Pancreatic cystic lesions: sorting benign from malignant

Pancreatic diseases
Pancreatic cysts are a common incidental finding on imaging and may signify benign, premalignant or malignant disease. It is therefore important to investigate in an expert environment to identify the likely pathology and manage accordingly.
- Pancreatic cysts are a common incidental finding on imaging and may signify benign, premalignant or malignant disease.
- Early referral to a high-volume pancreatic unit is recommended for all patients with a pancreatic cyst.
- Triple-phase CT scan of the abdomen or gadolinium- enhanced MRI with MR cholangiopancreatography are the most appropriate imaging modalities for all patients with pancreatic cysts.
- As the malignant potential of pancreatic cysts varies, surgical intervention is recommended in selected cases only.
- Patients whose lesions are not resected should undergo surveillance under the close supervision of a specialist pancreatic unit.
Picture credit: © 3D4Medical/Medical Images
With the widespread use of cross-sectional imaging to evaluate abdominal symptoms, the incidental finding of cystic lesions of the pancreas is increasing. Although most pancreatic cysts are benign, some have malignant potential or are malignant at the time of diagnosis. Recommended treatment depends on the perceived risk of malignancy and presence of symptoms, and ranges from careful observation to pancreatic resection. For this reason, it is essential that patients undergo an appropriate ‘work-up’ in a high-volume institution with multidisciplinary specialist expertise in pancreatology. Sources of information on high-volume pancreatic surgical centres in Australia are shown in Box 1.
{kind=link}
Approximately 20 different types of pancreatic cystic lesion have been described.1 A few of these account for 90% of all pancreatic cystic lesions and are the focus of this article: pancreatic pseudocyst, serous cystic neoplasm, mucinous cystic neoplasm, intraductal papillary mucinous neoplasm (IPMN) and solid pseudopapillary neoplasm. The investigation and follow up of patients with these pancreatic cystic lesions are outlined.
Pancreatic pseudocyst
Pancreatic pseudocysts are collections of enzyme-rich pancreatic fluid, enclosed by a wall of fibrous or granulation tissue with no epithelial lining. Typically, pancreatic pseudocysts develop within or adjacent to the pancreas at least four weeks after an episode of pancreatitis.2 Pseudocysts are so named because they lack the epithelial lining that characterises true cysts.
Epidemiology and pathogenesis
Pancreatic pseudocysts account for the vast majority of cystic lesions in the pancreas. They affect up to 25% of patients who have a bout of pancreatitis. Most (85%) pseudocysts are single lesions, but some patients have multiple pseudocysts.3
Pseudocysts occur due to leakage of pancreatic juice from regions of inflamed pancreas or disrupted pancreatic duct. The most common causes, by far, are previous pancreatitis and trauma. Around half of these acute pancreatic fluid collections resolve spontaneously over time. However, in the remainder, the fluid collection persists, leading to the formation of a wall of nonepithelialised granulation tissue, creating a pseudocyst.
Clinical presentation and natural history
Symptoms of pseudocysts include abdominal pain and early satiety caused by gastric or duodenal compression. In a thin individual with a particularly large pseudocyst, an abdominal mass may be palpable. The diagnosis of pseudocyst should be suspected if there is continued abdominal pain, with or without a raised serum lipase level, persisting after resolution of acute pancreatitis.
The natural history of pseudocysts depends largely on their size. Around half of all pseudocysts resolve spontaneously. Nearly all pseudocysts less than 4 cm in diameter resolve spontaneously, but those that are greater than 10 cm in diameter are highly unlikely to resolve without intervention.4
Pseudocysts may give rise to complications that include infection, rupture and pseudoaneurysms of adjacent arterial structures (e.g. splenic, gastroduodenal and pancreaticoduodenal arteries). These pseudoaneurysms may subsequently bleed and require angiographic embolisation.
Investigation
On imaging, pseudocysts appear as well-circumscribed round structures with homogeneous fluid density surrounded by a thin-walled capsule. If the diagnosis is unclear on CT imaging then an endoscopic ultrasound (EUS) examination may be performed. EUS-guided fine-needle aspiration of pseudocyst contents is expected to reveal a low level of carcinoembryonic antigen but a high amylase concentration.
Treatment
Intervention is indicated when a pseudocyst is causing symptoms or complications, is increasing in size or is larger than 5 cm in diameter and has not decreased in size for longer than six weeks. Minimally invasive options for pseudocyst drainage are favoured, including endoscopic drainage. This can be achieved in most cases with the assistance of EUS by inserting one or more double pigtail stents or a larger covered bi-flanged metal stent through the posterior wall of the stomach into the pseudocyst.
Larger pseudocysts with dependent sections may require laparoscopic or open surgery to create a communication between the pseudocyst and the gastrointestinal tract allowing continuous drainage (e.g. cystojejunostomy or cystogastrostomy).
Serous cystic neoplasm
Serous cystic neoplasms are glycogen-rich lesions arising from the pancreas with extremely rare malignant potential.
Epidemiology and pathology
Serous cystic neoplasms account for 10 to 15% of all pancreatic cystic neoplasms and 1 to 2% of all pancreatic neoplasms. They affect mainly women aged in their 50s
or 60s.
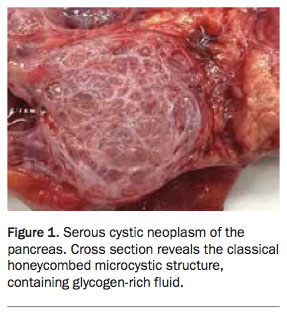
On examination, serous cystic neoplasms appear as multiloculated lesions characterised by a microcystic architecture that gives rise to a honeycomb appearance (Figure 1), although oligo- and macrocystic varieties have also been described. They contain serous fluid free of mucin, surrounded by cuboidal epithelium. Characteristically, the lining epithelium contains glycogen. Any part of the pancreas can be involved.
{kind=link}
Clinical presentation and natural history
Small serous cystic neoplasms are asymptomatic, but large lesions may cause nonspecific abdominal pain. Early satiety may occur if the lesion is large enough to cause gastric or duodenal compression. Multiple serous cystadenomas may occur in patients with von Hippel–Lindau syndrome.
Serous cystic neoplasms are almost always benign, with malignant disease (serous cystadenocarcinoma) rarely described. If followed up with imaging over time, most serous cystic neoplasms remain stable, but up to 37% may show slow growth (approximately 4 mm per year).5
Investigation
On CT or MRI, serous cystic neoplasms classically have a spongy honeycomb appearance. A central calcified scar is also often seen. Macro- or oligocystic varieties can be difficult to differentiate from lesions such as branch-duct IPMN (described below). If the diagnosis is uncertain then EUS-guided fine-needle aspiration should be performed. In patients with serous cystic neoplasm, this is expected to show serous fluid with low concentrations of amylase and carcinoembryonic antigen.
Treatment
Because of the benign nature of serous cystic neoplasms, a conservative approach to management is appropriate for most patients. However, pancreatic resection may be performed in some patients with large symptomatic lesions, diagnostic uncertainty on imaging and EUS or rapid growth of the lesion.
Mucinous cystic neoplasm
Mucinous cystic neoplasms are mucin-producing lesions of the pancreas with malignant potential.
Epidemiology and pathology
Mucinous cystic neoplasms account for 2 to 5% of all pancreatic exocrine tumours, with a female-to-male ratio of 20:1. These lesions generally affect women aged in their 40s.
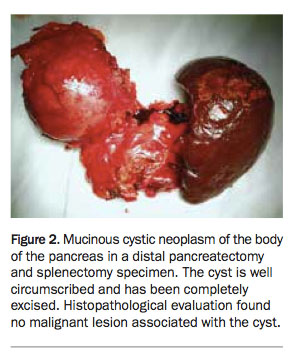
Mucinous cystic neoplasms are large thick-walled septated cysts containing abundant mucin, lined by tall columnar epithelium surrounded by ovarian-type stroma. In rare cases, these lesions affect areas other than the body and tail of the pancreas (Figure 2). They are almost always unifocal.
{kind=link}
Clinical presentation and natural history
Large mucinous cystic neoplasms may cause abdominal pain and early satiety. However, most of these lesions are asymptomatic and found incidentally on abdominal imaging. Significant weight loss and other constitutional symptoms should raise suspicions of associated malignancy.
The most concerning feature of mucinous cystic neoplasms is the risk that they harbour malignancy, which occurs in 15% of cases. Invasive mucinous cystic neoplasm tends to affect an older cohort of patients than noninvasive forms. Larger lesions tend to have a higher risk of harbouring malignancy than lesions smaller than 4 cm.6
Investigation
Mucinous cystic neoplasms are characterised on CT and MRI by a macrocystic appearance, containing a few septa with some peripheral ‘eggshell’ calcifications. Imaging features associated with a higher risk of malignancy in mucinous cystic neoplasms include septations, enhancement of the cyst wall, larger size and the presence of mural nodules. Analysis of cyst fluid obtained from mucinous cystic neoplasms through EUS-guided fine-needle aspiration usually shows high levels of carcinoembryonic antigen and low amylase levels.
Treatment
Resection is recommended for all surgically fit patients with mucinous cystic neoplasm. Resection is fully curative in patients with lesions with no malignant component, but has a five-year disease-specific survival of 57% in patients with mucinous cystic neoplasm-associated malignancy.6 Therefore, timely resection of these lesions is imperative.
Intraductal papillary mucinous neoplasm
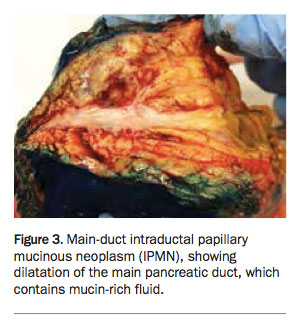
IPMN is a mucin-producing lesion arising from the main duct or branch duct of the pancreas, with a variable risk of malignant transformation (Figure 3).
{kind=link}
Epidemiology and pathology
IPMN accounts for 15 to 30% of all cystic neoplasms of the pancreas, affecting men and women in equal proportions, usually when aged in their 60s.
IPMN may be classified either according to the level of pancreatic duct from which it arises (main-duct, branch-duct or mixed IPMN) or based on the lining epithelium (intestinal, gastric, pancreatic or oncocytic). Most intestinal-type IPMNs correspond to main-duct IPMN and most gastric-type IPMNs correspond to branch-duct IPMN.
IPMNs can be graded according to the level of atypia seen in the ductal epithelium: low-, intermediate- or high-grade dysplasia. The major prognostic factor, however, is the presence of invasive carcinoma, which generally has a better postresection prognosis (45% five-year survival) than pancreatic ductal adenocarcinoma (15% five-year survival), owing to earlier staging at the time of diagnosis.
Clinical presentation
Although mostly IPMNs are found incidentally on imaging, patients occasionally present with symptoms related to ductal occlusion, including pancreatitis and abdominal pain. Cystic lesions centred around the head of the pancreas may cause painless jaundice.
Investigation
Triple-phase abdominal CT and MRI with MR cholangiopancreatography (MRCP) are the imaging modalities of choice in assessing IPMN. Main-duct IPMN appears as either diffuse or segmental dilatation of the main pancreatic duct. Branch-duct IPMN appears as a cystic lesion and may be multifocal. MRCP may reveal a communication between the cyst and the main pancreatic duct, but this is not always seen. The presence of mural nodules in both main- and branch-duct IPMN should raise suspicion of an associated malignancy.
EUS is useful for characterising features associated with a high risk of malignancy, including mural nodules. EUS-guided fine-needle aspiration of cyst contents generally reveals a high concentration of carcinoembryonic antigen. Theoretically, communication with the pancreatic duct leads to a high amylase level, but this is not always the case.
Treatment
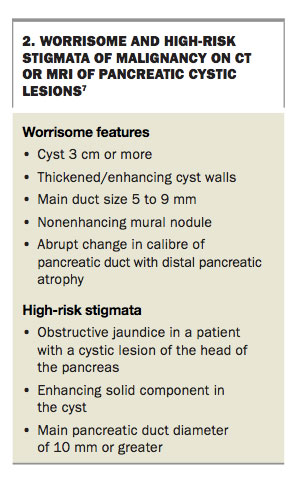
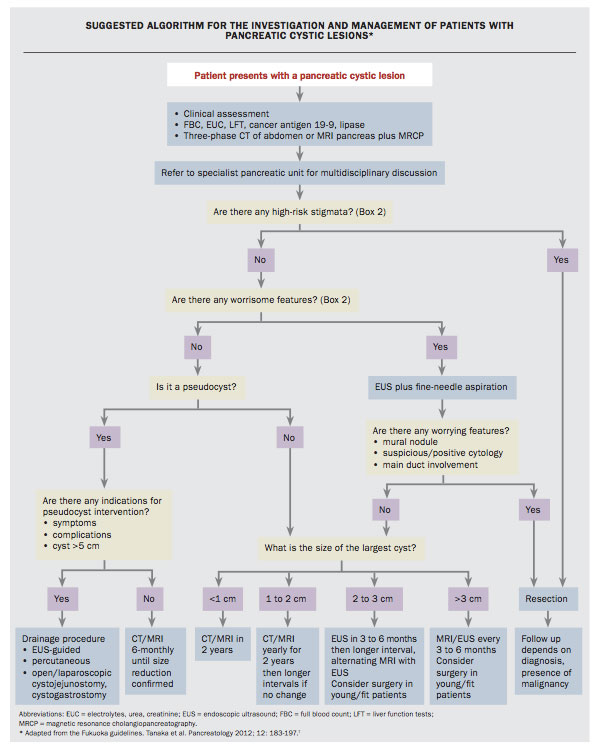
The optimal management of a patient with IPMN has been much debated, leading most recently to the 2012 Fukuoka guidelines.7 These list worrisome and high-risk features on imaging that assist clinicians in deciding further work-up, surveillance and whether surgical resection is indicated (Box 2). The presence of high-risk stigmata should lead to surgical resection in surgically fit individuals. The presence of worrisome features on imaging should lead to further evaluation with EUS and fine-needle aspiration. A lesion with no worrisome or high-risk stigmata should undergo surveillance according to its size (Flowchart).
{kind=link}
{kind=link}
The procedure most often recommended to patients is partial pancreatectomy (Whipple’s procedure or distal pancreatectomy) with frozen section of the neck margin to ensure the absence of high-grade dysplasia or malignancy. As IPMNs may involve the duct system in a multifocal manner, the remnant pancreas then undergoes surveillance with serial imaging. Total pancreatectomy is associated with major long-term morbidity and should be reserved for highly selected patients.
Solid pseudopapillary neoplasm (Frantz tumour)
Solid pseudopapillary neoplasm, also known as Frantz tumour, is a rare indolent pancreatic tumour with cystic and solid components and potential for malignant behaviour.
Epidemiology and pathology
Solid pseudopapillary neoplasm accounts for only 2.5% of resected pancreatic tumours, and primarily affects young women (mean age, 22 years), with a female to male ratio of nearly 10:1.8
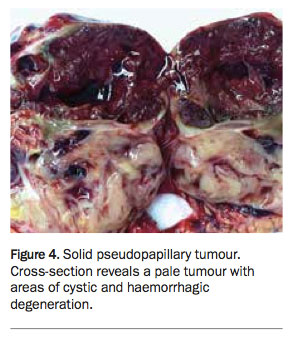
Solid pseudopapillary neoplasms are generally large at the time of diagnosis, affecting any part of the pancreas, and associated with metastatic disease in 6% of patients.9 On cross-section, these tumours appear heterogeneous, with haemorrhagic cysts interspersed among pale areas of solid tumour (Figure 4).
{kind=link}
Clinical presentation
Because of the size of the lesion, patients usually have symptoms at diagnosis, presenting mainly with abdominal pain or an abdominal mass. Weight loss is an uncommon feature of this disease.
Investigation
On CT or MRI, solid pseudopapillary neoplasms appear as well-circumscribed lesions with areas of cystic degeneration due to necrosis and haemorrhage.
Treatment
After complete surgical resection of solid pseudopapillary neoplasms, 85 to 95% of patients are cured. Although metastasis (and dissemination after rupture) have been reported, these lesions typically have indolent behaviour, and recurrence is exceptional. Metastatic disease should not preclude resection, as it would in patients with pancreatic ductal adenocarcinoma, because long-term survival is possible even under these circumstances.8
Investigation of pancreatic cystic lesions
A suggested algorithm for the investigation and management of patients with pancreatic cystic lesions is shown in the Flowchart.
Blood tests
- Blood tests recommended for all patients with a pancreatic cystic lesion include:
- full blood count
- serum urea, electrolytes and creatinine measurement
- liver function tests
- serum C-reactive protein, lipase and cancer antigen 19-9 (CA19-9) measurement.
Raised inflammatory marker levels in the context of abdominal pain and fevers in a patient with a known or suspected pseudocyst should raise concern for secondary infection. Liver function test results may be deranged if there is extrinsic bile duct compression from a pancreatic lesion, particularly if it is located in the head of the pancreas. A persistently elevated lipase level after resolution of an episode of pancreatitis should raise concern for the development of a pseudocyst. A raised CA19-9 level should raise concern for a pancreaticobiliary malignancy associated with the cystic neoplasm.
Imaging
The aims of imaging are to achieve a diagnosis, detect worrisome features or high-risk stigmata and assist with surgical planning. A triple-phase CT scan with fine slices through the pancreas (pancreatic protocol CT) or a gadolinium-enhanced MRI of the pancreas with MRCP is recommended. In Australia, GP-referred MRI of the pancreas with MRCP is not currently subsidised by the MBS.
CT is able to identify intracystic septations, nodules and calcifications. It is also valuable for identifying surrounding anatomy and vascular structures for surgical planning. However, MRI with MRCP has the advantage of being able to better define the relation of the cystic lesion to the pancreatic duct, an important feature when trying to distinguish between branch-duct IPMN and oligocystic serous or mucinous cystic neoplasm. In addition, MRI may be preferred for patients who require frequent imaging surveillance, to avoid radiation exposure.
Endoscopic ultrasound and fine-needle aspiration
EUS is a highly sensitive but invasive imaging modality that involves the passage of an echoendoscope into the stomach and duodenum, enabling the entire pancreas to be visualised in great detail. EUS is indicated for all pancreatic cysts with worrisome features and for those larger than 3 cm without worrisome features. As with conventional ultrasound, EUS is highly operator dependent. It is also associated with procedural risks, including gastrointestinal perforation and haemorrhage, and therefore needs to be performed in a unit with high-volume expertise in this technique.
EUS-guided fine-needle aspiration of pancreatic cyst contents allows cyst fluid to be evaluated for cytology and carcinoembryonic antigen and amylase levels. A carcinoembryonic antigen level greater than 192 mg/mL has been shown to be highly predictive of a mucinous lesion (i.e. mucinous cystic neoplasm and IPMN) but does not predict the presence of malignant disease.10 A raised amylase level in cyst fluid usually signifies communication of the cyst with the main pancreatic duct (as in pancreatic pseudocyst and IPMN). However, the cyst fluid amylase level is not consistently elevated in IPMN, and mucinous cystic neoplasms have also been shown to have high cyst fluid amylase levels. Serous cystic neoplasm is associated with low carcinoembryonic antigen and amylase levels in cyst fluid.
Follow up
Depending on the diagnosis, patients may require short- or long-term follow up. All follow up should involve a pancreatic surgeon.
Patients with pancreatic pseudocysts should be followed up with six-monthly CT or MRI until symptoms have abated, and a clear trajectory towards resolution of the pseudocyst has been established. Those with unresected serous cystic neoplasms should also be followed up with imaging according to cyst size (see the Flowchart).
As resection is curative for serous cystic neoplasms, patients who have undergone resection do not need long-term follow up, except in the rare circumstance of serous cystic neoplasm-associated malignancy. Patients who have undergone resection of mucinous cystic neoplasm similarly do not require long-term follow up as long as there is no associated malignancy.
Patients with unresected branch-duct IPMN should be followed up with serial imaging according to lesion size (Flowchart). For those who have undergone IPMN resection, follow up depends on whether IPMN is present in the remnant pancreas. Those with a remnant pancreas free of known IPMN may be followed up with serial imaging at two years and then five years after resection to confirm there is no new recurrence. Patients with IPMN in the remnant pancreas should be followed up similarly to those with unresected IPMN.
Patients with a solid pseudopapillary neoplasm with no invasive features do not require long-term follow up after resection. However, the presence of invasive features or anaplastic dedifferentiation heralds a higher risk for developing metastatic disease, and therefore these patients should be followed up with serial imaging every six to 12 months.
Patients with mucinous cystic neoplasms or IPMN with an invasive component should be followed up similarly to patients with pancreatic ductal adenocarcinoma, which was discussed in the April 2016 issue of Medicine Today.11
Conclusion
There are many causes of pancreatic cystic lesions, which are associated with varying degrees of malignant potential. Surgical resection is required only in selected patients, and conservative management with close observation is appropriate in many cases. For this reason, it is imperative that patients are investigated systematically in a unit with surgeons, gastroenterologists, radiologists, oncologists and pathologists with high-volume experience in pancreatic pathology. From a GP’s perspective, any patient with a newly diagnosed pancreatic cystic lesion should have a triple-phase CT scan as a minimum investigation and referral to a pancreatic surgeon for ongoing management and surveillance. MT
References
- Kosmahl M, Pauser U, Peters K, et al. Cystic neoplasms of the pancreas and tumor-like lesions with cystic features: a review of 418 cases and a classification proposal. Virchows Arch 2004; 445: 168-178.
- Working Group IAPAPAAPG. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology 2013; 13: e1-15.
- Brun A, Agarwal N, Pitchumoni CS. Fluid collections in and around the pancreas in acute pancreatitis. J Clin Gastroenterol 2011; 45: 614-625.
- O’Malley VP, Cannon JP, Postier RG. Pancreatic pseudocysts: cause, therapy, and results. Am J Surg 1985; 150: 680-682.
- Jais B, Rebours V, Malleo G, et al. Serous cystic neoplasm of the pancreas: a multinational study of 2622 patients under the auspices of the International Association of Pancreatology and European Pancreatic Club (European Study Group on Cystic Tumors of the Pancreas). Gut 2016; 65: 305-312.
- Goh BK, Tan yM, Chung yF, et al. A review of mucinous cystic neoplasms of the pancreas defined by ovarian-type stroma: clinicopathological features of 344 patients. World J Surg 2006; 30: 2236-2245.
- Tanaka M, Fernandez-del Castillo C, Adsay V, et al. International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology 2012; 12: 183-197.
- Papavramidis T, Papavramidis S. Solid pseudopapillary tumors of the pancreas: review of 718 patients reported in English literature. J Am Coll Surg 2005; 200: 965-972.
- Nguyen NQ, Johns AL, Gill AJ, et al. Clinical and immunohistochemical features of 34 solid pseudopapillary tumors of the pancreas. J Gastroenterol Hepatol 2011; 26: 267-274.
- Nagula S, Kennedy T, Schattner MA, et al. Evaluation of cyst fluid CEA analysis in the diagnosis of mucinous cysts of the pancreas. J Gastrointest Surg 2010; 14: 1997-2003.
- Gundara J, Samra JS, Mittal A. Pancreatic ductal adenocarcinoma: optimal patient management. Med Today 2016; 17(4): 14-20.
COMPETING INTERESTS: None.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.