increases risk, as does concurrent use of nonprescribed sedatives such as alcohol and heroin. Sedation can lead to respiratory depression, respiratory arrest and cardiac arrest, resulting in fatal overdose. Nonfatal overdose can lead to organic brain injury, cognitive impairment and ongoing disability.
{kind=link}
Increasing the dose of high-risk medicines increases risk.8 The route of administration also influences risk; taking an oral or transdermal medicine intravenously leads to rapid onset of action and greater availability of the active constituents.9 Comorbidities can also increase the risk of overdose and other harms in individual patients. The risk is compounded by lack of patient knowledge about their medication risk and poor access to treatment.10
Further, our understanding of the risks versus benefits of high-risk medications has changed over time. Opioids are of limited use for chronic pain. Their efficacy is likely to be small with a risk of serious sequelae. There is little evidence supporting long-term use of benzodiazepines, and cessation of these medications can be difficult.11
Assessing opioid risk
The risk of opioids increases with increasing dose and potency.8 Some opioids (e.g. hydromorphone and fentanyl) are more potent than others. Calculating the oral morphine equivalent dose (OMED) for opioids can help assess risk. We suggest that prescribers should start considering the efficacy and risk of prescribed opioids in patients using an OMED greater than 60 mg/day, as this suggests the pain condition is not opioid-responsive. In fact, a dose greater than 100 mg/day OMED is estimated to lead to a fivefold increase in risk of harm.8
Some RTPM programs calculate the OMED and send notifications when the dose exceeds certain thresholds. The Faculty of Pain Medicine in the Australian and New Zealand College of Anaesthetists provides a free app to help with OMED calculation (www.opioidcalculator.com.au).12
Benefits of RTPM
As illustrated in Case 1, prescribers may have limited information to inform the clinical decision: should they prescribe or not? It may be that the patient Josephine is taking her medicines absolutely as directed and is low risk, or she may have developed issues due to her prescribed medicines but be unaware of her risk, or she may be one of a small group of people knowingly seeking medicines for their intoxicating effect or to sell on to others.13
Assuming everyone is drug seeking, although understandable, is unhelpful for many patients who feel targeted and stigmatised when they have been taking their medicines as directed.14 Sudden cessation of opioids has been found to increase hospital emergency department visits and admissions, with adverse effects on the management of patients’ chronic health conditions.15
RTPM allows prescribers to make informed decisions about the risk of prescribing by providing up-to-date in-time information about medicines. RTPM programs have been shown to decrease overdose deaths and help patients at risk of harm to be diagnosed and offered appropriate treatment.6,16
When should you use RTPM?
RTPM is useful for new patients and patients inherited from other prescribers. In these groups, there is limited knowledge of the patient’s history and little therapeutic alliance. RTPM can help the potential new prescriber to reassess and reframe current management and corroborate information to inform best options for treatment.
RTPM is also useful when reviewing a colleague’s patient to fulfil PBS requirements for ongoing opioid prescribing after 12 months. In this situation, the reviewing doctor has access to the patient’s history through consultation with the patient, their medical records and RTPM. This can bring a fresh perspective to the patient’s management and assist with choosing the most appropriate treatment options.
In longstanding patients who are well known to the prescriber, the introduction of RTPM may feel intrusive to both prescriber and patient. However, given the changing approach to management, RTPM can assist objective re-evaluation to ensure the patient is receiving the most appropriate management.
Importance of language used
Some patients will feel targeted or stigmatised when their long-term use of high-risk medicines is reviewed, and the language the prescriber uses to describe their presentation is important.14,17 Patients can also become afraid and anxious when they think their medicines will be ceased and worry about an exacerbation of their illness. It can take time to help them understand the need to reassess and perhaps make treatment changes.
It is important to use person-centred language and to work collaboratively with the patient. Language matters, and the words used can help the patient better understand the case for change. Let your patient know that you need to check RTPM to ensure you are not going to cause them harm. Understand that this issue can be distressing for both the patient and prescriber. Focus on the medicine risk rather than perceived attributes of the patient. For example, say: ‘these medicines are high risk and can cause real harm to people. I want to ensure you receive the best and safest treatment possible to help you manage your health’. Don’t say ‘you’re an addict and you need to stop now’.
Weigh up the consequences of not prescribing versus the risk of continuing to prescribe. Understand that often not everything can be solved in one appointment. You may need a number of appointments to fully assess your patient’s presentation and history.
At times, the risk of prescribing outweighs everything else. Case 2 illustrates a patient whose use of medicines is high risk. Another prescription is likely to add to this risk without achieving positive therapeutic outcomes. RTPM helps with this assessment.
Case 2. Refusing a request for opioids
Adam, aged 49 years, is new to your practice and, like Josephine, arrives late on a Friday afternoon as a ‘walk in’ and asks for a repeat script for oxycodone.
You have access to RTPM, which shows that he is prescribed:
- oxycodone 5 mg as required
- oxycodone MR 20 mg twice daily
- fentanyl 12 mcg/h transdermal patch
- diazepam 5 mg three times daily
- pregabalin 150 mg twice daily.
Adam has obtained these prescriptions from six different practices and had them dispensed at six different pharmacies. His most recent prescriptions for oxycodone and oxycodone MR were last dispensed three days ago. His prescribed OMED is 126 mg/day, but given his frequent attendance and many prescriptions, his actual OMED is likely to be much higher. His use of other sedatives, diazepam and pregabalin, increases his risk of harm. Alternatively, he could be selling these high-risk medicines, with risk of harm to others.
You explain that you are concerned about the large number of medications he is taking that can cause him harm and, given this information, you cannot prescribe. You encourage him to seek help for his medication use and let him know you are happy to refer him for further support.
The issues in this case are clear cut; it is not appropriate to prescribe oxycodone for Adam, and this request should be refused. This refusal may result in conflict in the consultation, and it is not uncommon for prescribers to be verbally threatened by patients seeking high-risk medications.18 In this situation, a prescriber needs to assess their personal safety and refuse to prescribe if they are safe to do so. If personal safety is threatened, you may choose to give the prescription, seek support from your colleagues and institute a practice-wide response to this behaviour.19,20 This may include calling the police and a practice-wide ban that prevents the person attending your practice in future. Document the incident and the plan in your clinical notes and inform your medical defence organisation and regulatory authorities of the incident.
More often the situation is not so clear cut. There are good reasons why the patient is on the medication, they may not understand why there are concerns, and with time you can help them safely manage their health.
How to respond
Explain and set boundaries
Talk to the patient about the risks of harm from their medication. Explain the need to re-evaluate their treatment to achieve the best outcomes for them. Assure them of your long-term collaborative commitment to their care. Set clear prescribing boundaries. They need to attend for regular appointments, see only one doctor, get their medicines from one pharmacy and attend for any other reviews that are needed to ensure best management, as in the following Case 3.
Case 3. Helping a temporary patient
Sean, aged 49 years, is new to your practice and also arrives late on a Friday afternoon as a ‘walk in’ and asks for a repeat script for oxycodone.
Like Josephine, he explains he had to travel without notice to assist his father, who is unwell, and his prescription has run out. His GP in his home town is not available to help. He also has a letter from a medical specialist in another city, listing his medications as:
- oxycodone 5 mg as required, one to two daily
- oxycodone MR 20 mg twice daily
- fentanyl 12 mcg/h transdermal patch
- diazepam 5 mg three times daily
- pregabalin 150 mg twice daily.
You review Sean’s medications on RTPM and see he has seen only one doctor for prescriptions and had them dispensed at a single pharmacy over the past three months. He is taking all his medications as prescribed, and his last prescription for oxycodone was 27 days ago.
You tell Sean you are concerned as he is taking multiple opioids and other high-risk medications that increase his risk of harm. You explain that because of this and the limited information you have, you are happy to prescribe the oxycodone but will organise staged supply through a local pharmacy to ensure he has medication over the weekend. You arrange a follow-up appointment for Sean on Monday and explain that you will talk to his current GP to obtain additional information to ensure best care.
Seek advice
For any patient taking high-risk medications, GPs can seek further information to support their prescribing decisions.
- Call the available telephone specialist addiction support services in your state or territory for advice.
- Check local HealthPathways for treatment and referral options.
- Ask for a second opinion from a colleague. Refer to pain, addiction or mental health services as required and available in your area.
- Consider accessing specialist telehealth services for this if they are available.
Manage, reduce risk and improve outcomes
Staged supply or supervised pharmacy dosing can help patients manage their medications more safely and provide greater oversight and support. Consider prescribing naloxone (intranasal or intramuscular) for opioid overdose, and teach the patient, their family and others involved in their care how to recognise an overdose, how to manage this and how to use naloxone.21,22
Set clear and achievable goals and assess these regularly with functional measures such as the Brief Pain Inventory.23,24 Institute self-management and nonmedication options and help the patient to understand the important roles of these in the ongoing management of their health. With the patient’s consent, involve family and others involved in their care.
A practice-wide approach and the use of case conferencing, GP chronic disease management plans and team care arrangements can help ensure members of the treatment team work together and understand the roles and responsibilities of everyone involved.
Assess for addiction or substance use disorders
Some patients may have developed a substance use disorder, including benzodiazepine use disorder or opioid use disorder. It is important to assess and treat this. Buprenorphine and methadone are highly evidence-based treatments as part of medication-assisted treatment of opioid dependence (MATOD).25,26 The regulations for prescribing these medications vary. Prescribers should seek help from state and territory guidelines, local drug and alcohol services and 24/7 state and territory drug and alcohol telephone lines.
Consider the use of urine drug screening if there are concerns about the use of nonprescribed substances.27 Check the costs and what substances are tested for with your local pathology service.
If it becomes clear that patients are injecting their medicines, encourage them to seek help for this with a referral to drug and alcohol services and advice about safer injecting and attendance at a medically supervised injecting centre for further support (available in Sydney and Melbourne).
Look at other options
Some patients will benefit from tapering their medicines. This is a collaborative patient-centred approach to slowly and safely decrease doses. It requires long-term commitment on the part of the patient and the treating team.
The patient may benefit from a specialist opinion or collaborative management from allied health, pain or addiction services. They will also benefit from the ongoing involvement of their GP to help them shift to other treatment options.
Case 4. Managing an inherited patient taking opioids
Helen, aged 44 years, is a patient of a retired colleague in your practice. She tells you ‘Dr X has prescribed oxycodone for me for years’.
You see in her medical records that she is prescribed oxycodone MR 30 mg twice daily, which was commenced in a hospital emergency department after she sustained extensive superficial abdominal burns three years ago. She attends the practice regularly for oxycodone prescriptions. She takes no other prescribed medications, does not drink alcohol or smoke and has a past history of postnatal depression and no other health issues.
On reviewing Helen’s records, you suspect that her abdominal burns have fully healed and she may no longer have a chronic pain condition nor require ongoing opioid medication. RTPM shows that she has obtained prescriptions only from your colleague and no other high-risk medications are prescribed.
You gently ask Helen about her history, and she tells you that she has tried several times to reduce the oxycodone dose but gets terrible anxiety, nausea, diarrhoea and an overwhelming desire to take the medication. You acknowledge how hard this has been for her and let her know that she has developed a side effect of the long-term medication and is experiencing withdrawal from the medication. As a result, she needs to decrease the dose slowly to cease this. You let her know that if she cannot decrease and stop, there are other treatments, such as buprenorphine or methadone, which can help her manage her condition. You also let her know that you will support her throughout this process.
This case illustrates a not uncommon scenario where a patient was started on an appropriate medicine but it was not ceased in a timely manner. This has led to long-term use and the development of opioid dependence. Opioid cessation is likely to improve the patient’s wellbeing; however, reduction may need to be slow, and some patients may need methadone or buprenorphine as part of MATOD. Most importantly, a planned reduction with frequent review and support from the prescriber, pharmacist, a counsellor and family and friends will assist this.
Case 5. Reassessing prescribing for your own patient - safe use
David, aged 60 years, comes to see you for ‘my usual medications’. He has severe osteoarthritis in both knees and hips, recurrent lower back pain and chronic insomnia. You have been prescribing the following medications for him for eight years:
- oxycodone plus naloxone 15 mg/7.5 mg twice daily
- oxycodone 5 mg as required for breakthrough pain (20 tablets per month)
- diazepam 5 mg at night as required (two to three tablets per week)
- pregabalin 75 mg twice daily.
You explain to David that you need to check RTPM to ensure that his medication use is going safely. RTPM shows that he has no additional medications or prescribers; he is taking his medication as prescribed and obtains his medications from one pharmacy.
You assess his progress using the Brief Pain Inventory. His pain is controlled, with a pain score of 4/10 and a pain interference score of 3/10. His mood is stable, he walks his dog for about an hour on five days a week, is managing shopping, cooking and cleaning, and is active in his local men’s shed. He is happy with his current management.
In this scenario for the ongoing care of a patient with chronic pain, RTPM in conjunction with comprehensive assessment of function and treatment outcomes and regular reviews reassures the treating prescriber that the management is achieving the treatment goals and is low risk. Annual review by a second medical practitioner to fulfil PBS requirements for ongoing supply allows external oversight with ‘fresh eyes’.
Case 6. Reassessing prescribing for your own patient - high-risk use
Julie, aged 60 years, comes to see you for a repeat prescription. Like David, she has severe osteoarthritis in both knees and hips, for which you have been prescribing oxycodone plus naloxone combination 15 mg/7.5 mg twice daily. She has a past history of recurrent lower back pain and chronic insomnia, which you are not currently treating.
You explain to Julie that you need to check RTPM to ensure that her medication use is going safely. RTPM shows that she is also prescribed the following medications by another three doctors:
- oxycodone 5 mg as required for breakthrough pain (20 tablets per month), by another local GP
- diazepam 5 mg at night (50 tablets every two months), by a psychiatrist
- pregabalin 75 mg twice daily, by a GP in the local shopping centre.
You explain to Julie that you need to know if she is accessing medication from other doctors as the use of multiple medications increases the risk of serious side effects. To decrease this risk, you will need to contact her other prescribers to ensure all of her treating team are aware of all the medicines she is taking.
Julie is surprised as she did not realise this was an issue. She agrees that she would like you to continue to be her treating doctor. You organise consent for release of information for her other prescribers and let her know you will organise a case conference with them. You book her a long consultation in one week for review and to make long-term plans for her medication management.
In this case, the patient is accessing multiple high-risk medications from multiple prescribers. She is seeing a psychiatrist and accessing other prescribers as convenient, and all are prescribing with limited understanding of the patient’s entire care.
This fragmented care, although understandable, leads to a higher risk of harm as no healthcare provider has oversight of the whole treatment plan. In this situation, patient education, comprehensive assessment, regular treatment review and liaison with all treatment providers and the patient will help ensure best treatment outcomes. The patient needs to decide who will be their treating doctor, this doctor needs to agree to provide this care, and they need to plan regular treatment reviews together. This does not mean that only this prescriber can provide medications but that this provider needs to be given oversight and continue to interact with other providers to ensure safe and co-ordinated care. Currently available MBS numbers should be used to support this process.
Some patients have limited understanding of the risks of medication. They may have limited access to care because of geography, financial constraints, other health issues, poor health literacy, caring responsibilities or cultural considerations. Increasing their access to treatment and knowledge of their risks is core to ensuring appropriate and safe care.
Conclusion
Chronic pain, mental health issues and substance use disorders can lead to significant disability. The population of Australia is fortunate to have low-cost universal access to medications through the PBS. Some medicines are higher risk because of their pharmacological properties. RTPM helps prescribers and pharmacists make informed treatment decisions when prescribing high-risk medications. RTPM should assist but not rule clinical decisions. It should be used as a tool. Key practice points on RTPM are summarised in Box 2. We recommend that prescribers work collaboratively with patients and their families and carers and seek further support and advice through local state and territory or bodies whenever needed. Remember the patient may have a chronic condition and need long-term management. MT
{kind=link}
COMPETING INTERESTS: Dr Wilson has received payment for sitting on expert and clinician panels on monitored medicines as part of the rollout of SafeScript NSW and for creating and facilitating training for prescribers and pharmacists; and funding for consulting and sitting on expert advisory panels for Indivior, Lundbeck, Mundipharma, Pfizer and Seqirus. Mr Hargreaves: None.