Osteoporosis: a hidden burden in men

Osteoporosis
Men's health
Almost one-third of all minimal trauma fractures occur in men, but men remain less likely than women to be investigated or treated for osteoporosis. GPs are well placed to identify, diagnose and treat men at increased risk of osteoporotic fracture, thereby narrowing the gap in care for patients with this condition.
- Almost one-third of all osteoporotic fractures occur in men.
- Compared with women, men have a higher risk of refracture, morbidity and mortality after a minimal trauma fracture.
- Men are less likely than women to undergo investigation and treatment for osteoporosis.
- Bisphosphonates, denosumab and teriparatide are safe and effective medications to treat osteoporosis in men.
- Men with any one of the following risk factors should be assessed for osteoporosis: age 70 years or older, previous minimal trauma fracture, receiving androgen deprivation therapy or long-term glucocorticoid exposure.
Osteoporosis is a musculoskeletal disease characterised by low bone mass and microarchitectural deterioration in bone that predisposes to minimal trauma fractures (MTFs). Although osteoporosis is often misconceived as a disease affecting women only, it is also a major public health problem in men that contributes to significant morbidity, mortality and healthcare costs. The magnitude of this problem is expected to increase with the ageing Australian population.
Burden of osteoporosis in men
After the age of 60 years, about 25% of men and 44% of women will sustain an osteoporotic fracture during their remaining lifetime.1 About 30% of all MTFs occur in men.2 In 2013, there were 43,275 MTFs in Australian men (one fracture every 12 minutes), with a projected 55,316 fractures in 2022 (one fracture every 9.5 minutes).2
Although the lifetime risk of hip fracture is lower for men than for women, men who sustain a hip fracture have a mortality rate two to three times higher than that in women.3 Men are also at significantly higher risk of refracture compared with women.2 In 2012, the total costs associated with all osteoporotic fractures in Australian men over 50 years of age amounted to $525 million.2 Despite its clear impact on health outcomes and healthcare costs, men are less likely to be investigated or treated for osteoporosis.4,5 In one study that followed men and women admitted to hospital with an MTF, only 10% of men were receiving appropriate osteoporosis treatment 12 months after the fracture, compared with 48% of women.5
Pathogenesis
Osteoporosis in men can be the result of a multitude of factors, including genetics, declines in testosterone levels that accompany an increase in comorbidities with age, physical inactivity and traditional risk factors for bone loss, such as vitamin D deficiency, low calcium intake and glucocorticoid therapy.
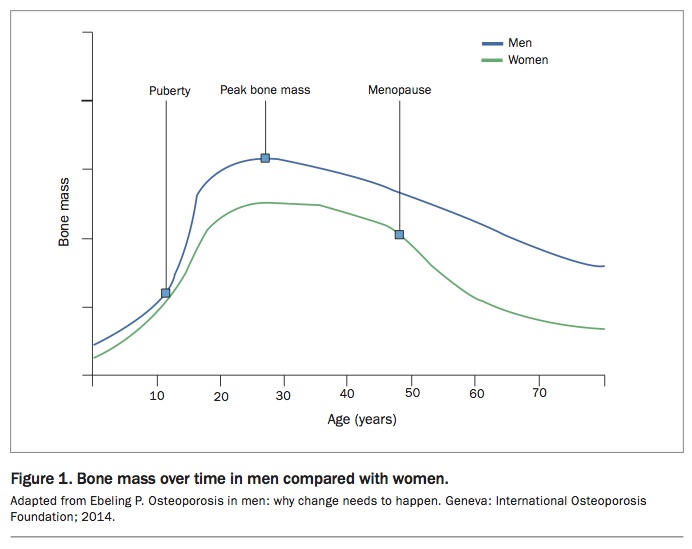
Bone mineral density (BMD) is similar in both sexes in early life and increases rapidly in puberty. Men start puberty later than women but have a longer bone maturation period and later epiphyseal fusion (Figure 1). Androgens increase periosteal bone apposition, increasing the cross-sectional diameter of bone and leading to the development of larger skeletons.6 By the end of puberty, men are less prone to fracture because they have higher peak bone mass, larger bone size and greater bone strength than women.7 Low oestradiol levels in older men are associated with a higher risk of fracture. Maintenance of cortical and trabecular BMD in older men is associated with higher levels of bioavailable oestradiol.8
{kind=link}
As men and women age, bone resorption exceeds formation, leading to bone loss. Bone mass starts to decline gradually in men from the age of 30 years (about 0.5 to 1% annually), without the abrupt decline seen in women at menopause. Microarchitectural deterioration with advancing age is an important feature of osteoporosis. Bone loss in men occurs in the form of trabecular thinning, whereas there is a loss of trabeculae in women.9
Causes and risk factors
Osteoporosis can be classified as either primary (age-related or idiopathic) or secondary (the result of hypogonadism, chronic diseases, drug therapy or adverse lifestyle practices that increase bone loss). In secondary osteoporosis, trabecular bone is often affected more than cortical bone, which manifests as vertebral fractures.10
Age-related osteoporosis tends to occur in men over the age of 70 years. Both trabecular and cortical bone are affected, predisposing to fractures of the proximal femur, vertebrae and radii.11 It is thought to arise from a combination of decreased calcium absorption, reduced activation of vitamin D, a decline in the lifespan and function of osteoblasts, and decreased concentrations of sex hormones and insulin-like growth factor 1.
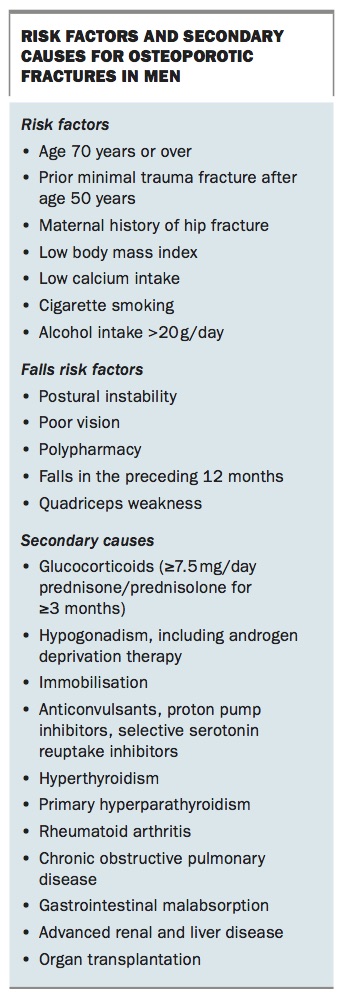
Secondary causes of osteoporosis are more often present in men than women and include glucocorticoid use, excess alcohol intake and androgen deprivation therapy (Box). Glucocorticoid-induced osteoporosis is associated with an increased risk of fracture as early as three months after initiation of glucocorticoids, so it should be recognised and treated promptly. Additional risk factors for osteoporotic fractures are listed in the Box.
{kind=link}
The major determinants of absolute fracture risk are increasing age, BMD, falls and previous osteoporotic fracture. BMD alone does not always reliably predict risk, and other risk factors should therefore be considered. Absolute fracture risk can be estimated using validated risk prediction tools, such as the Garvan Fracture Risk Calculator (www.garvan.org.au/bone-fracture-risk) or the Fracture Risk Assessment Tool (www.shef.ac.uk/FRAX). These can be used as patient education tools or to assess fracture risk if there is uncertainty about whether treatment is warranted.
Initial clinical assessment
The clinical assessment of osteoporosis begins with a detailed history, thorough clinical examination and investigations to confirm the diagnosis, assess severity and guide treatment, based on an individual’s absolute fracture risk.
History
The history should focus on risk assessment, eliciting any history of MTFs after the age of 50 years. Height loss of more than 2.5 cm may indicate previous vertebral fractures. Enquiries to assess potential secondary causes of osteoporosis should include any history of long-term glucocorticoid exposure, androgen deprivation therapy, thyrotoxicosis, malabsorptive disorders, myeloma, chronic kidney disease, hyperparathyroidism or inflammatory arthropathy. Specific symptoms of hypogonadism, such as loss of libido and reduced shaving frequency, should be elicited.
Maternal hip fracture is a nonmodifiable risk factor that increases absolute fracture risk. Modifiable risk factors include smoking, alcohol intake, physical inactivity, low dietary calcium intake and vitamin D deficiency, which should be addressed as part of the management strategy. Falls risk should be assessed, taking into account the number of falls over the past 12 months. The Falls Risk Assessment Tool is an example of a screening tool validated for use in elderly patients in residential care.12
Clinical examination
A focused clinical examination of a man being assessed for osteoporosis should include measurement of height and weight and calculation of body mass index. Thoracic kyphosis, focal vertebral tenderness and loss of height may raise suspicion of vertebral fractures. Evaluation for features of thyrotoxicosis, Cushing’s syndrome and hypogonadism should be undertaken. Features of hypogonadism include sparse facial, body and pubic hair, gynaecomastia and reduced testicular volumes (normal range, 15 to 25 mL).
Investigations
BMD measurement with dual-energy x-ray absorptiometry is a useful adjunct to history taking and examination in quantifying fracture risk and monitoring treatment response. A baseline measurement should be obtained, even for patients in whom treatment is clearly indicated based on clinical assessment. A thoracolumbar spine x-ray is useful to detect prevalent vertebral fractures (Figure 2), which are often asymptomatic. The presence of vertebral fractures indicates a high risk of future fractures and is thus important in the initial assessment of fracture risk.
{kind=link}
Suggested laboratory tests for men with osteoporosis include:
- renal function
- serum calcium, phosphate and thyroid stimulating hormone levels
- serum electrophoresis and immunofixation
- serum free light chain analysis
- coeliac serology
- measurement of 25-hydroxyvitamin D level.
Additional testing for other secondary causes of osteoporosis may be indicated based on individual clinical assessment. The Endocrine Society of Australia guidelines recommend against the routine measurement of sex steroid hormones in men with osteoporosis, unless indicated after careful clinical assessment.13
Treatment of osteoporosis in men
General measures
Men should be advised about lifestyle measures that optimise bone health. A balanced diet with adequate calcium intake, safe sunlight exposure and regular weight-bearing physical activity, where appropriate, are recommended. Smoking cessation and moderation of alcohol intake should also be encouraged.
The recommended dietary intake of calcium is 1000 mg daily for men from 50 to 70 years of age and 1300 mg daily for men older than 70 years.14 Calcium supplementation (500 to 1000 mg of elemental calcium) may be necessary if dietary intake is inadequate.
Sunlight exposure is required for synthesis of vitamin D. In Australia, the general recommendation for people with moderately fair skin is five to 10 minutes of sunlight exposure (either before 10 am or after 3 pm each day) to 15% of the body surface area on most days during summer months.14 Longer periods of sunlight exposure are required in winter months, for people living in lower latitudes and for those with darker skin tones.14 The ability of skin to synthesise vitamin D diminishes with age. Vitamin D supplementation (cholecalciferol 1000 to 2000 IU daily) is often a safer and more practical means of overcoming mild- to-moderate deficiency. In those with severe vitamin D deficiency (25-hydroxyvitamin D level less than 20 nmol/L), higher doses of cholecalciferol (3000 to 5000 IU daily) can be given for 12 weeks before reducing to a lower maintenance dose, with the goal of maintaining a 25-hydroxyvitamin D level of more than 50 nmol/L.
Management of falls risk is multifactorial and may include (but is not limited to) periodic medication review (especially psychotropic and cardiovascular medications), referral to an exercise program that features strength and balance training, assessment of vision and occupational therapy home assessment.
Pharmacotherapy
Most clinical trials evaluating the antifracture efficacy of osteoporosis treatments have involved postmenopausal women. Similar trials in men have been scarce and most that have been conducted had major limitations, such as small cohorts, short study duration and use of surrogate outcome measures, such as change in BMD, rather than fracture outcomes. Regulatory authorities approved the available treatments for male osteoporosis on the assumption, primarily based on BMD outcome data, that antifracture efficacy was similar to that in women. Few studies in men have been sufficiently powered to detect differences in fracture outcomes.
Bisphosphonates
Bisphosphonates are structurally similar to pyrophosphate and inhibit osteoclast-mediated bone resorption. The oral bisphosphonates available in Australia are alendronate and risedronate, taken as daily or weekly preparations. Zoledronic acid is an intravenous bisphosphonate administered yearly.
Alendronate, using either 10 mg daily or 70 mg weekly dosages, has been shown in a meta-analysis of small randomised controlled trials involving 988 men to be effective at increasing BMD and reducing vertebral fractures.15 In a randomised controlled trial of 284 men with osteoporosis, risedronate 35 mg weekly significantly increased BMD after two years compared with placebo; this study and its open-label, two-year extension were not sufficiently powered to determine antifracture efficacy.16,17
A large randomised, placebo-controlled trial of 1199 men with osteoporosis evaluated the effect of annual intravenous zoledronic acid. After two years, men receiving zoledronic acid had a 67% relative risk reduction in incident vertebral fractures compared with placebo.18 The Health Outcomes and Reduced Incidence with Zoledronic Acid Once Yearly (HORIZON) Recurrent Fracture Trial was a randomised, placebo-controlled trial of 2127 men and women with recent hip fracture. Those randomly assigned to receive annual zoledronic acid showed 55% and 29% relative risk reductions in the incidence of new clinical vertebral and nonvertebral fractures, respectively, at two years, and a 28% reduction in the risk of all-cause mortality.19
Adverse gastrointestinal effects of oral bisphosphonates, such as reflux oesophagitis, may be minimised by correct administration. Patients should take the medication with a large glass of water. They should remain in an upright position and refrain from eating food and taking other medications for at least 30 minutes afterwards. One formulation of risedronate (Actonel EC; Teva Pharma Australia) can be administered with food; however, dairy products and calcium supplements should not be taken within two hours of risedronate.
The risk of medication-related osteonecrosis of the jaw (less than one to 10 per 10,000 patient-years) and atypical femoral fracture (3.2 to 50 per 10,000 patient-years) is relatively low. The risk of atypical femoral fracture may increase with longer duration of treatment. Intravenous zoledronic acid is associated with an acute phase reaction characterised by influenza-like symptoms in about 30% of patients after the first infusion.20
Discontinuation can be considered after five to 10 years, particularly among those at low absolute fracture risk. However, treatment should continue or resume in patients at high fracture risk, particularly those with hip or vertebral fractures or low BMD (T-score of –2.5 SD or less).14
Denosumab
Denosumab is a fully human monoclonal antibody that inhibits RANK ligand, thereby reducing osteoclast formation, maturation and function. Studies have shown similar BMD improvements in men and women treated with denosumab.21
It is administered as a subcutaneous injection (60 mg) every six months and is generally well tolerated. Hypocalcaemia may occur after treatment, especially in those with unrecognised vitamin D deficiency or chronic kidney disease.
After starting denosumab treatment, timely administration every six months is key, because discontinuation or delay in treatment has been associated with BMD loss, with a small proportion of patients potentially at increased risk of vertebral fractures.22
Teriparatide
Although sustained elevations in parathyroid hormone levels have deleterious effects on bone (as seen in primary hyperparathyroidism), parathyroid hormone administered in a pulsatile manner has anabolic effects on bone. Teriparatide is a parathyroid hormone analogue administered as a daily subcutaneous injection. In studies involving men, teriparatide significantly improved BMD, similar to rates seen in larger studies of postmenopausal women, in whom it has proven antifracture efficacy.23 Teriparatide is PBS subsidised for a maximum of 18 months for men with severe osteoporosis (BMD T-score of –3.0 SD or less) and previous osteoporotic fractures who have sustained a further fracture after at least 12 months of adequate antiresorptive therapy. It must be initiated by a specialist.
Hypogonadism and bone health in men
Male hypogonadism is an established risk factor for osteoporosis. Any patient with hypogonadism qualifies for an MBS-subsidised BMD test. Testosterone has important direct and indirect effects on bone health. However, in population studies of men with osteoporosis, there appears to be a stronger association between low oestradiol levels and fracture risk, independent of serum testosterone levels.24,25 Similarly, high levels of sex hormone-binding globulin appear to be more predictive than testosterone levels of bone loss and fracture risk in older men.25-27
Role of testosterone therapy in men with osteoporosis and hypogonadism
Serum testosterone levels normally decline with age and can be reduced in chronic disease states without necessarily reflecting abnormalities in the hypothalamic–pituitary–testicular axis.13 Although testosterone therapy in men with low serum testosterone levels and osteoporosis has been shown to improve lumbar spine BMD in various small-scale randomised controlled trials, there are no data to support its antifracture efficacy.28
Testosterone therapy may cause polycythaemia, elevation of prostate specific antigen levels and lower urinary tract symptoms and can exacerbate obstructive sleep apnoea. Some studies have reported a possible excess in cardiovascular events with testosterone therapy in men without hypogonadism.29 Thus, its use in men without pathological hypogonadism (i.e. hypogonadism secondary to diseases affecting the hypothalamus, pituitary gland or testes) is not recommended.13 Testosterone replacement therapy should be considered for all men with pathological hypogonadism regardless of age, provided there are no contraindications. Hypogonadal men receiving testosterone therapy who also have osteoporosis should still be treated with agents with proven antifracture efficacy (bisphosphonates, denosumab or teriparatide).
Androgen deprivation therapy and fracture prevention
Men being treated with androgen deprivation therapy or bilateral orchidectomy for prostate cancer are at increased risk of fracture. In a large observational study of 50,000 men with prostate cancer, the risk of fracture was up to 54% higher in men with iatrogenic hypogonadism.30 Australian guidelines recommend fracture risk assessment and BMD measurement for all men starting androgen deprivation therapy, as well as implementing general measures to protect bone health.14 Men with nonmetastatic prostate cancer treated with androgen deprivation therapy have been shown to benefit from denosumab and zoledronic acid, both of which improve BMD at the hip and lumbar spine, whereas denosumab has been shown to reduce the risk of vertebral fractures.31,32 In a large randomised controlled trial of 1468 men undergoing androgen deprivation therapy, the mean age of the men was 75 years, mean T-scores at baseline were –1.4 SD and –0.6 SD at the femoral neck and lumbar spine, respectively, and one-quarter of the men had a history of osteoporotic fracture. Treatment with denosumab significantly reduced the incidence of new vertebral fractures by 62% compared with placebo after three years of follow up.
National guidelines recommend that all men starting androgen deprivation therapy have baseline assessment of fracture risk and receive antiresorptive therapy if they have a history of MTF.14,33 In the absence of previous MTF, treatment for primary prevention should be considered in those with a baseline T-score of –2.0 SD or less or with a 10-year risk of major osteoporotic fracture exceeding 20%, although such treatment would not qualify for PBS subsidy.33
Conclusion
Although men contribute significantly to fracture burden, they are less likely to be investigated or treated for osteoporosis, despite the availability of safe and effective treatments for fracture prevention. GPs are well placed to identify, diagnose and treat men at increased fracture risk, particularly those who have sustained a previous MTF, who are receiving chronic glucocorticoid treatment or androgen deprivation therapy, or who are over the age of 70 years. In doing so, we can all contribute to narrowing the gap in osteoporosis care for men. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.