Recognising androgen deficiency in adolescent boys

Endocrine diseases
Adolescent health
Parents who have concerns about their child’s growth and puberty will often seek advice from their GP. Many parents, however, are often not aware that their child’s pubertal progress is abnormal. A clear understanding of normal male pubertal milestones is essential for GPs to recognise when puberty is abnormal.
Case scenario
Daniel, aged 16 years, was accompanied by his father for a routine review of seasonal asthma with his GP. His father’s main concern was that Daniel seemed physically immature compared with his peers. Daniel was an otherwise healthy, prepubertal boy who was taking an inhaled corticosteroid as needed. Further history taking revealed that Daniel’s father had also been a late developer; he reported that he had been still growing while at university.
Pubertal changes in boys
Androgens are important for the development of secondary sexual characteristics during male puberty. These include development of masculine physique, facial and body hair, deepening of the voice, maturity of genitalia and spermatogenesis. Testosterone is the main androgen in males and is predominantly produced by the testes; dehydroepiandrosterone, androstenedione and dihydrotestosterone are also important.
In boys, pubertal changes typically occur between 9 and 14 years of age, with an average onset at 12 years. Puberty begins with activation of the hypothalamic-pituitary-gonadal axis as follicle stimulating hormone (FSH) and luteinising hormone (LH) stimulate Sertoli cells and Leydig cells, respectively, to stimulate spermatogenesis and testosterone production. Testicular enlargement is the first sign of puberty, followed by development of secondary sexual characteristics.
A normally timed puberty is both emotionally and physically important. About 40% of peak bone mass is attained in the two years before and after peak growth velocity, with pubertal delay restricting the ability to achieve maximal bone density.1 Delayed puberty is defined as the absence of secondary sexual characteristics by 14 years, the age when 95% of boys have commenced puberty.
Assessment
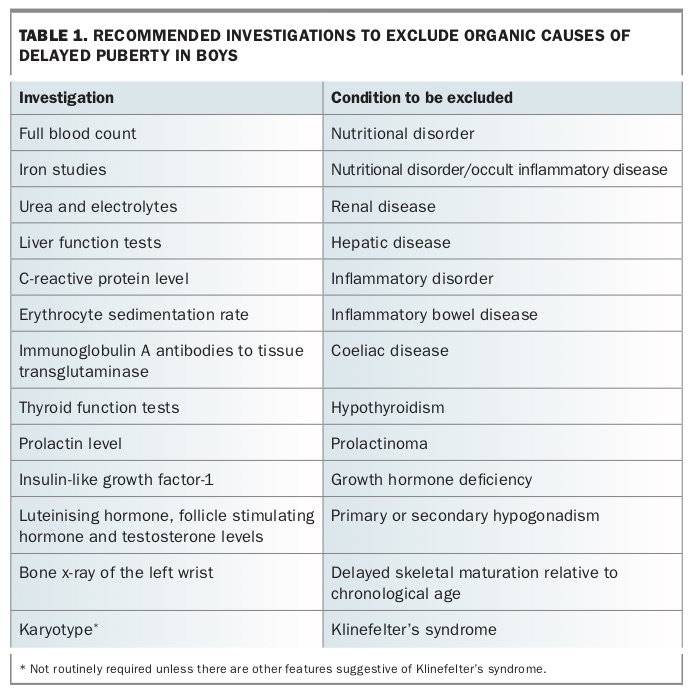
The objective of assessing delayed puberty is to differentiate pathological causes from constitutional delay, a normal variant. Assessment includes a thorough history and a systems review to exclude an underlying organic cause (Table 1) and effects of medications (e.g. steroids, stimulants). A family history of pubertal timing is essential.
{kind=link}
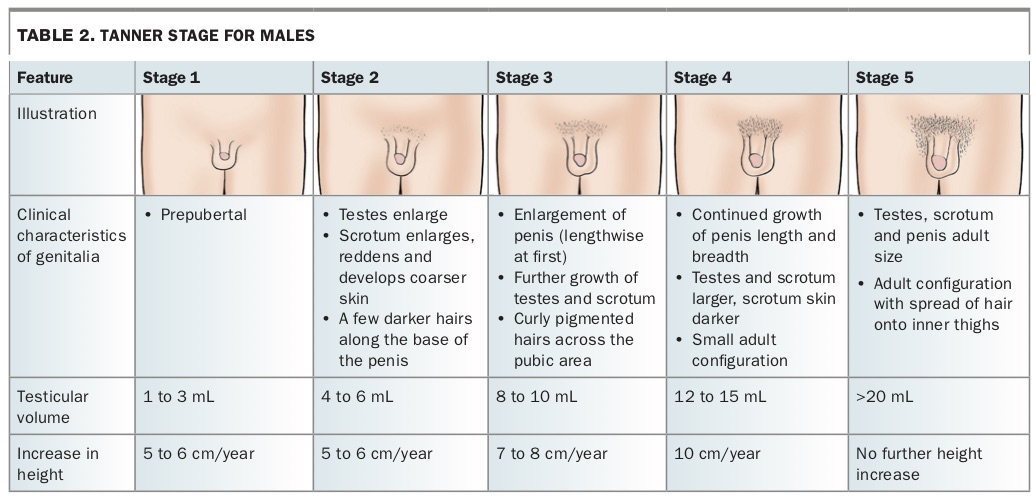
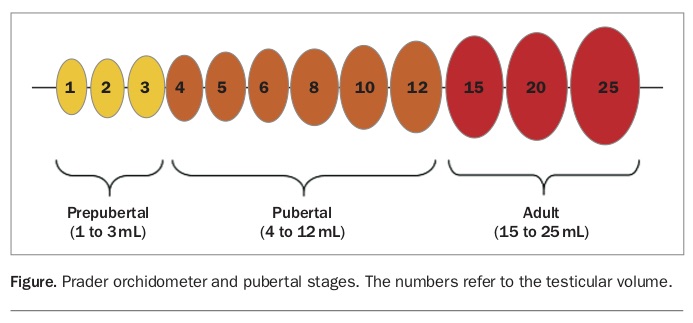
Serial height and weight measurements plotted on a growth chart are used to determine growth velocity. Pubertal assessment according to the five-stage classification by Tanner and Marshall (Table 2), including testicular measurement using a Prader orchidometer (Figure), is recommended to accurately determine puberty onset, stage and progression.2 Before puberty, normal growth velocity is at least 5 cm per year. At peak height velocity in males the 50th percentile is 9 to 10 cm per year and correlates with Tanner stage 3 to 4. On average, boys grow 31 cm taller during puberty, which is 17% of the final adult height.3 Measuring the length of the testis is an alternative to using an orchidometer; 2.5 cm along the long axis correlates to a testicular volume of 4 mL, indicating the start of puberty.
{kind=link}
{kind=link}
Other important aspects of the physical examination are recognising any midline defects (e.g. cleft palate, cardiac lesion, which may indicate a congenital abnormality of the pituitary gland), assessing visual fields to exclude a pituitary lesion and enquiring about olfactory nerve function, which may reveal underlying Kallmann’s syndrome. Kallmann’s syndrome is an uncommon condition with a prevalence of one in 8000. It is characterised by hypogonadotrophic hypogonadism and may be associated with anosmia.4 Klinefelter’s syndrome is more common, occuring in one in 580 live births.5 Boys with Klinefelter’s syndrome may have cryptorchidism, reduced muscle tone and learning or behavioural issues. Often, this syndrome is recognised for the first time in adulthood during investigation of infertility.5 Klinefelter’s syndrome should be considered in taller males with testes that remain under 4 mL despite otherwise advancing pubertal signs, especially if gynaecomastia is present.
How to investigate delayed puberty
Consider investigating to exclude organic causes if the clinical history suggests this (Table 1). A bone age assessment by x-ray of the left wrist will determine skeletal maturation compared with chronological age. The bone age will often lag behind the chronological age in delayed puberty. Blood tests for basal LH, FSH and testosterone levels may help to differentiate primary from secondary hypogonadism. An early morning blood sample should be collected for testosterone measurement.
Determining the aetiology of androgen deficiency
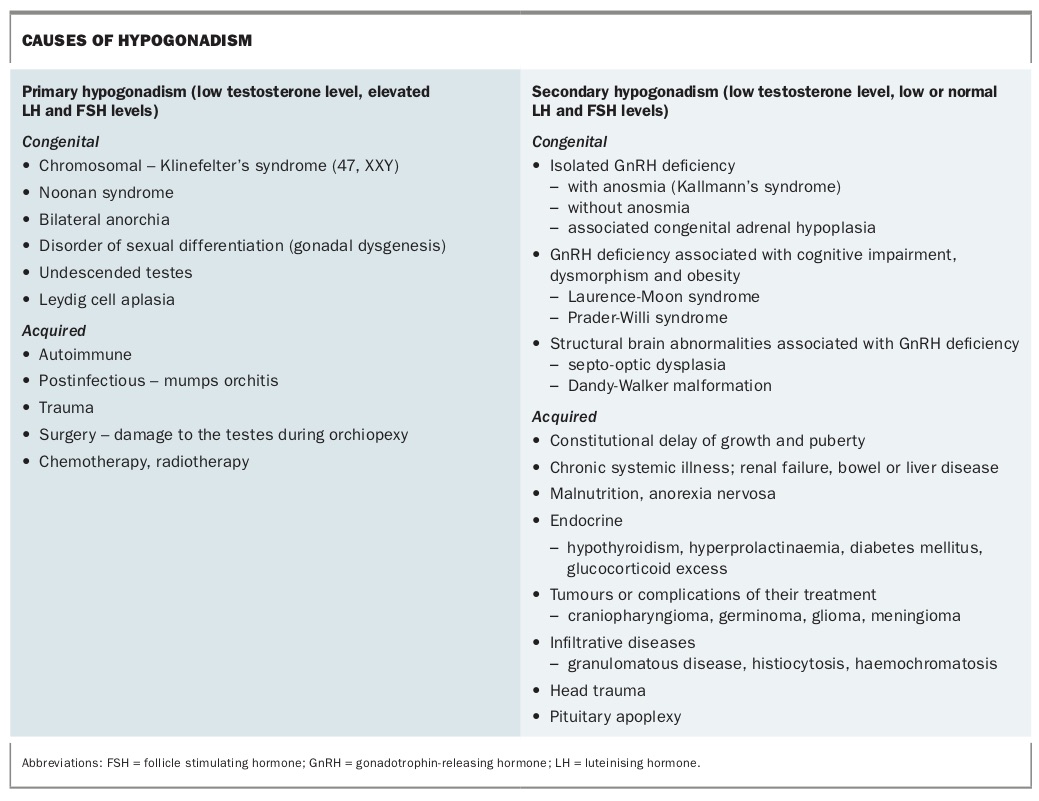
Causes of androgen deficiency can be divided into primary hypogonadism due to testicular dysfunction, or secondary hypogonadism due to dysfunction of the hypothalamus or pituitary. The most common cause of delayed puberty is constitutional delay of growth and puberty (CDGP). These healthy children have a slow growth rate and delay in pubertal onset. Bone age is often delayed and there may be a family history of CDGP. Other causes of primary and secondary hypogonadism are outlined in the Box. If androgen deficiency is suspected, referral to a paediatric endocrinologist is recommended for exclusion of pathological causes and discussion of management options.6
{kind=link}
Treatment options
Treatment of androgen deficiency usually involves testosterone therapy. The goal is to promote linear growth and development of secondary sexual characteristics and to facilitate normal acquisition of bone density. Pubertal induction is achieved with small and gradually increasing doses of testosterone over 18 to 24 months. The age at which pubertal induction is commenced varies according to the underlying condition and is generally from 12 to 14 years. Commonly, monthly intramuscular injections of testosterone enantate are prescribed for a short period (e.g. three to six months) to ‘kick-start’ puberty. Testosterone injections may be administered by a GP under the guidance of a paediatric endocrinologist.
If permanent androgen deficiency is diagnosed, testosterone maintenance therapy may be needed after pubertal development and linear growth are complete. Other available testosterone formulations, including capsules, patches, gel or cream, may also be used for pubertal induction.
Patient outcome
Daniel’s general examination results were normal, including visual field tests. Examination using a Prader orchidometer showed 5 mL testes bilaterally and stage 2 pubic hair, consistent with early puberty. His bone age was 13 years, which was significantly delayed. He was referred to a paediatric endocrinologist for ongoing surveillance. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.