
Associate Professor Fischer is Associate Professor of Dermatology at Sydney Medical School – Northern, The University of Sydney, Royal North Shore Hospital, Sydney, NSW.
Competing interests: None.
What’s the diagnosis?
An unwell patient with a blistering rash




Case presentation
A 35-year-old woman presents with a three-day history of malaise, headaches, dysuria and sore throat. The day before her presentation she developed a widespread rash, which has now started to blister.
The patient suffers from depression and was commenced on lamotrigine two weeks ago by her psychiatrist. She was otherwise well. She has not taken lamotrigine before but she has been treated with lithium and sertraline.
On examination, the patient appears unwell and she has a temperature of 39oC. She has an erythematous eruption involving her torso, limbs and face; superficial erosions and blisters are appearing in some locations. Her conjunctivae are injected and she has pharyngitis and vaginitis.
The patient is sent urgently to the hospital accident and emergency department. By the time she arrives, 30% of her skin has blistered (Figures 1a and b). Blood tests are performed: FBC results show an eosinophilia and liver function test results are abnormal.
Differential diagnoses
Conditions to consider among the differential diagnoses include the following.
- Viral illnesses. Patients with viral illnesses sometimes present with bizarre widespread eruptions. Blistering is unusual but may occur. It is possible for patients to be very unwell but this is uncommon. Viral illnesses may simulate many other conditions, but in an acutely unwell patient they are a diagnosis of exclusion.
- Bullous pemphigoid. This uncommon autoimmune blistering disease is usually seen in older patients. Bullous pemphigoid may be preceded by a prodrome of weeks to months in which there is a nonspecific eczematous itchy rash on the torso and limbs. The typical lesion is a thick-walled bulla on relatively normal skin (Figure 2). Mucosal lesions are unusual and patients are not unwell. Blood eosinophilia is often found.
- Bullous systemic lupus erythematosus (SLE). Rarely, SLE may present as an acute illness with fever, systemic symptoms and a blistering rash (Figure 3). Patients are usually known to have SLE. The rash is predominantly photodistributed, with blistering occurring on the face, upper trunk and arms. Mucosal involvement is uncommon.
- Drug reaction with eosinophilia and systemic symptoms (DRESS). This condition presents with a flu-like prodrome, which is followed by a widespread erythematous, exfoliative eruption that does not blister. Patients are very unwell with eosinophilia, fever and abnormal liver function. Multi-organ involvement often occurs. The drugs classically associated with DRESS are allopurinol, dapsone and antiepileptics.
- Stevens-Johnson syndrome (SJS). A mucocutaneous condition of varying severity, SJS (also known as erythema multiforme major) is not associated with systemic disease. Patients develop a blistering eruption, with the classic lesion being a ‘target’ that has the morphology of a bulls-eye. Although all mucosal surfaces, including the mouth, eyes and genitals, are often severely involved, patients remain systemically well. The usual triggers of this reaction are infections with herpes simplex virus (which can be subclinical) and Mycoplasma pneumoniae. Drugs are less common causes of SJS.
- Toxic epidermal necrolysis (TEN). This is the correct diagnosis. TEN and DRESS are the two most dangerous drug eruptions and each has a significant mortality, particularly in elderly and debilitated patients. There is some clinical confusion between TEN and SJS and in some cases the line between the two can seem unclear. Nevertheless, TEN has significant systemic associations and patients are severely unwell with a range of haematological, renal, liver and lung complications. It is possible for most of the skin surface to slough off in TEN, leaving the patient vulnerable to sepsis and loss of temperature control.
Causes
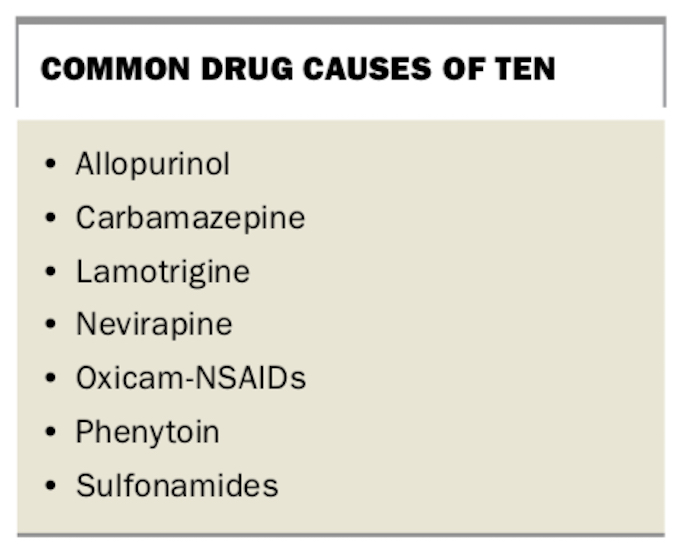
TEN is almost always induced by drugs (Box), with the most commonly involved drugs being sulfonamides, lamotrigine and antiepileptics. Patients who develop TEN are genetically predisposed to do so in response to certain drugs and therefore react on first exposure, usually 14 to 21 days after initiation of the drug. In some cases, however, no drug cause can be identified.
{kind=link}
Management
The use of oral prednisone in TEN is controversial; other immunosuppressive agents such as cyclosporine appear to be more effective.1 The use of single doses of tumour necrosis factor alpha (TNFα) inhibitors has recently been described as a successful therapeutic strategy in the management of TEN.2
Outcome
Upon arrival at hospital, the patient’s lamotrigine treatment was ceased. A skin biopsy was performed, which demonstrated the full thickness epidermal necrosis typical of TEN. A single dose of adalimumab 40 mg was given immediately and she was transferred to the burns unit.
Over the next 48 hours the patient’s blistering ceased. She was treated with supportive care, wound dressings and intravenous fluids. An ophthalmologist was consulted, and corticosteroid eye drops were initiated for the ocular symptoms. The vaginitis was treated with corticosteroid pessaries. The patient was discharged from the burns unit after a week and she recovered without sequelae.
References
1. Shokeen D. Cyclosporine in SJS/TEN management: a brief review. Cutis 2016; 97: E17-E18.
2. Paradisi A, Abeni D, Bergamo F, Ricci F, Didona D, Didona B. Etanercept therapy for toxic epidermal necrolysis. J Am Acad Dermatol 2014; 71: 278-283.
Skin conditions
Drug reactions