An 18-month-old girl with a severe blistering rash

Drug reactions
Skin conditions
Test your diagnostic skills in our regular dermatology quiz. What is the correct diagnosis?
Case presentation
{kind=link}
Two weeks ago, the girl was treated with a course of sulfamethoxazole/trimethoprim for a urinary tract infection. She had not received any antibiotics before.
While she is being observed in hospital, large areas of skin on her legs start to sheet off.
Differential diagnoses
Conditions to consider among the differential diagnoses for a child of this age include the following.
- Erythema multiforme major. This self-limiting hypersensitivity reaction may be considered for a patient with a history of a new medication. Erythema multiforme may also be a result of a viral infection, particularly herpes simplex. Mycoplasma infection is also commonly responsible. However, in many cases a triggering factor may not be identified. Erythema multiforme major is a severe skin and mucosal illness that is characterised by widespread blistering target lesions (Figure 2) and mucous membrane involvement. However, it is not a systemic disease.
- Acute generalised exanthematous pustulosis. This is a severe cutaneous adverse reaction to a drug. Acute generalised exanthematous pustulosis generally presents five to eight days after ingestion of the culprit drug with a characteristic rash that forms sheets of sterile pustules, rather than blisters, usually most prominent in flexural areas (Figure 3). The patient is usually febrile and very unwell. There is generally associated neutrophilia and in some cases organ involvement (hepatic, renal or pulmonary). Mucous membrane involvement is rare. Systemic involvement along with the rash is self-limiting.
- Immunobullous disease. Two immunobullous diseases affect children: IgA dermatosis of childhood and bullous pemphigoid. Both are very rare. The rash consists of thick-walled blisters scattered on any part of the skin surface. There may be mucosal involvement. These conditions affect only the skin and mucosa and patients usually remain well.
- Bullous impetigo and staphylococcal scalded skin syndrome. Some strains of Staphylococcus aureus are toxinogenic, and this manifests in two ways. The more common manifestation is bullous impetigo, which presents as multiple bullae on a background of normal skin. It is usually not generalised, but it may be a severe disease in neonates. Older children tend to remain well. The less common manifestation, staphylococcal scalded skin syndrome, affects children under 5 years of age, who present very unwell and febrile with generalised pain and cutaneous erythema on which thin-walled blisters form. There is often flexural and facial accentuation. Mucosal surfaces are not affected and, although children are miserable because of pain, they are not systemically unwell.
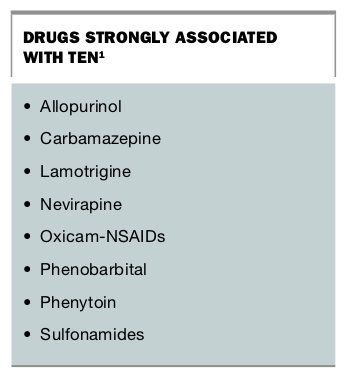
- Toxic epidermal necrolysis (TEN). This is the correct diagnosis. TEN is a drug-induced severe mucocutaneous reaction that should be considered in any patient who presents with a new rash after commencing an associated medication (Box).1 Full thickness necrosis of keratinocytes and sloughing of the skin and mucosal surfaces result in a life-threatening condition with an associated mortality rate of 30%.2 The main cause of death in TEN is due to severe sepsis. Apoptosis of the keratinocytes is believed to be an immune-mediated reaction to a medication or its metabolite. Initially, the patient will be generally unwell; the earliest lesions are atypical targets on the face, torso and proximal limbs. Vesicles or blisters appear in the lesional skin and can coalesce. This rash rapidly progresses over the entire body (Figure 4). Nikolsky’s sign is positive when epidermis is easily removed using gentle lateral pressure. All mucosal surfaces (eyes, mouth, genitalia and respiratory tract) can be affected by painful erosions and mucositis. Patients with TEN frequently have severe systemic disturbance, with multi-organ failure.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Management
This case emphasises the importance of taking a drug history in any patient presenting with a new rash. If there is a suspicion of TEN then any potential causative medications should be ceased immediately. Patients are best managed in an intensive care unit or special burns unit. Careful handling and wound care is paramount in the management of TEN due to the easily detachable epidermis and high risk of infection. Care must also be given to all the mucosal surfaces, and include regular assessment by ophthalmology, gynaecology and urology teams. Regular skin and line cultures should be performed and monitoring for infection is important. Guidelines around systemic therapy remain limited, due to the rarity of the disease and difficulty in conducting large randomised trials. Examples of the therapies used include high-dose corticosteroids, intravenous immunoglobulin, ciclosporin and, more recently, various tumour necrosis factor (TNF) alpha antagonists.3
Patients with TEN require long-term multidisciplinary follow up due to the multiple complications that may occur. These include ocular scarring, genitourinary adhesions and postinflammatory depigmentation. In some cases, there may be abnormal photosensitivity, abnormal sweating and pruritus. Patients should also wear a bangle with a drug warning once the culprit medication has been identified.
Outcome
The case patient was diagnosed with TEN and treated with an intravenous immunoglobulin infusion over two days. She remained intubated in the intensive care unit for five days, with the burns team supervising dressings. After three days new lesions stopped forming, and she was discharged from hospital after 14 days.
The patient continues to be reviewed by an ophthalmologist because of ocular irritation, but she has otherwise made a full recovery. The cause of the reaction was the antibiotic, and she now wears a MedicAlert bracelet. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.