Managing hip pain in young adults during the COVID-19 pandemic

Despite the social distancing restrictions currently in place as a result of the COVID-19 pandemic, GPs can still use telehealth to assess hip pain in young adults. This article presents a practical review for GPs considering nonoperative intervention or referral to an orthopaedic surgeon.
Many causes of hip pain in young adults are amenable to telehealth consultations. A short history allows the clinician to get a sense of the potential problem and of any necessary investigations.
Although remote examination is not ideal, asking the patient to point to the painful area will give a clue as to whether the problem relates to intra-articular, extra-articular or referred pathology. Appropriate investigations can be ordered and viewed online.
‘Common things occur commonly’
Young adults (15 to 50 years of age) might present to their GP with pain in or around the hip joint. Over the past 20 years, we have learned a lot more about the differential diagnosis, natural history and management options for hip pain.
Both the assessment of an ‘at-risk’ hip and the development of a management plan can be done over the phone.
History
Some areas to keep in mind and ask about while taking a patient history over the phone include:
- Recent injuries. Pain developing after prolonged exercise might indicate a stress injury to bone or muscle strain.
- Childhood hip problems. Dysplasia, Perthes disease or slipped epiphysis can lead to impingement and early osteoarthritis (OA).
- Pain while sitting in a car, on a plane or at the theatre. This might indicate labral pathology.
- Excess alcohol or prolonged steroid use. These might indicate avascular necrosis (AVN).
- Pain at night while resting. This could point to AVN, severe OA or, rarely, a tumour.
- Other affected joints. This is possibly due to inflammatory arthritis.
- Difficulty bearing weight. Think of fracture, arthritis, AVN, infection or tumour.
Where is the pain?
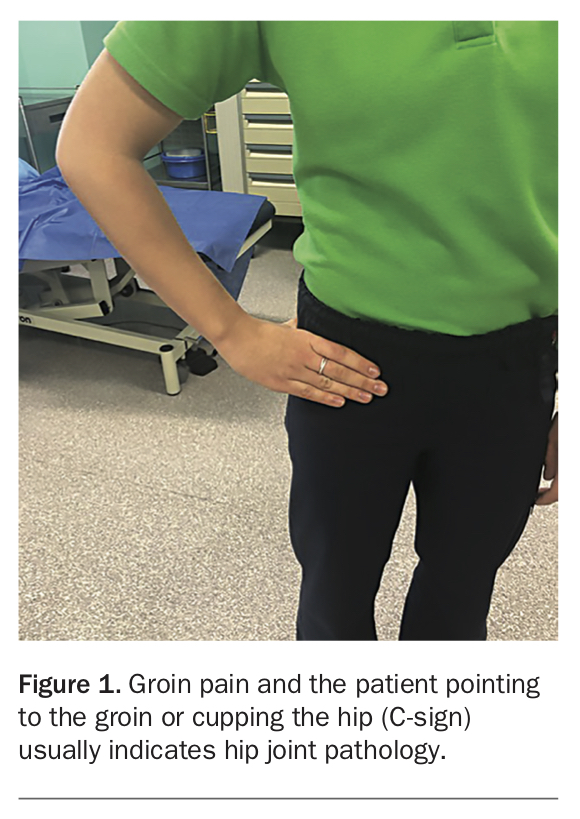
Groin pain, with the patient pointing to the groin or cupping the hip (C-Sign), usually indicates hip joint pathology (Figure 1).
{kind=link}
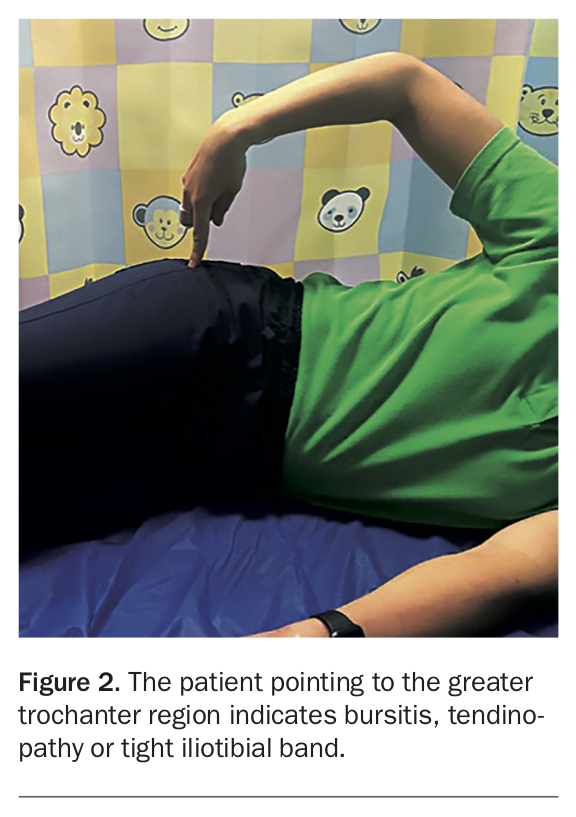
If the patient points to the greater trochanter, it is suggestive of bursitis, tendinopathy or tight iliotibial band (Figure 2).
{kind=link}
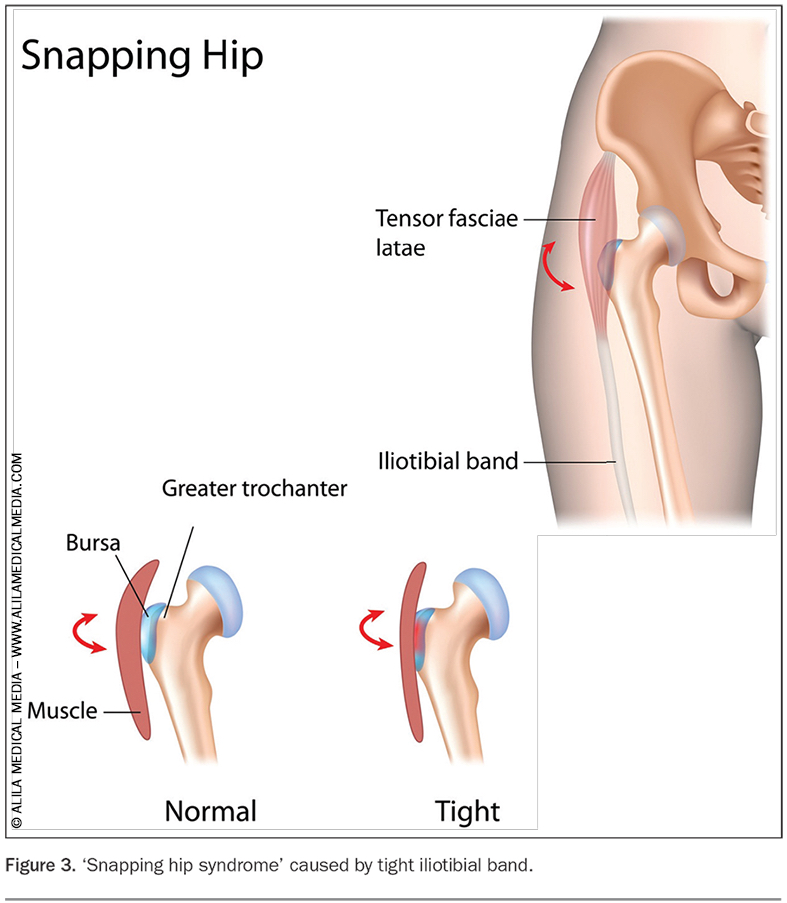
A ‘popping or clunking’ hip, with the patient pointing to the trochanter or groin, indicates the ‘snapping hip syndrome’ of either the tight iliotibial band snapping over the greater trochanter (lateral) or the tight iliopsoas tendon snapping over the front of the hip (groin) (Figure 3).
{kind=link}
Medial adductor muscle pain is usually related to an acute strain injury.
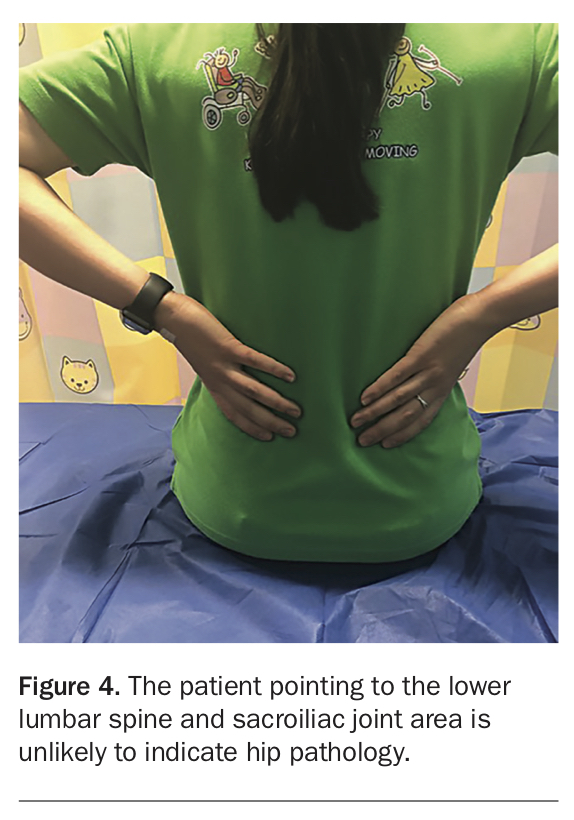
The patient pointing to the lower lumbar spine and sacroiliac joint area, is unlikely to indicate hip pathology (Figure 4).
{kind=link}
Pain radiating down past the knee to the lower leg, ankle and foot is more likely to be spinal pain.
Examination
Some physical examination procedures can be observed using the patient’s or their companion’s mobile phone:
- Palpation of the most tender area
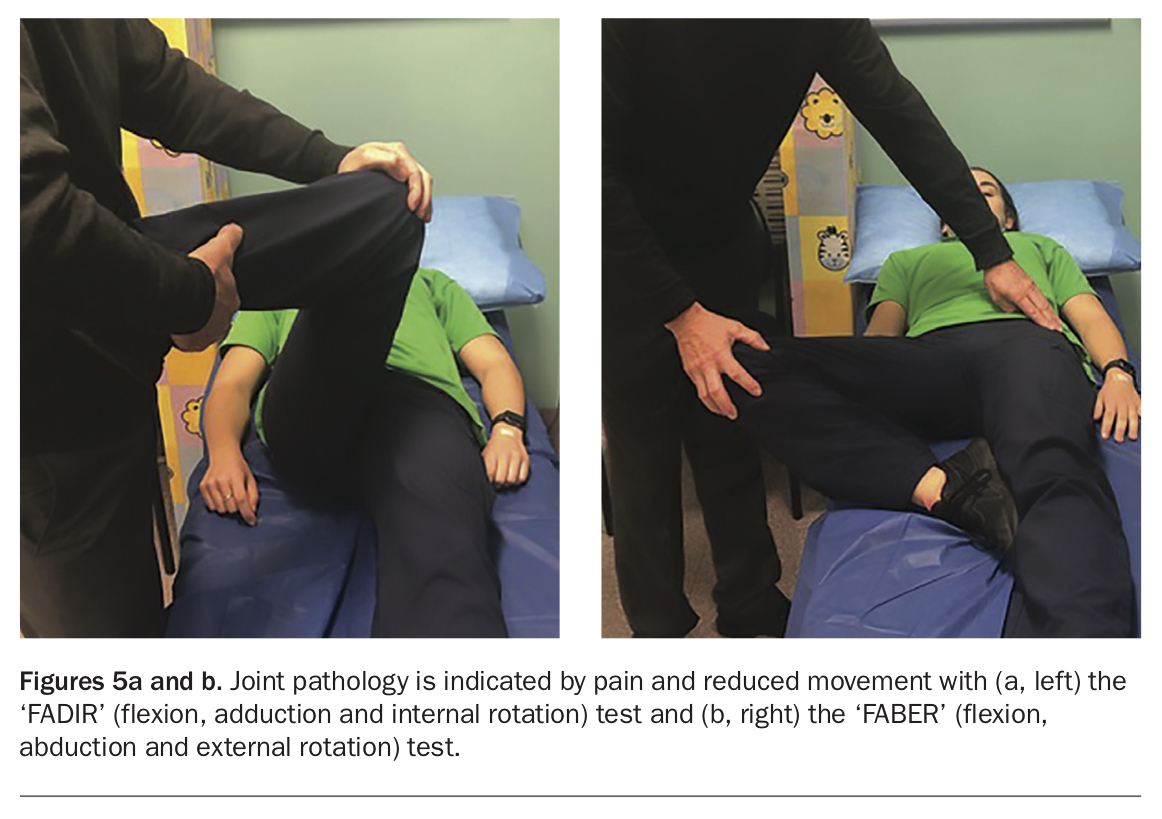
- Checking for asymmetry between the hips in the range of motion. Joint pathology is indicated by pain and reduced movement with the ‘FADIR’ (flexion, adduction and internal rotation) impingement test (Figure 5a) and the ‘FABER’ (flexion, abduction and external rotation) test (Figure 5b).
{kind=link}
Differential diagnosis – common causes
Conditions inside the hip joint
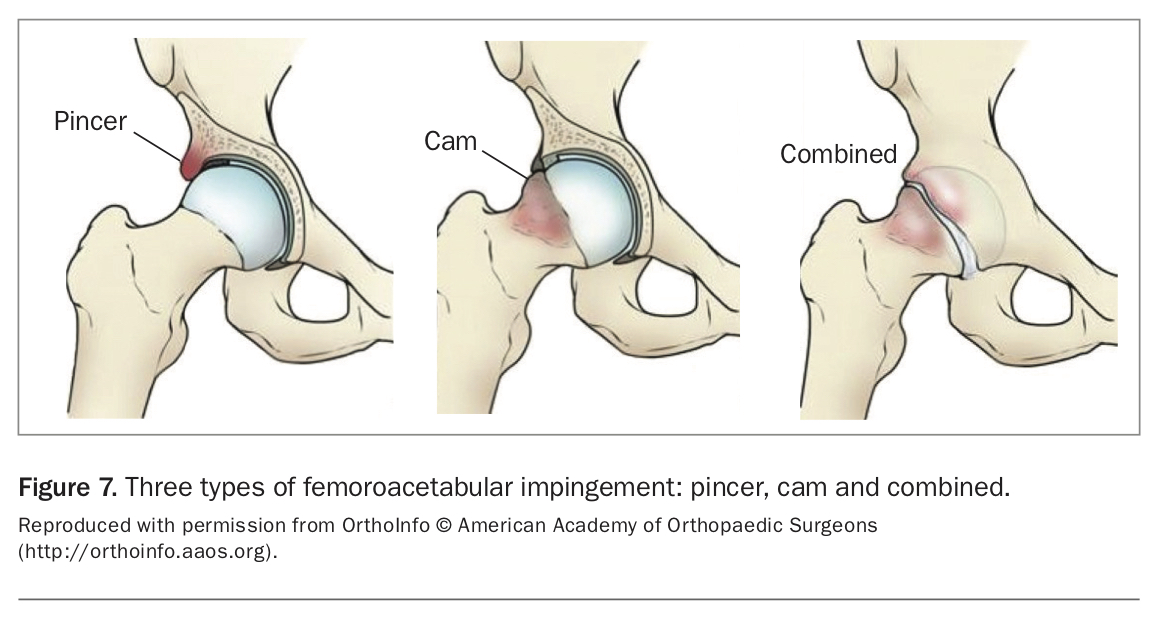
- femoroacetabular impingement (FAI) causing wear and tear
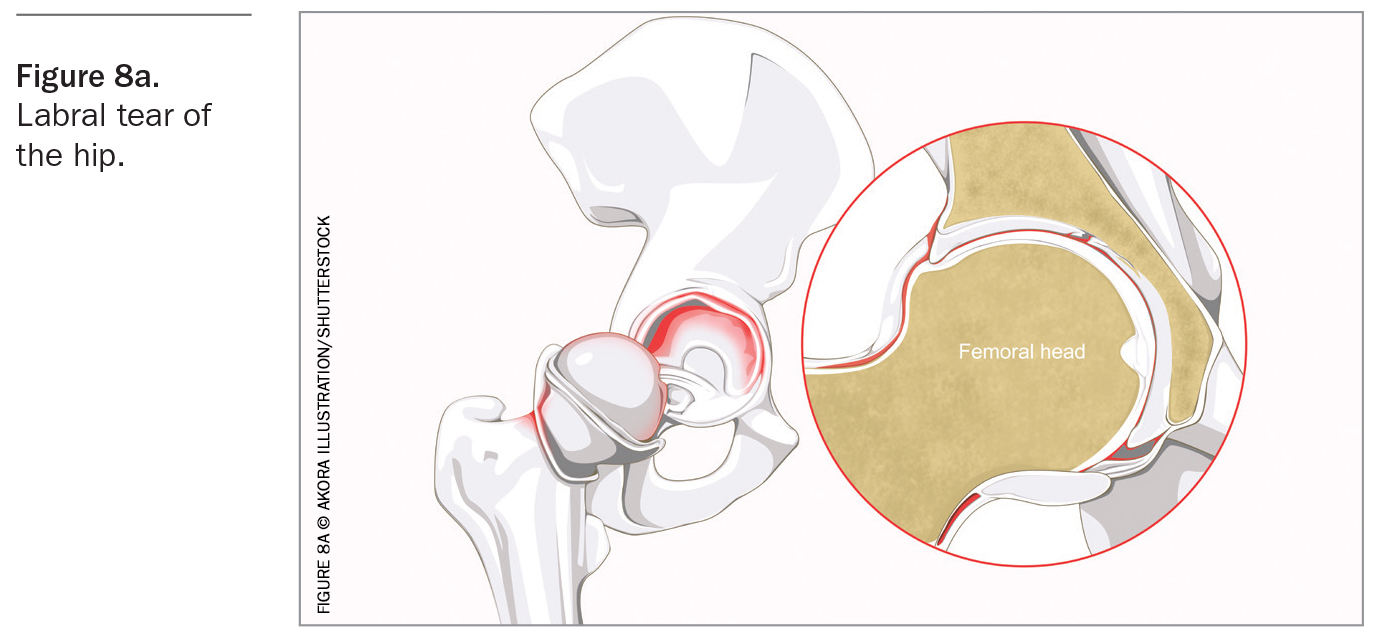
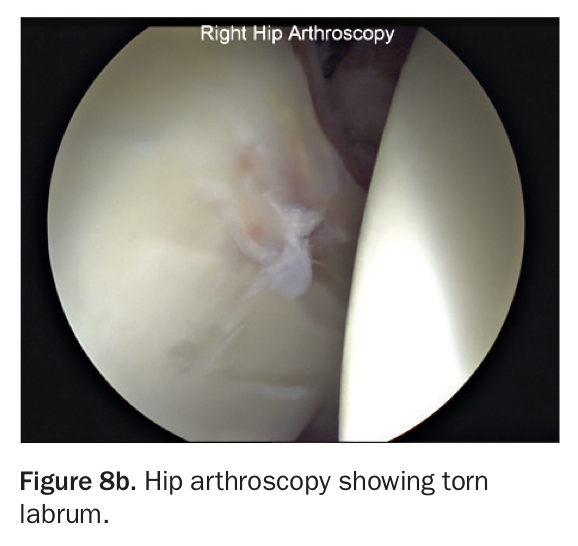
- labral tear
- AVN
- early OA
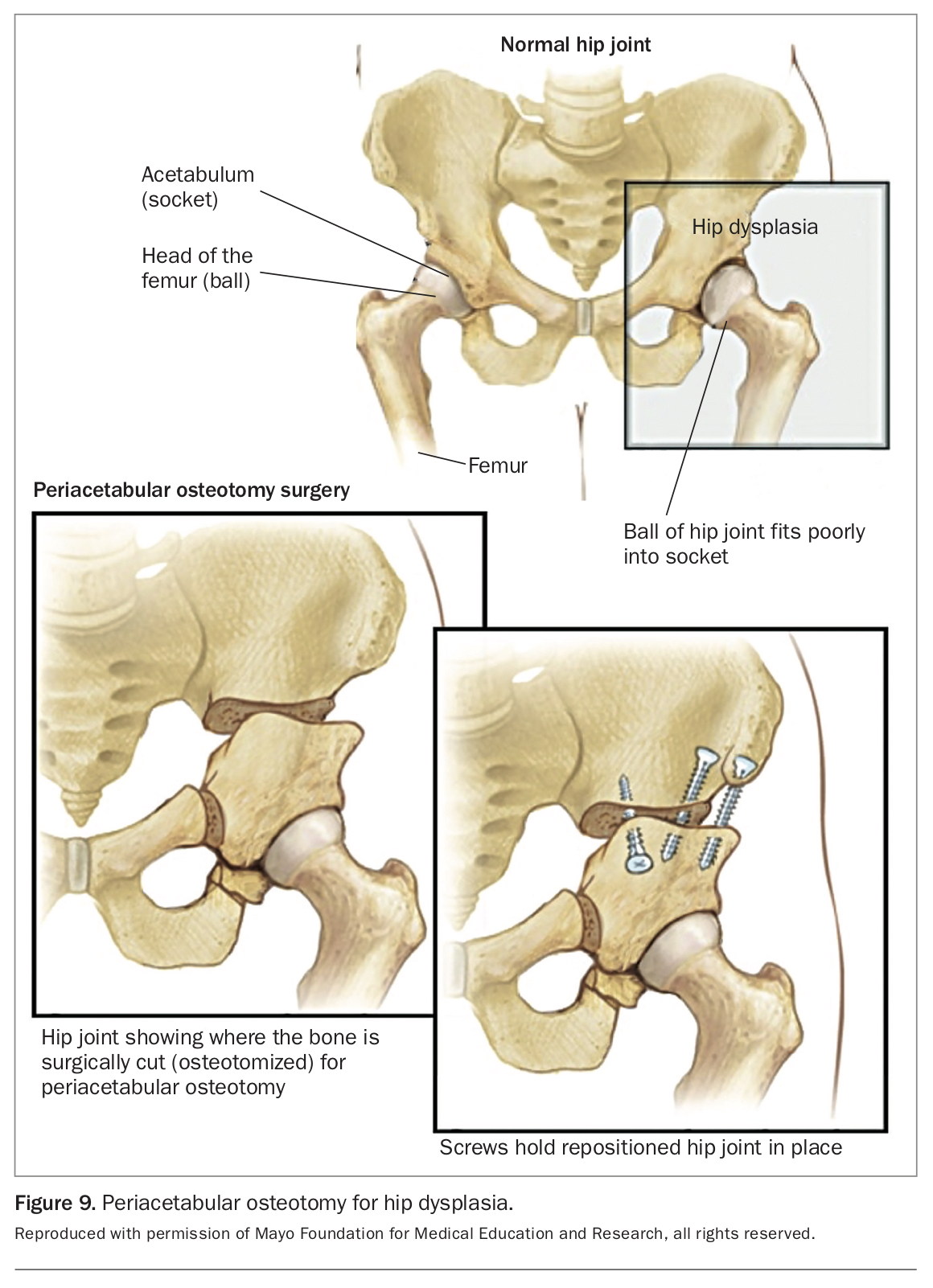
- developmental dysplasia of the hip (DDH) and secondary labral tear
- synovial pathology – less common – includes infection, inflammatory arthritis, pigmented villonodular synovitis or synovial chondromatosis.
Conditions outside the hip joint
- trochanteric bursitis/tendinopathy
- snapping hip
- stress fracture
- muscle tears
- referred pain from spine or abdomen
- deep gluteal syndrome (piriformis and other glutealmuscle entrapment of the sciatic nerve)
- inflammatory sacroiliitis
- osteitis pubis.
Investigations
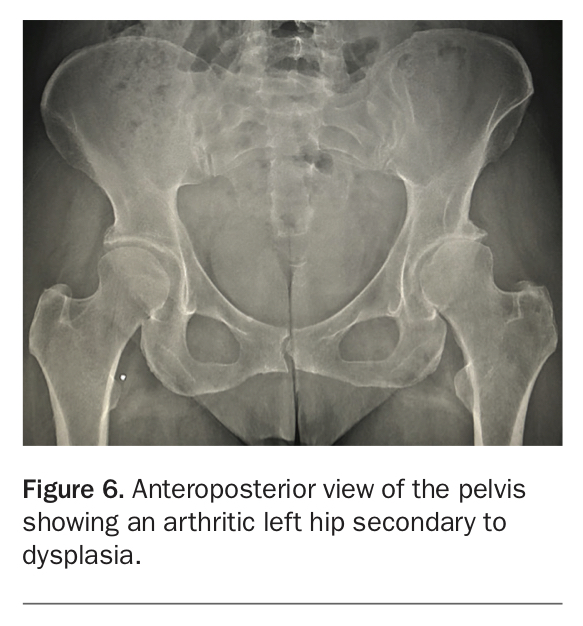
Always start with AP (anteroposterior) pelvis and lateral hip x-rays (Figure 6).
{kind=link}
If the x-ray is normal, an MRI scan is the investigation of choice.
Management plan
Nonoperative
Soft tissue injuries, tendinopathy, bursitis, snapping hip, nondisplaced labral tears, deep gluteal syndrome and early arthritis with no predisposing cause of FAI or DDH, are best treated nonoperatively with physiotherapy, activity modification, NSAIDs and, possibly, imaging-guided steroid injections.
Specialist referral
It is important to refer early when pain is not improving with nonoperative therapies. A patient with a diagnosis of FAI, AVN, dysplasia or stress fracture will benefit from early referral. This might enable joint-preserving treatments before OA develops.
FAI and hip dysplasia are treatable. Referral to an orthopaedic surgeon for elective surgery might prevent or delay OA.
Operative intervention
Femoroacetabular impingement (FAI)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Avascular necrosis
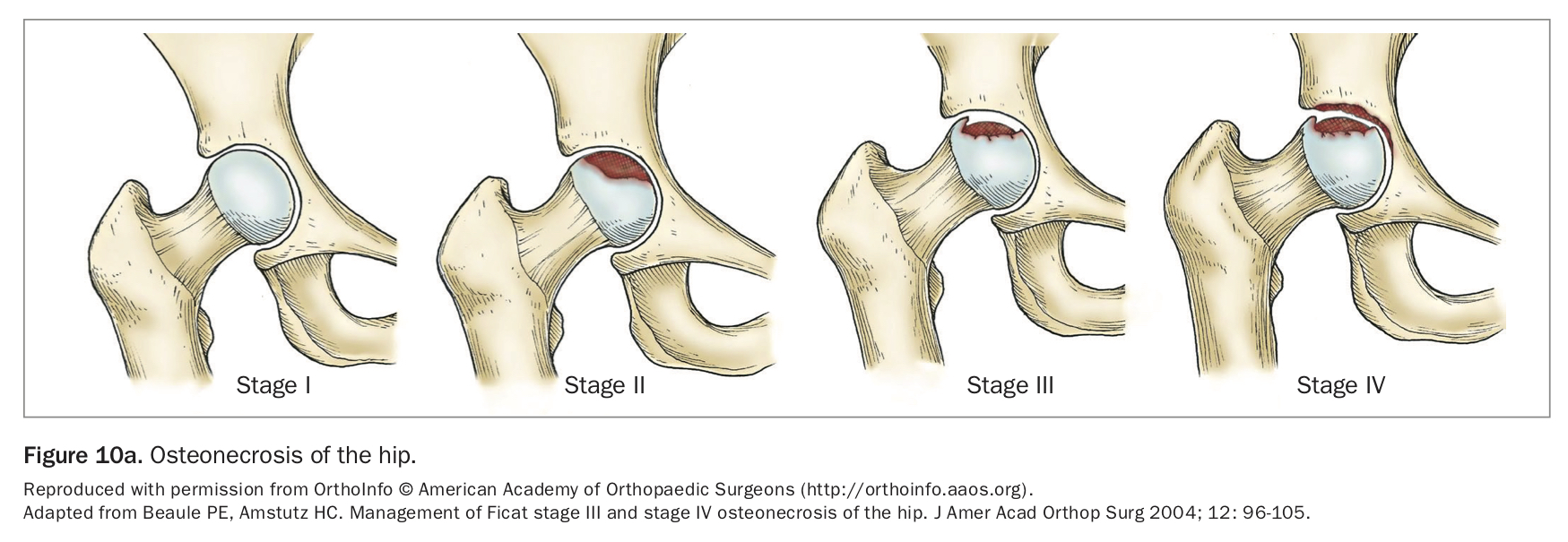
Recent advances in managing avascular necrosis hold promise for preventing or delaying its progression (Figure 10a) and reducing its associated morbidity.
{kind=link}
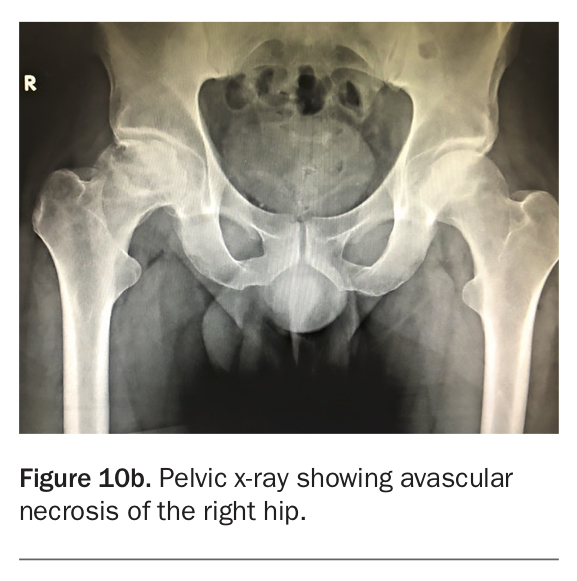
Early referral and surgical intervention are important to avoid femoral head collapse (Figure 10b).6
{kind=link}
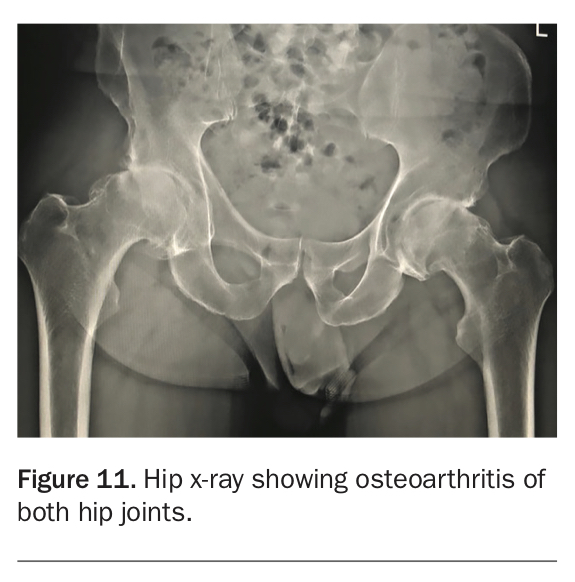
Established hip osteoarthritis and hip replacement
Today’s hip replacement surgery, using modern bearings, has excellent outcomes in patients under 55 years of age (and even, where indicated, in teenagers) (Figure 11 and Figure 12). Although there is no urgency for surgical intervention, clinical evaluation – with particular emphasis on the patient’s pain profile and the pain’s adverse effects on quality of life – is important.
{kind=link}
{kind=link}
The old philosophy of denying surgery until the patient is ‘much older’ no longer applies.
Hip replacement outcomes have proven excellent in restoring quality of life and relieving pain, with good long-term outcomes.
Considering that modern surgery has shown revision rates for young patients comparable to those of older patients, the former should also be afforded the opportunity to live pain free.7,8
Conclusion
Hip pain in a young adult may significantly adversely affect their quality of life. Establishing a likely cause – on history and examination, aided with a standard pelvic x-ray and possibly an MRI – would allow the GP to reach a definitive diagnosis. Management and treatment following the above guidelines would enable appropriate nonoperative or operative interventions.
Telehealth consultations are a practical alternative for making a diagnosis and advising on future action. MT