Migraine in 2022: an update on management

Migraine is a common and disabling neurological condition that affects quality of life. A personalised management approach addressing lifestyle factors and acute and preventive medications can improve the impact of disease and quality of life.
According to the Global Burden of Disease studies, migraine represents the second leading cause of disability worldwide and the leading cause of reversible disability in people under the age of 50 years.1,2 In Australia, migraine affects about one in five people and is among the 20 most common conditions managed by GPs, being responsible for one in 100 GP encounters.3 Unsurprisingly therefore, it is estimated to cost the economy AU$35.7 billion in direct health and indirect costs.4
Each year 2.5% of patients with migraine progress from episodic (less than 15 headache days per month) to chronic migraine (15 or more headache days per month), with associated negative impacts on quality of life and health resources.5 The key modifiable risk factors contributing to disability are obesity, snoring, stressful events, depression or anxiety and significantly ineffective preventive treatment. These risk factors increase severity or frequency of migraine, leading to increased attack frequency and acute analgesic overuse.5 This article outlines the diagnosis and management of migraine, highlighting the importance of careful assessment for differential diagnoses and an approach to management that includes lifestyle interventions and pharmacological treatment.
Pathophysiology
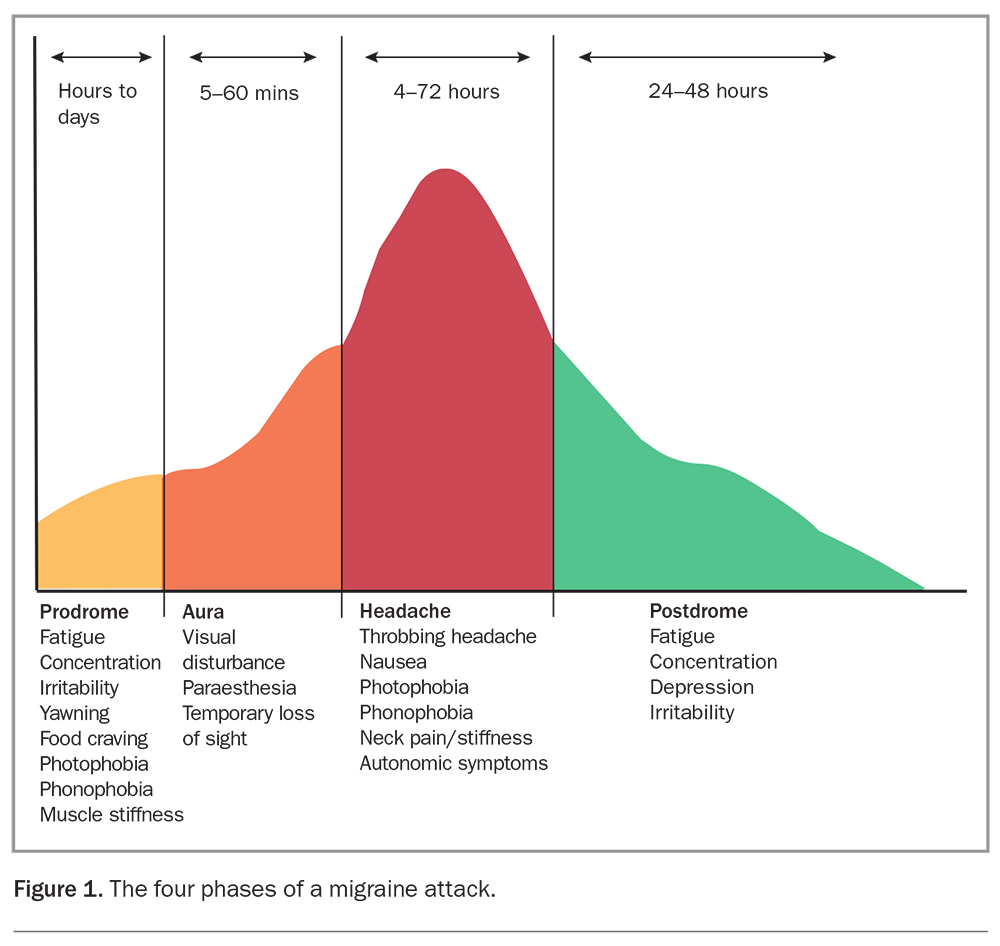
The 20th century vascular theory of migraine is now recognised to be incomplete, and while the pathophysiology of migraine is complex and reviewed elsewhere, several key points bear highlighting.6,7 Although the trigger is still debated, imaging studies show several brain regions, including the hypothalamus, are activated 24 to 72 hours before a migraine attack.8 These studies provide a pathophysiological correlation for the four clinical phases of a migraine attack, which are prodrome, migraine aura, headache and postdrome (Figure 1).6,9
{kind=link}
A migraine aura is believed to be caused by a spreading ‘wave’ of depolarisation and subsequent refractory period across a cortical region.10 The pain of a migraine attack itself is caused by activation of the trigeminocervical complex in the brainstem, along with other pain circuits, and subsequent release of a variety of neuropeptides including calcitonin gene-related peptide (CGRP).6,7 CGRP, which has emerged as a therapeutic target, acts on the trigeminovascular system, a complex system rich in CGRP and 5HT receptors that, as a potent vasodilator, causes the vascular changes originally observed in migraine.11
Presentation and assessment
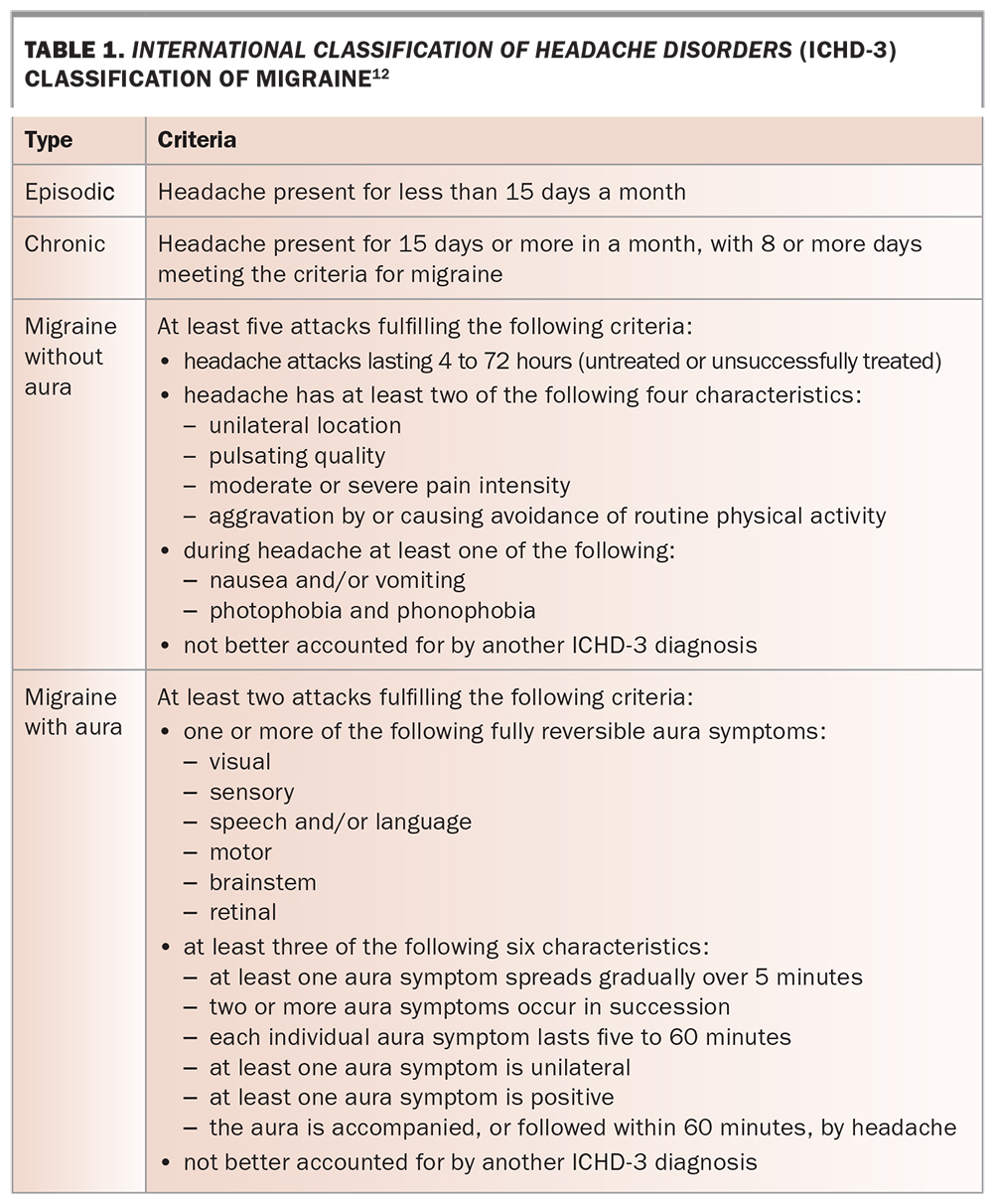
Migraine is defined by the International Classification of Headache Disorders, third edition (ICHD-3) and further classified by frequency as either episodic or chronic and by the presence or absence of aura (Table 1).12 The four phases of a migraine are described above. The headache phase is easily identified by the presence of pain; however, careful questioning can often identify features of a prodromal phase, which can provide greater certainty for the clinician, as well as understanding for the patient. For example, symptoms such as neck stiffness and food cravings can occur during the prodromal phase and, if patients are unaware of this, they may mistakenly attribute their migraine attack to foods consumed due to prodromal cravings.
{kind=link}
Migraine aura is reported in 30% of patients, and does not necessarily precede each headache. Over 95% of patients with aura experience a visual phenomenon, often a scintillating scotoma that may start centrally, often with jagged edges (fortification spectra) (Figures 2a and b).13,14 Other manifestations may be sensory, motor, speech or, rarely, brainstem symptoms. Aura causes fully reversible, typically unilateral symptoms. Certain features help to distinguish it from important differential diagnoses. Migraine aura develops gradually, evolving over 10 to 30 minutes, lasting 5 to 60 minutes and often consisting of positive symptoms (paraesthesia) followed by negative symptoms (numbness). Transient ischaemic attack, by contrast, begins suddenly, persists for minutes to hours, generally as negative symptoms, and only affects cranial vascular territories. Focal seizures also progress gradually (such as with a Jacksonian march), but are of shorter duration, lasting less than two minutes.15
{kind=link}
The pain phase of a migraine attack is often unilateral at onset, however, is generally not side-locked.16 It may occur on either side and become generalised with a gradual worsening and throbbing character that lasts from four to 72 hours.12 Features that differentiate migraine pain from other headaches include worsening with physical activity and the migrainous phenomena of nausea, or photophobia and phonophobia,12 thus generating the prototypic description of a person who avoids activity and lies down in a dark room because of their symptoms. Finally, a postdrome may be identified and include symptoms of fatigue, depression, irritability and reduced concentration (Figure 1).
Diagnosis
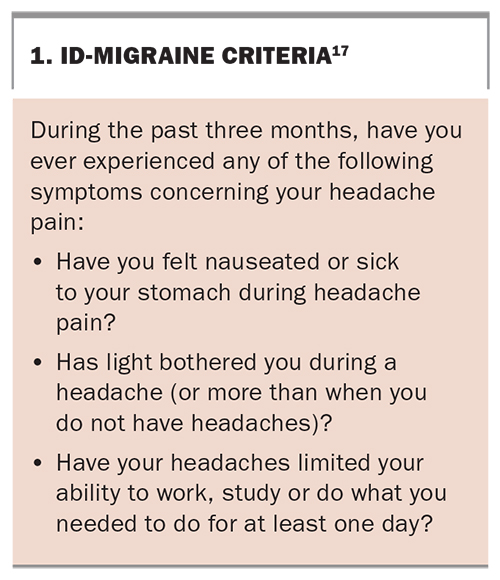
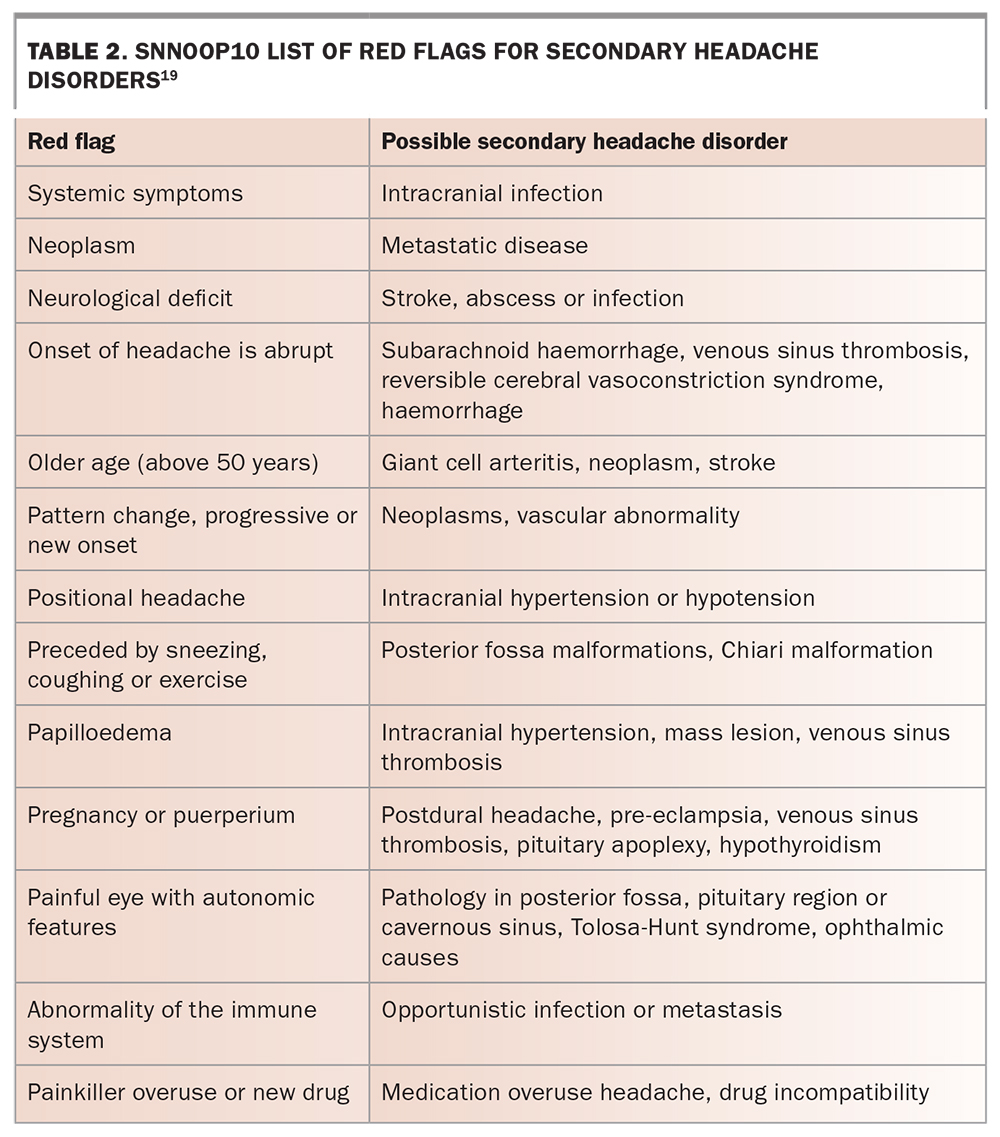
Migraine is a clinical diagnosis and further investigation should only be considered in the appropriate clinical context.17 The ID-Migraine questionnaire is a useful screening tool to help identify patients with migraine in primary care (Box 1) and should be performed alongside screening for red flags for secondary headaches using the SNNOOP10 flags for secondary headaches criteria (Table 2).18,19
{kind=link}
{kind=link}
Hypothyroidism and vitamin D and iron deficiency may be associated with increased headache frequency and should be identified and treated.20-22 Because incidental findings, found in 2% of the general population, may increase distress and provoke further unproductive investigation, routine neuroimaging is not recommended for patients with a normal neurological examination and no atypical headache features or red flags.23,24 Specific consideration should be given to important mimics that may be differentiated on history and include the following.25
- Cluster headache – this presents with excruciating, strictly side-locked pain over the temple and orbital region, with accompanying agitation and cranial autonomic features (e.g. tearing, nasal congestion).26 Differentiated from migraine by its side-locked pain and agitation, cluster headaches are typically shorter (averaging 90 minutes) and typically exhibit circadian (classically one to two hours after sleep onset) and circannual periodicity (bouts occur at the same time of year, typically in autumn and spring).
- Hemicrania continua – presents with strictly side-locked pain that is continuous from onset.12 Differentiated from migraine by its side-locked and continuous nature, it may also present with agitation and autonomic symptoms.
- New daily persistent headache – differentiated from migraine by its unremitting (persistent) nature and clearly remembered day of onset.
- Tension-type headache – described as a featureless headache, it is distinguished from migraine by shorter and less disabling attacks with an absence of migrainous features (i.e. throbbing pain, nausea, photophobia or phonophobia).12
- Sinus headache – although often diagnosed from imaging findings or frontal tenderness, headache due to chronic sinusitis is relatively rare. In one formative study, 81% of patients with the label actually had migraine and management was delayed by an average of 7.8 years.27
Approach to management
The management of migraine can be broken into three pillars: lifestyle management, acute treatment and preventive treatment. All patients benefit from lifestyle management and optimisation of acute treatment, while patients with four or more migraine days a month or attacks that are difficult to control may benefit from preventive treatment.
Lifestyle management
Lifestyle management is likely an effective treatment that affords patients autonomy over their health. Studies on lifestyle interventions in managing migraine are limited; however, some suggest engaging in regular positive lifestyle behaviours may help limit episodes of chronic migraine, with a number needed to treat (NNT) of just two in a population of people with chronic migraine.28 The mnemonic SEEDS (sleep, exercise, eating, diary, stress) is a useful framework for framing a discussion around lifestyle management.29
Sleep
Although snoring is a risk factor for progression to chronic migraine, obstructive sleep apnoea (OSA) does not occur more frequently in patients with migraine.30,31 The presence of sleep-disordered breathing, early morning headaches or daytime somnolence should, however, prompt further investigation for OSA as a modifiable factor in people with migraine. A bidirectional relationship may exist between migraine and insomnia, with a further association with frequency and severity of migraine attacks.32
Strategies to improve sleep quality include sleep restriction, improved sleep hygiene and stimulus control. Cognitive behavioural therapy (CBT) for insomnia has also been shown to improve headache frequency.33 The Sleep Health Foundation has detailed resources that are of benefit (https://www.sleephealthfoundation.org.au).
Exercise
A recent meta-analysis of 265 studies found that aerobic exercise of 30 to 50 minutes, three to five times a week over six weeks has a modest effect on the frequency of migraine attacks.34 Exercise was also shown to be noninferior to pharmacotherapy and patients saw an additive benefit of therapies.29 A graded exercise program is important for improving tolerability in patients with migraine.
Eating (diet)
Dietary triggers of migraine are reported by up to one third of patients, with 44%, 27% and 7.5% reporting migraines triggered by fasting, alcohol consumption and chocolate consumption, respectively.35,36 However, the role of specific dietary triggers should be interpreted carefully as the hypothalamic activation and food craving that often precede an attack can be mistaken for triggers.6,8,35 For example, one double-blind study showed that chocolate did not trigger migraines.37
Dietary advice should be practical and focus on avoiding general triggers, such as fasting, and making dietary choices to maintain even blood glucose levels.38,39 Although the role of caffeine in migraine is not fully understood, abrupt withdrawal from caffeine can potentiate headaches, with a dose-dependent relationship between cessation and withdrawal symptoms.40 A gradual reduction to the minimum tolerable level or a maximum of 200 mg of caffeine per day (two cups of coffee) is a reasonable approach.41 Several dietary interventions show improvement in headache frequency, including low-fat, low glycaemic and Mediterranean diets, and may be recommended to patients.3
Diary
Keeping a headache diary is recommended to help monitor disease activity, effectiveness of preventive treatment and frequency of analgesic use. Headache diary templates are available on the Australian and New Zealand Headache Society website (https://anzheadachesociety.org/for-patients). Electronic versions are available for smart devices.
Stress
The causal relationship between stress and migraine remains unclear; however, periods of stress are associated with both new-onset migraine and transformation to chronic migraine, and change in levels of stress (both increased and decreased) are a risk factor for a migraine attack.42 Accordingly, stress-centred interventions for managing migraine, such as relaxation therapy, CBT and biofeedback, are supported by grade A evidence.43
Acute treatments
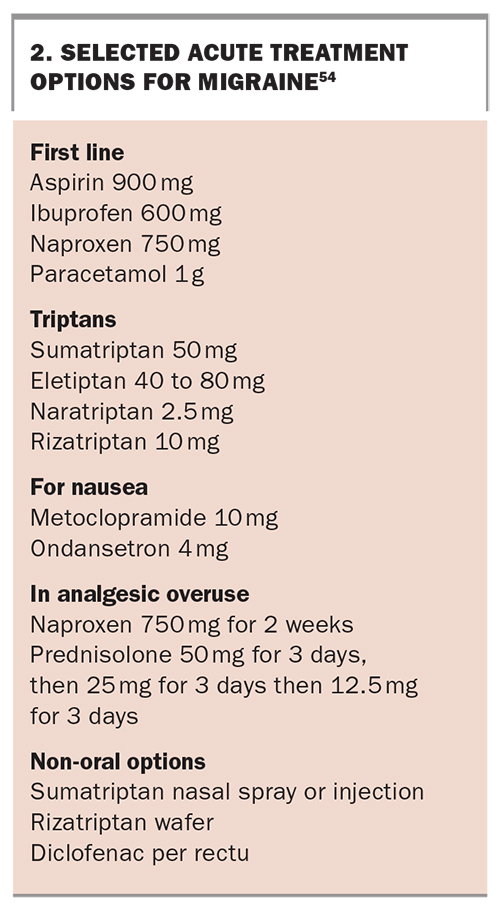
The goal of the acute treatment of migraine is pain freedom within two hours. This may be achieved through monotherapy with simple analgesia or, if analgesia alone is ineffective, by the addition of a triptan or an antiemetic (Box 2). Some key principles to enhance efficacy include:
{kind=link}
- analgesics are more effective when taken early during an attack44
- a combination of analgesics is more effective than monotherapy44
- beyond the antiemetic effect, metoclopramide provides additional analgesic effect and improves the response to other analgesics.45,46
In patients without a significant vascular history, triptans are an effective treatment. Studies have shown they achieved pain freedom as monotherapy in 18 to 50% of cases.47 Initial triptan selection is often based on route of administration – rizatriptan and sumatriptan are available as nonoral preparations for patients with prominent early nausea. In patients who do not have initial pain relief with other triptans, rotation to eletriptan 80 mg or rizatriptan 10 mg may be more effective.48 In patients in whom analgesia has a waning effect, longer acting analgesics such as naratriptan or naproxen may be preferable. Nonpharmacological interventions, such as meditation and ice-packs, have also shown effect.49,50
Overuse of acute medications
Overuse of acute analgesia for any reason predisposes patients with migraine to developing a secondary headache, medication overuse headache (MOH).12 MOH occurs as a result of further sensitisation of the pain circuits of the brain, and diminished ability to inhibit painful signals, resulting in headaches that are more frequent and refractory to both acute and preventive treatments.51 Unfortunately, up to 70% of patients with chronic daily headaches suffer comorbid MOH.52
Prevention is the best treatment for MOH, and patients must be counselled to not exceed 10 days of triptan use per month, or 15 days total for simple analgesics.12 Opiates are not recommended for migraine by the authors because of potential issues of both MOH and dependence. Few studies exist for MOH management; however, in conjunction with preventive treatments, bridging strategies, including use of slow-release naproxen (for triptan overuse) or prednisolone and withdrawal (although evidence for this is limited and mixed), are recommended (Box 2).25,53,54
Preventive treatments
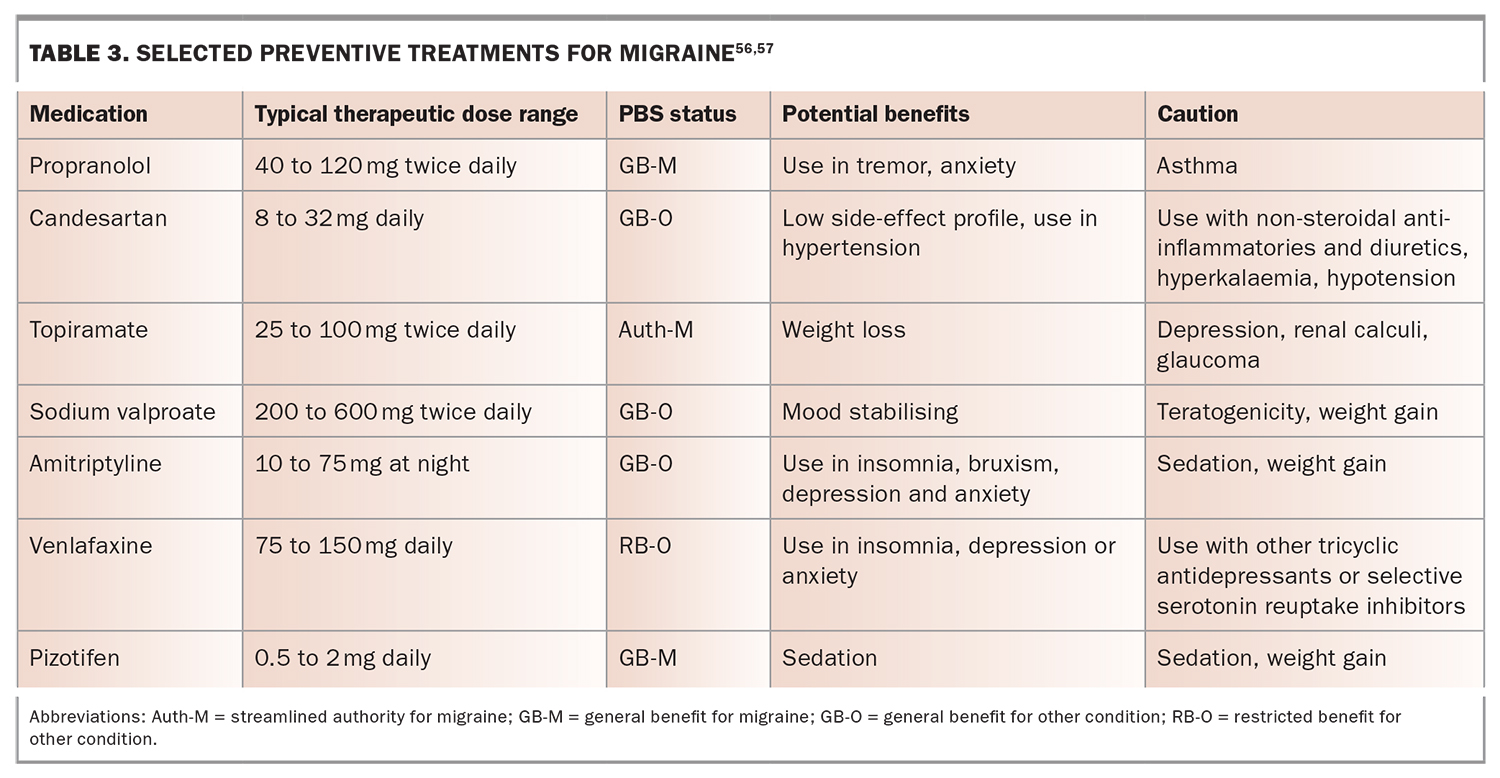
Preventive treatment for migraine is indicated to limit the impact of migraine and risk of acute analgesic overuse for patients who have more than four days of migraine per month or those with disabling disease.55 Selected oral medications are outlined in Table 3.56,57 Although evidence based, several preventive treatments for migraine are available for off-label use on the PBS. Guiding principles for the use of oral preventive treatments for migraine include:
{kind=link}
- given no preventive oral medication is clearly superior, the choice of medication is best guided by side-effect profile, comorbidity and patient preference
- in the absence of side effects, medications should be continued for a minimum of eight to 12 weeks at a moderate dose to assess efficacy
- in the absence of side effects, the dose should be titrated to assess efficacy and optimise response.
Some patients may prefer supplements for migraine prevention; however, evidence for their efficacy is limited and mixed. Some studies suggest magnesium, riboflavin, coenzyme Q10 and cholecalciferol are effective and safe for migraine prevention.21,58 Vitamin D deficiency has been shown and mitochondrial energy depletion suggested in people with migraines.21,59 Evidence suggests the following supplemental treatment may be considered for suitable patients:
- 400 to 600 mg of magnesium (elemental) daily60
- 200 mg of riboflavin daily54
- 150 to 300 mg of coenzyme Q10 daily54
- replacement of vitamin D to normal levels.61
Advanced treatment options are available for patients with chronic migraine in whom three preventive medications have not been effective or are contraindicated and any comorbid MOH has been addressed. Treatments include onabotulinumtoxin A (OnaB-A) and the CGRP monoclonal antibodies (mAbs) fremanezumab and galcanezumab. OnaB-A and CGRP mAbs must be started by a neurologist; however, CGRP mAbs may also be prescribed by GPs for continuing treatment in shared care with a neurologist. OnaB-A is given as a series of 31 subcutaneous injections through the head and neck at 12-weekly intervals and may be particularly useful for patients with neck-muscle activation, bruxism or multiple comorbidities owing to its limited systemic uptake. CGRP mAbs are given as a single subcutaneous injection to the stomach or thighs. The PBS requires a patient to show a 50% or greater improvement in headache frequency to continue the treatment, assessed at six months for OnaB-A and three months for CGRP mAbs.
Although there are no high-quality data assessing the relative efficacy of these two treatments, both have shown efficacy in treating headaches in clinical trials. OnaB-A achieved a 50% or greater improvement in headaches in 47.1% of patients.62 CGRP mAbs showed a 50% or greater reduction in headaches in 30 to 40% of patients.63 These medications are very well tolerated, with reported side effects of constipation, injection site reactions and nasopharyngitis in about 5% of patients. Given the potential for off-target effects of inhibition, individualised decision-making is important, particularly for patients with cardiovascular or significant autoimmune disease, or upcoming planned surgery.63,64
Conclusion
Migraine is a common presentation in clinical practice that requires a comprehensive approach to management. Important differential diagnoses should be assessed in the context of the four clinical phases of migraine. Addressing lifestyle factors that may contribute to migraine can help reduce migraine frequency and morbidity. Pharmacological treatments include acute and preventive medications and should be used appropriately to optimise response and reduce acute analgesic overuse. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.