Codeine rescheduling and the GP

Since the recent rescheduling of codeine, patients who have been taking over-the-counter products are increasingly presenting to their GPs. For this reason, we are highlighting this article, which featured in a recent Medicine Today supplement.
- If a patient requests a codeine prescription, first establish the reason they take codeine and their pattern of use.
- If a patient has been using codeine regularly over a relatively long period (e.g. more than a month), assess for likely dependence.
- A taper from codeine (e.g. with symptomatic medication or a medication such as buprenorphine–naloxone)is a reasonable approach in the first instance where a diagnosis of codeine dependence is not established.
- When a patient clearly meets criteria for opioid dependence, with a well-established pattern of daily high-dose use, and taper approaches have failed, consider medication-assisted treatment for opioid dependence (e.g. with buprenorphine–naloxone), with the support of alcohol and drug services for nonaccredited prescribers.
On 1 February 2018, codeine became a prescription-only medication in Australia. Many patients who take codeine are presenting to GPs and other healthcare providers asking for advice. Some patients may have been using codeine intermittently for acute pain in recommended doses, and others may have found themselves taking larger doses over a longer period (see the case of Julie in Box 1). This article outlines the recommended assessment and management strategies for patients who present with different levels of codeine use in general practice.
{kind=link}
Why, how much, how often and how long?
The first step with patients presenting with over-the-counter (OTC) codeine use is to understand the underlying symptoms or conditions for which they are using codeine and to determine how likely they are to need help in stopping codeine. Are they taking codeine occasionally for acute pain or daily for chronic pain? Are they taking codeine for nonpain reasons, such as in response to stress, anxiety or insomnia?
The next step is to assess the pattern of codeine use and ask patients what happens when they do not take it. This information will help determine whether they have developed opioid tolerance and show signs of opioid withdrawal on cessation. These symptoms may be part of a pattern of opioid dependence. However, opioid dependence (as defined by the International Classification of Diseases [ICD-10]) goes beyond neuroadaptation to opioids (with tolerance and withdrawal) to include behavioural components such as craving, continued use despite ill health or other harm and loss of control over use.
Patient assessment
Assessment of patients taking codeine should cover:
- current codeine use (reason, dose, route of administration, duration and symptoms on cessation)
- other medication and alcohol, nicotine and substance use
- mental health and physical comorbidities
- social circumstances
- physical examination (including signs of opioid toxicity and withdrawal; see Box 2)
- investigations (e.g. urine drug screen, liver function tests, full blood count)
- how difficult the patient thinks it may be to go without codeine and whether they experience opioid withdrawal symptoms when they go without codeine
- whether the patient is exceeding maximum doses, buying codeine from multiple pharmacies, obtaining prescriptions for codeine or other opioids or hiding their use from others.
{kind=link}
Identifying opioid dependence
The ICD-10 includes criteria to identify dependence. According to the ICD-10, opioid dependence is defined by the presence of three or more of the following features at any one time in the preceding year:
- a strong desire or sense of compulsion to take opioids
- difficulties in controlling opioid use
- a physiological withdrawal state
- tolerance
- progressive neglect of alternative interests or pleasures because of opioid use
- persisting with opioid use despite clear evidence of overtly harmful consequences.
There are other definitions of opioid dependence or ‘use disorder’ (e.g. the Diagnostic and Statistical Manual of Mental Disorders, 5th edition, [DSM-5]), but the central features are the same: loss of control over use, continuing use despite harm, craving, compulsive use, physical tolerance and dependence remain key in identifying problems.
Is the patient experiencing pain or opioid withdrawal?
For a patient who takes codeine regularly, it can be difficult to differentiate between the re-emergence of pain and the emergence of opioid withdrawal symptoms. Pain symptoms often increase during opioid withdrawal. Some patients describe taking codeine as ‘the only thing that works’, for example in self-management of persistent or recurrent headaches. In some cases, a detailed assessment can reveal that opioid overuse or withdrawal itself may be the cause of the headaches (medication overuse headache, Box 3).1 In other cases, patients have always used the ‘strongest’ product available and have never tried taking simple analgesics without codeine.
{kind=link}
Is the patient likely to need help in stopping codeine?
The assessment and management of patients who present with regular OTC codeine use is summarised in the Flowchart. Management approaches depend on the likelihood of opioid tolerance and dependence.
Patients who are unlikely to be codeine tolerant or dependent
Patients who are unlikely to be opioid dependent include those who have taken codeine intermittently for relief of acute pain, for example once a week or less often. For most people, simple OTC analgesics are as effective as combination analgesics containing low-dose codeine. A typical example of such a patient, Tom, is described in Box 4.
{kind=link}
Management principle: for patients who are unlikely to be opioid tolerant or dependent, give brief advice on the changes in codeine availability and other options for management of acute pain.
Patients with possible codeine tolerance and withdrawal but uncertain dependence
Some patients may have been taking codeine daily or on most days for at least a month, but do not have clear features of opioid dependence, as in the case of Harriet in Box 5. These patients describe codeine use only in the context of managing their pain. They take doses in the recommended range (albeit for a longer period than recommended), and they may not yet have tried to cease codeine.
{kind=link}
These patients may need medical assistance in ceasing codeine use. Reasons not to prescribe codeine or another opioid are outlined in Box 6.2 Depending on the patient’s level of codeine use, opioid tolerance, self-efficacy and resilience, either a trial of cessation with no medication or a short opioid taper assisted by a nonopioid medication may be appropriate. Alternative (nonopioid) pain management approaches should also be discussed.
{kind=link}
Management principle: in the absence of a clear diagnosis of opioid dependence, support attempts at ceasing codeine.
How useful is the codeine dose in diagnosing dependence?
The case of Harriet in Box 5 demonstrates that problems with codeine can emerge even at recommended doses. The dose of codeine taken may help indicate the degree of dependence and the likely severity of opioid withdrawal symptoms. However, codeine has variable metabolism. About one in 10 people of Caucasian background are considered ‘ultra-rapid metabolisers’ of codeine, converting codeine into larger dose of morphine than usual and being at risk of toxicity. At the other end of the spectrum, 5 to 10% of the population are ‘poor metabolisers’ and cannot convert codeine into morphine, therefore experiencing little analgesia.3,4
Variation in metabolism is linked to genetics, with the reported prevalence of ultra-rapid metabolisers ranging from 1 to 25%, depending on genetic background.3 Consequently, it is possible, albeit uncommon, to have a significant level of opioid tolerance while taking relatively low therapeutic doses of OTC codeine. For example, as few as eight tablets per day of OTC codeine has led to dependence requiring opioid agonist treatment. Similarly, opioid toxicity has been reported in patients taking relatively low daily doses of codeine. The patient’s symptoms on opioid cessation and assessment of other clinical indicators should drive the treatment approach as much as the codeine dose.
Patients who are likely to be codeine dependent
Patients who have been taking codeine regularly (at least daily and probably multiple times a day for months or years) are likely to have developed tolerance to codeine and may have developed dependence, as in the case of Ivana (Box 7). These patients may take codeine for pain or for nonpain reasons such as insomnia and to help with psychological distress.
{kind=link}
Other characteristics commonly associated with codeine dependence include:
- difficulty stopping or inability to imagine stopping codeine use
- emergence of withdrawal symptoms six to 12 hours after the last codeine dose
- self-medication with opioids for opioid withdrawal that has been self-diagnosed as re-emergence of pain (e.g. rebound headaches)
- other substance use disorders (more often alcohol, benzodiazepines and less frequently other opioids or other illicit drugs)
- concurrent mental health conditions.
Management principle: advise patients with significant codeine dependence to consider maintenance treatment with buprenorphine–naloxone or methadone, following national guidelines.5 Another option is detoxification. Address any concurrent mental health problems and investigate for possible adverse effects of high-dose ibuprofen or paracetamol, as relevant.
Management options for codeine dependence
Maintenance treatment with buprenorphine–naloxone or methadone (also termed substitution treatment) is indicated for the treatment of opioid dependence, including codeine dependence.5 Other opioids, such as oxycodone–naloxone, are not indicated in the treatment of opioid dependence. Most state and jurisdictional regulations preclude use of opioids other than methadone and buprenorphine (with or without naloxone) for the treatment of opioid dependence.
Detoxification is an alternative to maintenance treatment, particularly for patients who have less severe dependence and no medical problems such as liver, kidney and gastrointestinal complications due to the use of high doses of ibuprofen or paracetamol in codeine-containing products or other factors that increase the risk of relapse. For patients who have used larger doses of opioids and have established opioid dependence, short-term opioid tapering is associated with poorer treatment outcomes compared with maintenance treatment with opioid agonists.6 The low rates of success for short-term withdrawal and risk of overdose with loss of tolerance should be discussed with the patient. The patient should be advised that if codeine withdrawal management is unsuccessful then maintenance treatment with supervised buprenorphine–naloxone or methadone is indicated.
Concurrent mental health problems such as anxiety should be addressed. Options include face-to-face psychological support (e.g. through a mental healthcare plan) or online support (e.g. through services such as beyondblue). During initial withdrawal, psychosocial approaches are recommended before psychotropic medications, as opioid withdrawal symptoms can contribute to diagnostic uncertainty.
When a patient is codeine dependent, longer-term prescribing of opioids should be under the framework of supervised medication-assisted treatment of opioid dependence (e.g. with buprenorphine–naloxone or methadone). Clinicians should contact the local health department to confirm requirements in their jurisdiction before prescribing pharmacotherapy, in addition to checking electronic medical records and prescription monitoring records where these are available.
When patients report taking large doses of ibuprofen plus codeine or paracetamol plus codeine combination products, relevant investigations should be considered, particularly to assess for renal and hepatic impairment and for anaemia. A range of serious and even fatal consequences have been reported with long-term high-dose use of codeine combination products, including perforated gastric ulcer, hypokalaemia and liver failure.7
Weaning off codeine in an outpatient setting
An opioid taper may be appropriate for patients who:
- show evidence of physiological dependence to codeine but no clear diagnosis of opioid dependence
- are otherwise in good health and do not have concurrent comorbidities that warrant specialist assessment or admission for inpatient treatment
- have no other concurrent substance use disorders and are not using other psychoactive substances of concern
- have home and social environments that are safe, supportive and free from other substance use.
Patients who have significant comorbidity or concurrent substance use disorder may be best managed in a specialist drug treatment setting, in an outpatient setting through a shared-care arrangement, or with the input and support of health care providers and services specialising in treatment of substance use disorders.
An opioid taper can be considered as the first step in assessing opioid dependence when use has been in lower doses or over shorter periods, and other pharmacological approaches are not indicated. For an opioid taper to be indicated, the patient should describe a pattern of daily or near daily codeine use for at least a month (it is likely it would be longer) and opioid withdrawal symptoms on codeine cessation (see Box 2). If the patient has not experienced opioid withdrawal symptoms on cessation then it is appropriate, before a medication-assisted taper is considered, to educate them about withdrawal symptoms and ask them to try ceasing codeine and record daily symptoms in a symptom diary.
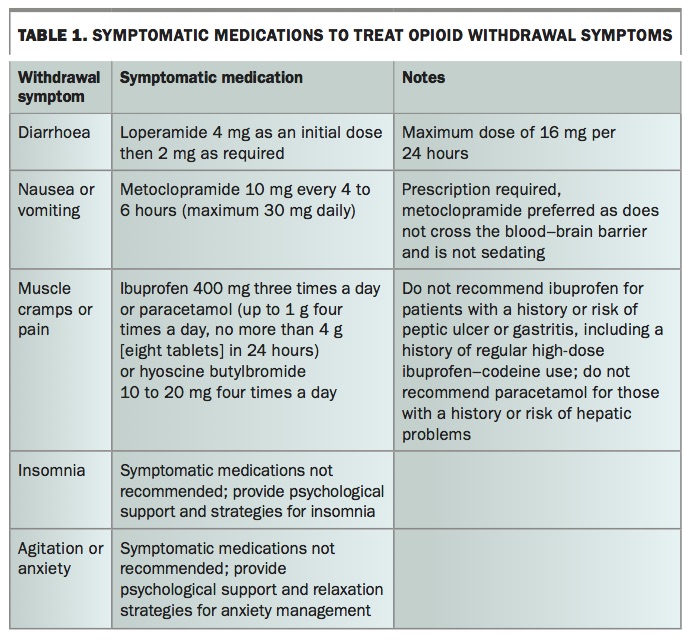
Symptomatic medications (nonopioid medications that reduce the symptoms of opioid withdrawal) can be used by patients who wish to self-manage codeine cessation without an opioid being prescribed. Examples are listed in Table 1. Patients should be advised that these medications can reduce the discomfort but may not entirely relieve opioid withdrawal symptoms.
{kind=link}
Medication options for managing codeine withdrawal symptoms
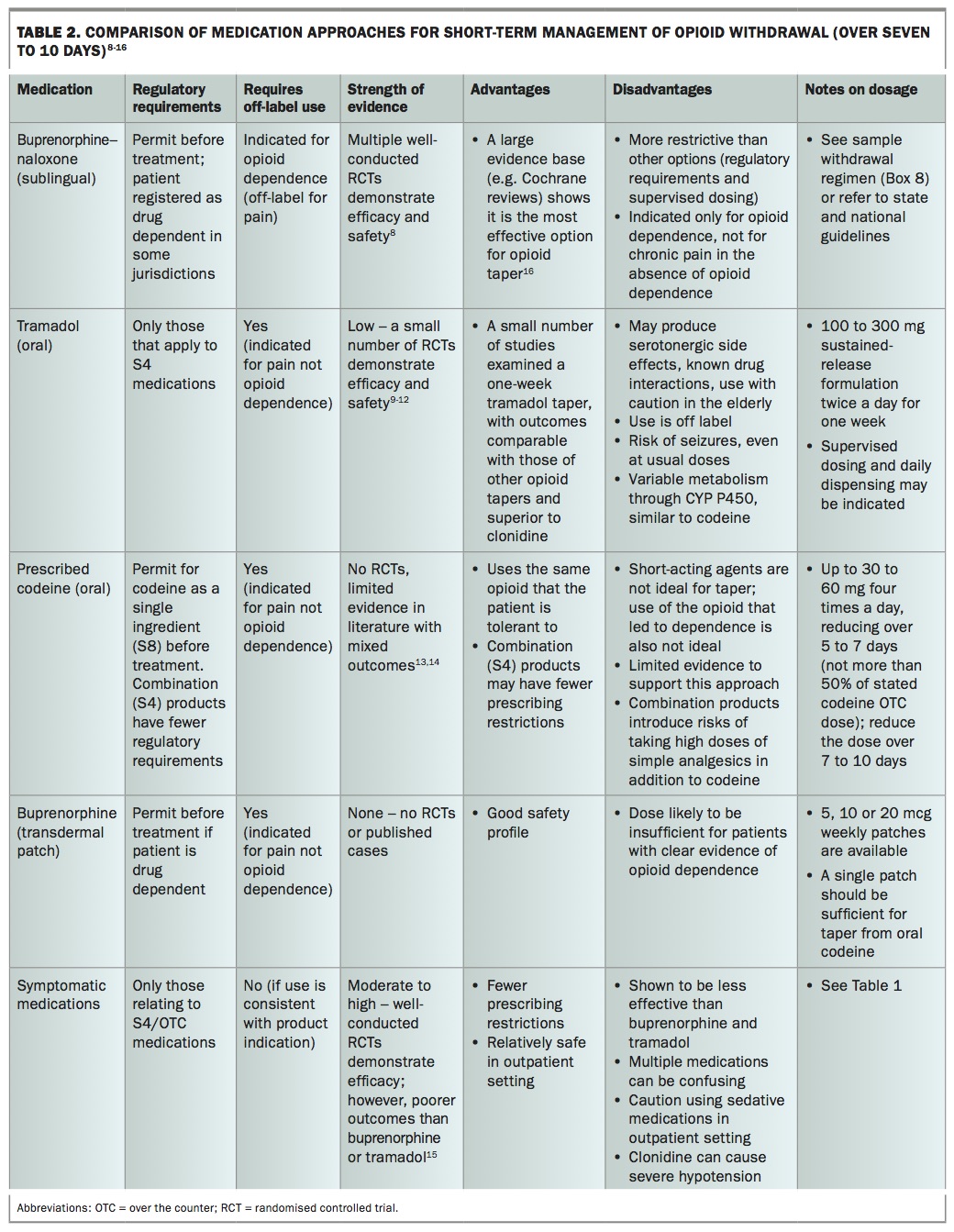
A range of medications have been proposed to help manage the temporary discomfort caused by codeine cessation, including the nonopioid symptomatic medications described above and opioids. These medications and their regulatory requirements, supporting evidence, advantages and disadvantages are summarised in Table 2.8-16 This use is off-label for most; many have limited supporting evidence and not all can be recommended.
{kind=link}
The largest body of evidence supports the use of sublingual buprenorphine (provided as buprenorphine–naloxone), followed by symptomatic medications. The latter nonopioid medications are an alternative that may be appropriate for patients with lower-level opioid neuroadaptation and are discussed above. Prescribed codeine, tramadol and buprenorphine patches have also been proposed to treat opioid withdrawal but their use is off label for this purpose and they have a limited evidence base. Tramadol and buprenorphine patches are indicated only to treat pain.
If opioid withdrawal symptoms are not relieved by buprenorphine or symptomatic medications then this may indicate a higher level of dependence. Where the treating doctor does not possess relevant training and experience, these patients may require referral for management by an addiction medicine specialist in an inpatient or outpatient setting. Maintenance treatment with opioid agonists (buprenorphine–naloxone or methadone) should be considered for these patients.
Prescribing of opioids for the management of codeine withdrawal should be limited to a maximum of seven to 10 days. If longer periods of medication are required then these should be provided in the context of medication-assisted treatment for opioid dependence (buprenorphine–naloxone or methadone) in accordance with national and jurisdictional guidelines.5 There is little evidence to support the use of medications other than methadone and buprenorphine–naloxone, and for this reason these other approaches are not recommended. It is strongly recommended not to transfer patients to strong opioids such as oxycodone, oxycodone–naloxone or fentanyl.
Patients should be in contact with an experienced healthcare professional while undergoing opioid withdrawal, and this contact should be at least daily during the first few days to allow clinical review and dose adjustment. Because of interpatient variability in the opioid effects of codeine, the risk of either undertreatment or oversedation should be considered. Review of patients is recommended a few hours after the first dose of buprenorphine–naloxone. Patients should be warned that they may have difficulty fulfilling their usual roles during this time; they may need time off work or to make alternative child care arrangements and they may not be able to drive a car (depending on the strength of the medication prescribed and how it affects them). If necessary, opioid withdrawal can be conducted in a residential facility such as a drug and alcohol detoxification service.
Buprenorphine in management of codeine withdrawal
The largest body of evidence is for the use of buprenorphine in the clinical management of opioid withdrawal.16 The efficacy of buprenorphine is supported by a Cochrane review, and the most clinical experience exists for buprenorphine to treat codeine dependence.16,17
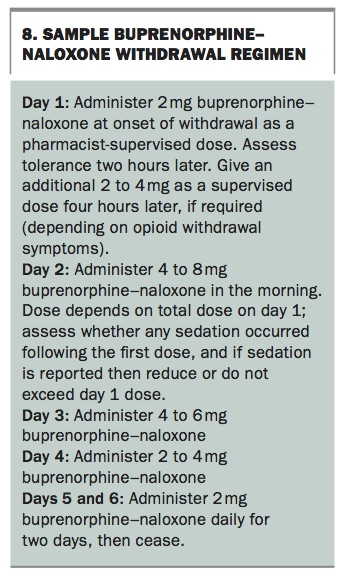
Buprenorphine is ideal for management of opioid withdrawal as it is a partial agonist with a ceiling on respiratory depressant effects and can be administered with once-daily supervised dosing.18 A sample buprenorphine–naloxone withdrawal regimen is shown in Box 8.
{kind=link}
When a patient commences buprenorphine, key considerations include avoiding ‘precipitated withdrawal’. This occurs when buprenorphine is administered while a full opioid agonist is still active in the body. Buprenorphine displaces the full opioid agonist at the mu-opioid receptor, leading to opioid withdrawal symptoms. To avoid precipitating opioid withdrawal, standard procedures outlined in guidelines include waiting until mild-to-moderate opioid withdrawal symptoms are observable, typically about 12 hours after the last dose of a short-acting opioid such as codeine. The Clinical Opioid Withdrawal Scale is a useful tool to assess opioid withdrawal (Box 9).19
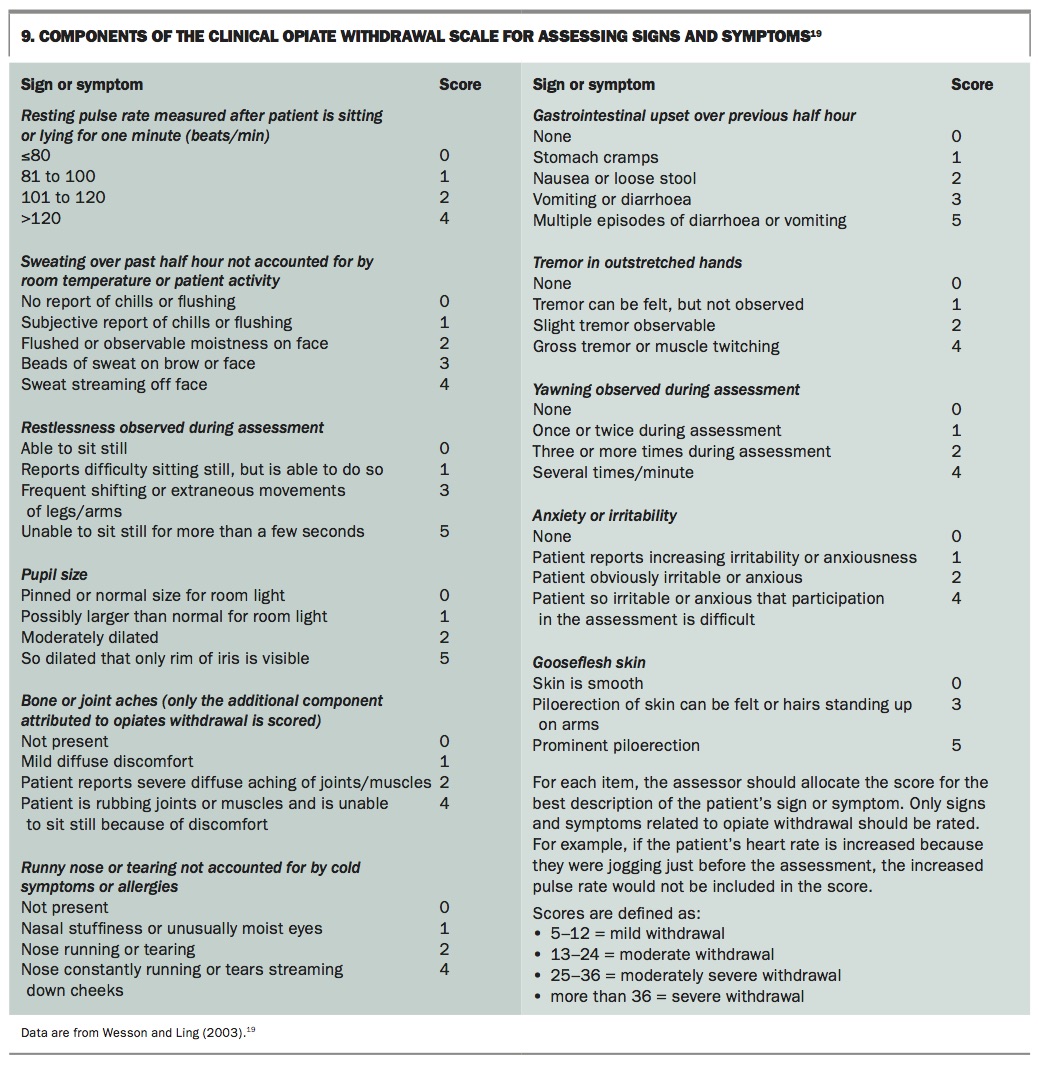{kind=link}
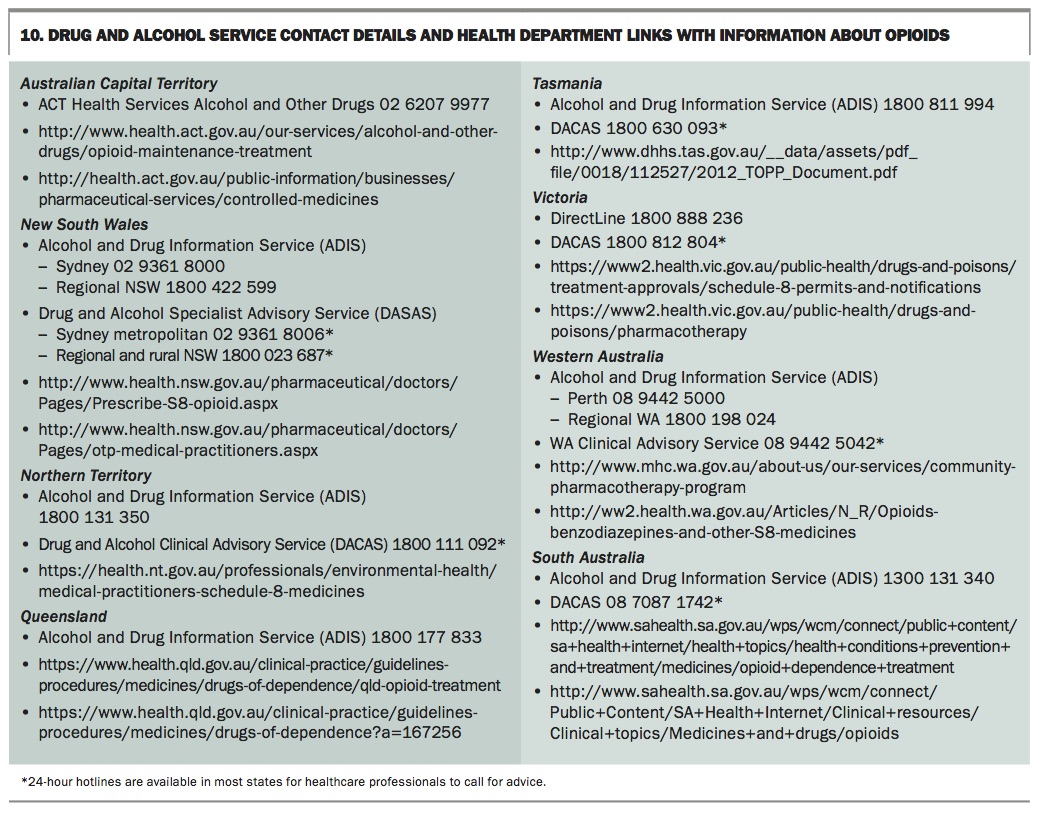
GPs unfamiliar with their local state and territory requirements on prescribing buprenorphine should contact their local health department or addiction specialists for advice and support (see Box 10 for contact details). Advice is also available from local drug and alcohol services, which in most states provide 24-hour telephone advice lines (Box 10). Before buprenorphine treatment begins, an authority is required from the state or territory health department. In states such as Victoria, South Australia and Western Australia, GPs can commence buprenorphine–naloxone treatment without being accredited prescribers or with minimal additional training. However, most other jurisdictions require doctors to undergo some training before being authorised to prescribe buprenorphine. Buprenorphine (usually as buprenorphine–naloxone) is dispensed only by specific pharmacies. The pharmacy should be contacted in advance to confirm that it can accept the patient.
{kind=link}
Longer-term treatment with buprenorphine–naloxone should be considered when there is a clear diagnosis of opioid dependence, including difficulty controlling use, continued codeine use despite harm, clear tolerance and withdrawal symptoms on cessation. For some people with codeine dependence, ongoing treatment with buprenorphine–naloxone or methadone has been lifesaving.
Conclusion
Over the next few months, as patients present to their GPs requesting codeine or reporting previous OTC codeine use, careful assessment may identify unmanaged tolerance or opioid dependence. The change in codeine availability may provide an opportunity for better management of chronic pain conditions. Depending on the pattern of codeine use, different management strategies may be appropriate. For most patients who report infrequent codeine use, alternative nonopioid analgesia will be appropriate. Where patterns of high-dose use are identified, medication-assisted treatment in consultation with drug and alcohol experts may be required. Where the level of opioid tolerance and dependence is unclear, supporting the patient to cease codeine in the short term is recommended in the first instance. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.