Erectile dysfunction. Part 2: Management of ED unresponsive to PDE5 inhibitors

Although phosphodiesterase-5 (PDE5) inhibitors are regarded as first-line treatment for most men with erectile dysfunction (ED), they are not effective in about a third of cases. GPs have a pivotal role in management of this group, with a range of strategies and therapeutic options, including sex therapy, alternative medications, devices and surgery.
- About a third of men with erectile dysfunction (ED) fail to respond to a phosphodiesterase-5 (PDE5) inhibitor.
- The most common cause of initial PDE5 inhibitor failure is inadequate patient education or a failure to optimise dosage.
- Severe penile vascular disease, unrecognised hypogonadism, uncorrected comorbid disease, vascular risk factors or psychosocial factors are also associated with initial PDE5 inhibitor failure.
- Initial PDE5 inhibitor failure is almost universal after a radical prostatectomy.
- Treatment with self-administered intracavernous injection therapy, a vacuum constriction device, combination therapy or a penile prosthesis is likely to help men with ED unresponsive to PDE5 inhibitors.
Community-based epidemiological studies suggest that erectile dysfunction (ED) is common and associated with reduced quality of life.1,2 The introduction of phosphodiesterase-5 (PDE5) inhibitors has changed the ED treatment paradigm and decreased the use of more invasive options. PDE5 inhibitors have been shown to be effective and well tolerated in men with ED with a broad range of causes and severity. However, about a third of men fail to respond to an adequate trial of a PDE5 inhibitor. For these men there are a range of therapeutic options.
This is the second in a two-part series on ED. In Part 1 in the March 2020 issue of Medicine Today, we described assessment of patients with ED and treatment options.3 Here we describe the management of men with ED that does not respond to initial therapy with PDE5 inhibitors. We review the options currently available in Australia and propose an algorithm for the management of men with oral therapy failure (Flowchart).
PDE5 inhibitor therapy failure
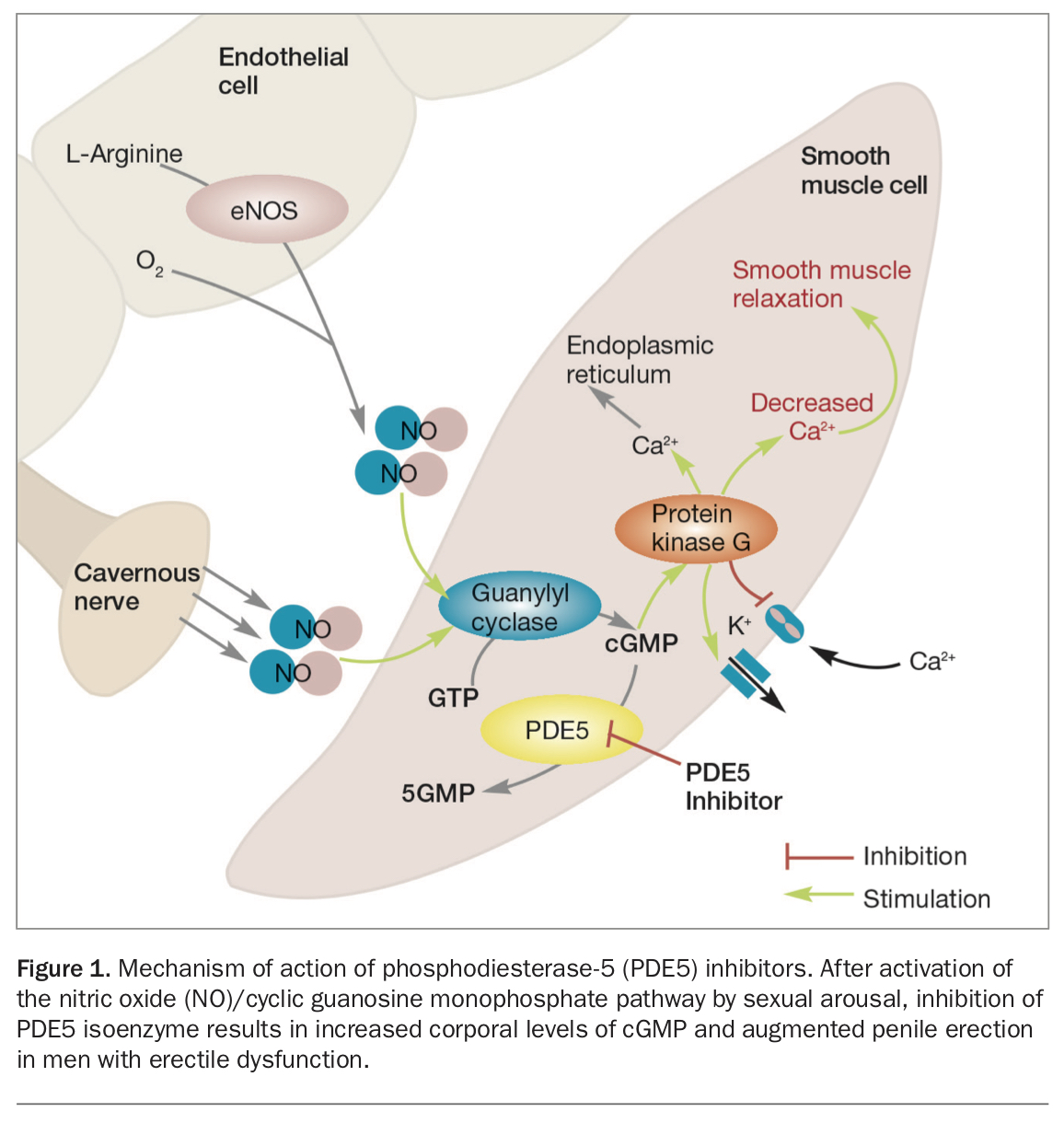
Four highly potent, selective PDE5 inhibitors (sildenafil, tadalafil, vardenafil and avanafil) are currently available and are regarded as first-line treatment for most men with ED. PDE5 inhibitors act via the nitric oxide-cyclic guanosine monophosphate (cGMP) pathway (see Figure 1 in Part 1 of this series in the March 2020 issue of Medicine Today).3 Sexual arousal activates this pathway, leading to relaxation of cavernosal smooth muscle cells, engorgement of lacunar spaces and erection. The enzyme PDE5, which is predominantly found within the corpora cavernosa, hydrolyses cGMP to 5-GMP, terminating the pathway and producing detumescence. PDE5 inhibitors compete with cGMP for the PDE5 receptor site, resulting in increased intracellular levels of cGMP and an augmented penile erection in men with ED.
{kind=link}
The efficacy and tolerability of PDE5 inhibitors have been demonstrated in men with ED with a broad range of causes and severities in multiple large multicentre clinical trials. However, 30 to 35% of patients fail to respond to PDE5 inhibitors. Furthermore, in men who do respond to PDE5 inhibitors, the reported drop in prescription renewal rates from 62% at three to four-month follow up to 50% at six to 12 months suggests there are many reasons in addition to treatment failure for discontinuing therapy.4
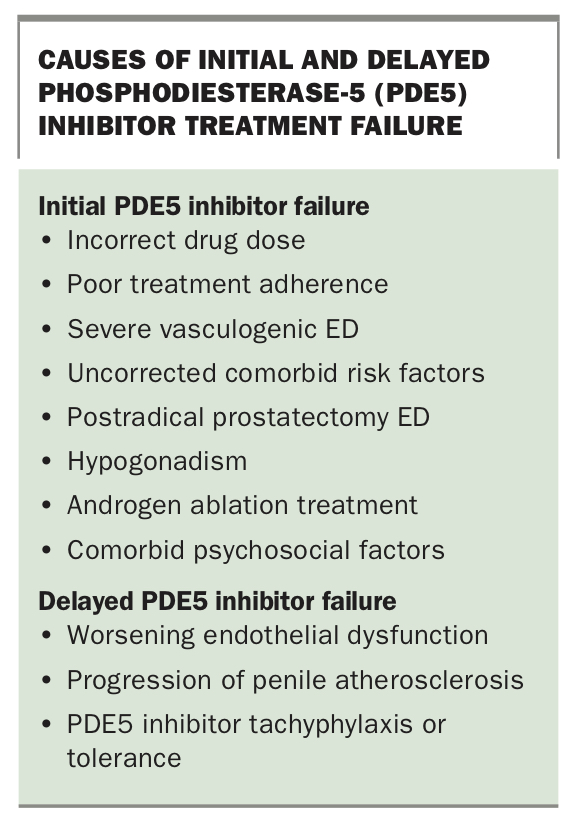
The reasons for initial or delayed PDE5 inhibitor failure are diverse and manifold. They include:
- severe ED at first presentation
- worsening of endothelial dysfunction and progression of penile atherosclerosis
- ED after radical prostatectomy
- unrecognised hypogonadism
- inadequate patient education and incorrect drug use
- possible development of tachyphylaxis or drug tolerance
- presence or development of comorbid psychosocial factors (Box).
{kind=link}
Several studies report that the response to PDE5 inhibitors is reduced in men with more severe ED and ED of longer duration, especially men with diabetes, higher levels of penile arterial insufficiency and corporal venous leakage and endothelial dysfunction.5,6
Therapeutic options for ED unresponsive to PDE5 inhibitors
GPs have a pivotal role in the management of men with ED that does not respond to treatment with a PDE5 inhibitor. Available treatment approaches include:
- referral to a specialist
- further patient education, including about appropriate use of PDE5 inhibitors
- dose optimisation, trial of an alternative PDE5 inhibitor or daily dosing
- correction of risk factors and lifestyle changes
- relationship and psychosexual counselling
- androgen replacement when indicated
- other medications (e.g. intracavernous injection therapy or combination therapy)
- vacuum constriction devices
- penile prostheses.
Referral
A busy GP may elect to refer men with ED that is refractory to a PDE5 inhibitor to a sexual health physician, urologist or other interested specialist.
Patient education
Treatment failure may result from inadequate education and incorrect drug use. Studies report that as many as 81% of patients initially took sildenafil incorrectly.7 Patient re-education can be effective in up to 55% of men who do not respond to sildenafil, as well as achieving improved drug efficacy and patient satisfaction.8,9 Initial education focusing on the following points can optimise treatment outcomes.
Adequate sexual stimulation
Patients must recognise that sexual arousal, ideally with a partner, is required to activate the nitric oxide-cGMP pathway involved in the action of PDE5 inhibitors.
Timing of administration
It is crucial that patients are advised of the time of onset of action of the specific PDE5 inhibitor they are taking as premature attempts at intercourse are likely to be unsuccessful. Sildenafil, vardenafil and avanafil are rapidly absorbed and can be taken 30 to 60 minutes before intercourse. Tadalafil does not achieve maximal plasma concentrations until two hours after dosing because of its longer time-to-maximum concentration (Tmax) of 2.5 hours. Although some men may respond to tadalafil as early as 16 minutes after dosing and about half may respond by 30 minutes, others, especially older men with vasculogenic ED, should be advised to take tadalafil at least two to three hours or longer before sexual activity.
Effect of alcohol and food
The time of onset and extent of response to sildenafil, vardenafil and avanafil are highly dependent on the effect of alcohol and food. Moderate-to-high fat meals or excessive alcohol may reduce the speed and extent of absorption of all three mediations. Advising patients to initially administer sildenafil, vardenafil or avanafil on an empty stomach will optimise their initial response, after which they can experiment with the effects of alcohol or food to determine the best timing of administration. The absorption of tadalafil is largely unaffected by food and alcohol, but occasional patients report a reduced response when it is taken after a fatty meal or excessive alcohol.
Duration of response
Delayed attempts at intercourse that fall outside the duration of effective PDE5 inhibitor plasma concentrations are likely to be associated with either drug failure or a reduced response. Sildenafil and vardenafil are rapidly cleared from the body and are active for four and eight hours, respectively. Tadalafil, with a half-life of 17.5 hours, is active for up to 36 hours. Anecdotally, some young men with psychogenic ED may report a response to PDE5 inhibitors in excess of that predicted by the drug’s pharmacokinetics.
Adequate trial of treatment
Although most men respond after one to two doses of a PDE5 inhibitor, some may require six to eight doses before an optimal response occurs.10
Dose optimisation
PDE5 inhibitor failure may be due to inadequate dosage. A study found that patient education, progressive dose titration to the maximum tolerated dose and use on at least four occasions achieved salvage rates of 32% and 44% among nonresponders to tadalafil and vardenafil, respectively.11
Recommended doses for on-demand dosing are as follows. These drugs should not be used more than once daily.
- Sildenafil should be initiated at a dose of 50 to 100 mg (25 mg for older patients and patients with hepatic cirrhosis or renal impairment) and titrated to achieve a maximal response.12 Doses higher than 100 mg may be effective but are associated with a significantly higher incidence of side effects and a 30% treatment discontinuation rate.
- Vardenafil should be initiated at a dose of 10 to 20 mg, with dose titration to achieve either an optimal response or a maximum dose of 20 mg.
- Avanafil should be initiated at a dose of 100 to 200 mg, with dose titration to achieve either optimal response or a maximum dose of 200 mg.
- Tadalafil should be initiated at a dose of 20 mg, the most common dose, but can be downtitrated to 10 mg in responders to identify the lowest effective dose.
Loss of efficacy caused by tachyphylaxis (decreased tissue responsiveness) is a concern with drugs that are administered frequently, and tolerance is possible for drugs that are used regularly for long periods. Tachyphylaxis has been suggested as a possible cause of the reported 17% sildenafil discontinuation rate after two years.13 Several possible biological mechanisms for tachyphylaxis and tolerance during PDE5 inhibitor treatment have been tested preclinically. In vitro, PDE5 expression or activity can be up- or down-regulated in response to nitric oxide and cGMP, but in animal models sildenafil did not affect PDE5 expression in the corporal smooth muscle. Consistent with this, most clinical studies do not suggest that clinically relevant tolerance to PDE5 inhibition develops during treatment periods ranging from about six months to four years.14,15 A more plausible explanation for decreased efficacy is progressive worsening of the patient’s underlying cause of ED, such as worsening atherosclerosis or diabetes.
Trial of another PDE5 inhibitor
Although the four PDE5 inhibitors have not been compared in direct head-to-head studies, it is likely that they have similar efficacy and tolerability. One study reported that only a small percentage (12%) of sildenafil nonresponders were responsive to vardenafil.16 However, as individual responses to these drugs may vary inexplicably, it is reasonable to offer patients a trial of a different PDE5 inhibitor before proceeding to more invasive treatments.
Daily dosing of a PDE5 inhibitor
Salvage of patients who fail to respond to on-demand tadalafil with daily or alternate day tadalafil has been reported but is limited by the relatively high cost of treatment.11,17 Treatment with daily tadalafil significantly improved all treatment outcomes in men previously unresponsive to on-demand tadalafil.17 The mean successful intercourse completion rate increased from 21% with on-demand 20 mg tadalafil to 58% with daily 10 mg tadalafil. The improved erectile response with daily tadalafil is probably related to improved endothelial function. PDE5 inhibitors have been reported to improve endothelium-dependent, flow-mediated vasodilation in patients with diabetes mellitus or chronic heart failure and in smokers.18
Improvement of comorbid conditions
Many men have underlying comorbidities that are risk factors for ED, including diabetes, hypertension, visceral obesity, cardiovascular disease, depression, prostatic hypertrophy, smoking, medications, a sedentary lifestyle and drug and alcohol abuse. Metabolic syndrome (the clustering of several cardiovascular risk factors including visceral obesity, hypertension, dyslipidaemia and glucose intolerance) is associated with a higher incidence of ED and a lower response rate to sildenafil.19,20
Control of these risk factors is an essential part of first-line ED therapy, to improve not only erectile function but also the patient’s response to therapy.21,22 One study reported that modifying associated risk factors before commencing sildenafil resulted in an improved overall success rate of 82%, with 77% of patients having success at every intercourse attempt.10 The success rate varied with different comorbidities and was lower in patients with multiple risk factors. Several studies quote higher success rates than those reported in studies where risk factors are not modified, suggesting that modification plays an important role in the success of oral therapy.21
Sex therapy
Psychosexual therapy involving individuals or couples focuses on improving sexual functioning. To be effective, ED therapy must go beyond the simple restoration of erectile function, and some cases require integrated treatment using psychosexual and pharmacological therapy.
Numerous psychological factors adversely impact on the efficacy of sildenafil and may result in therapy nonadherence, making it important to differentiate therapy nonresponse due to psychosocial issues from that due to biochemical failure.23 These psychological factors include:
- Negative reactions to treatment. Therapy may be perceived as temporary, unnatural or unacceptable. There may be unrealistic expectations or a fear of side effects and complications
- Partner attitudes. Regaining potency does not necessarily translate into the couple resuming sexual intercourse, and partner resistance may result in pharmacotherapy failure.24
Contributing factors include:
– the duration of sexual abstinence before seeking treatment
– the man’s approach to resuming sexual contact
– the partner’s physical and emotional readiness to resume sexual contact
– the quality of the nonsexual relationship.
Sex therapists are trained to address these issues and help maximise the patient’s response to the sexual situation. They can also re-motivate patients with oral therapy failure, making them more receptive to trying again or seeking further options. Although controlled outcome data examining the efficacy of this integrated approach is lacking, clinical experience indicates that it may be effective in cases where psychosocial issues exist.
Androgen replacement therapy in hypogonadal men
The role of androgen replacement therapy in ED is evolving. It is generally accepted that androgens play a role in overall male sexual function and erectile physiology, with deficiencies being commonly associated with hypoactive sexual desire and less often with ED.25 Animal studies have shown that apoptosis of corporal smooth muscle cells, reduced nitric oxide synthase and PDE5 gene expression, which occur after castration, are reversed by testosterone administration.26 Testosterone deficiency appears to predict a poor response to PDE5 inhibitors. Hypogonadal men who do not respond to PDE5 inhibitors might benefit from testosterone replacement.27-30 Furthermore, several studies report that topical testosterone treatment in men with ED and low baseline testosterone levels (less than 10.4 nmol/L) improves the erectile response to sildenafil, possibly by increasing arterial inflow to the penis during sexual stimulation.31-33
Intracavernous injection therapy
Intracavernous injection therapy involves self-administration of vasodilator drugs, which act by relaxing arterial and trabecular smooth muscle resulting in an erection. It is regarded as second-line ED therapy and should be considered when oral therapy fails. The most commonly used intracavernous drugs are alprostadil and a combination of papaverine, phentolamine and alprostadil.
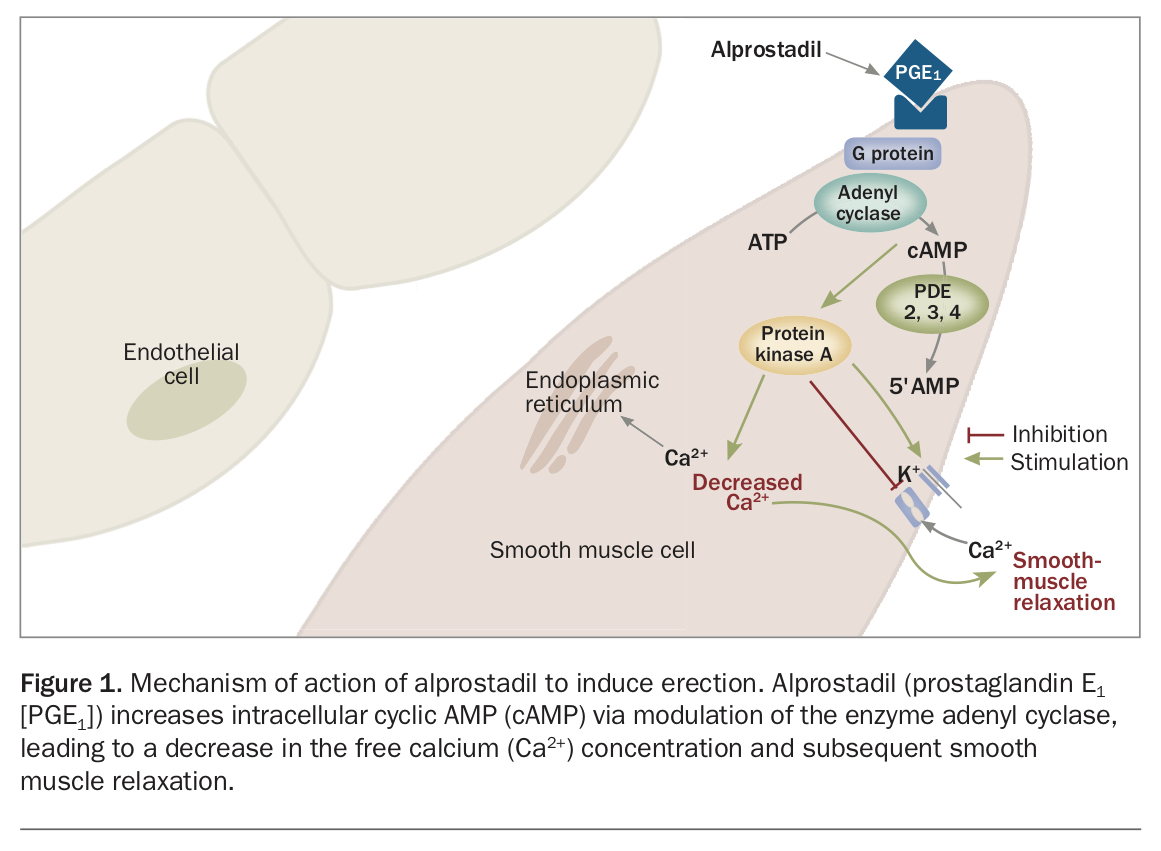
Alprostadil modulates the action of the enzyme adenyl cyclase, increases intracellular cAMP and leads to relaxation of corporal smooth muscle cells and erection (Figure 1). Furthermore, cAMP may exert a positive feedback on the nitric oxide-cGMP pathway and further increase cGMP levels. Intracavernous alprostadil has a response rate of more than 70% and is considered superior to other intracavernous drugs in regard to risk of complications.34 This treatment is effective and safe in patients who do not respond to initial sildenafil therapy, with 88% of patients reporting at-home treatment success.35 The most commonly reported adverse effects include penile pain, fibrosis and priapism.
{kind=link}
Therapy with the combination of papaverine, phentolamine and alprostadil may be effective treatment for patients who do not respond to alprostadil monotherapy. A comparative study reported a 91.6% response rate for the three-drug combination.36
Combination therapy
PDE5 inhibitor nonresponders may respond to combination therapy with agents that act synergistically because of their different mechanisms of action. This approach may also allow lower drug doses and have a reduced incidence of adverse effects. The most popular approaches use sildenafil and intracavernous alprostadil. One study reported that of 61 men who had previously failed to respond to an adequate trial of either intracavernous injection therapy or sildenafil, (48%) responded to combination therapy.30,37 However, 33% of patients reported adverse events, including a 20% incidence of dizziness; these adverse events were described as largely mild to moderate in severity and responsible for treatment discontinuation in 14%.
Despite the growing evidence that combination therapy may be effective in patients in whom monotherapy fails, double-blind randomised controlled trials are needed to establish the benefits, optimal dosage, possible adverse effects and patient acceptance of combination therapies.
Vacuum constriction devices
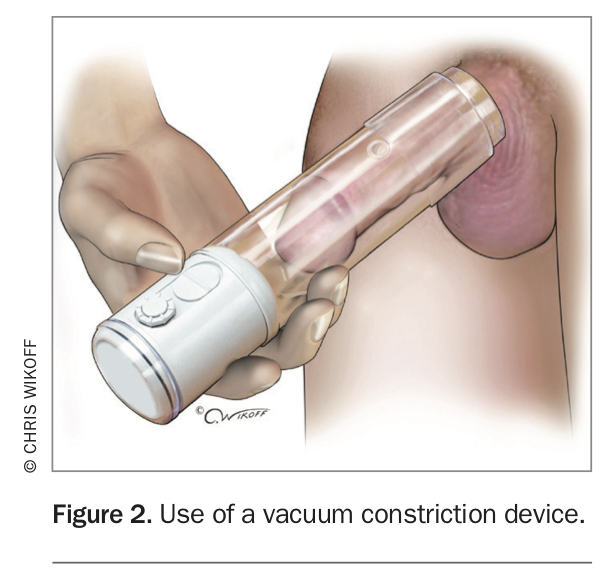
Vacuum constriction devices may appeal to men who are either not interested in or not suitable for pharmacological treatment. They are the least invasive option and are inexpensive. Vacuum constriction devices are made of a clear plastic cylinder with either an integrated battery or attached hand pump and a collection of sizes of constriction rings. They act by applying negative pressure to the penis, which increases the blood flow into the corpora cavernosa. The resulting engorgement is maintained by a constriction ring at the base of the penis, which prevents venous outflow and should be removed within 30 minutes (see Figure 2 in Part 1 of this series in the March 2020 issue of Medicine Today).3
{kind=link}
The device can be used daily, and reported success rates range between 70% and 94%.38,39 The associated side effects include penile pain, numbness, bruising and obstructed ejaculation. Currently, there are no studies examining the combination of PDE5 inhibitors and vacuum constriction devices.
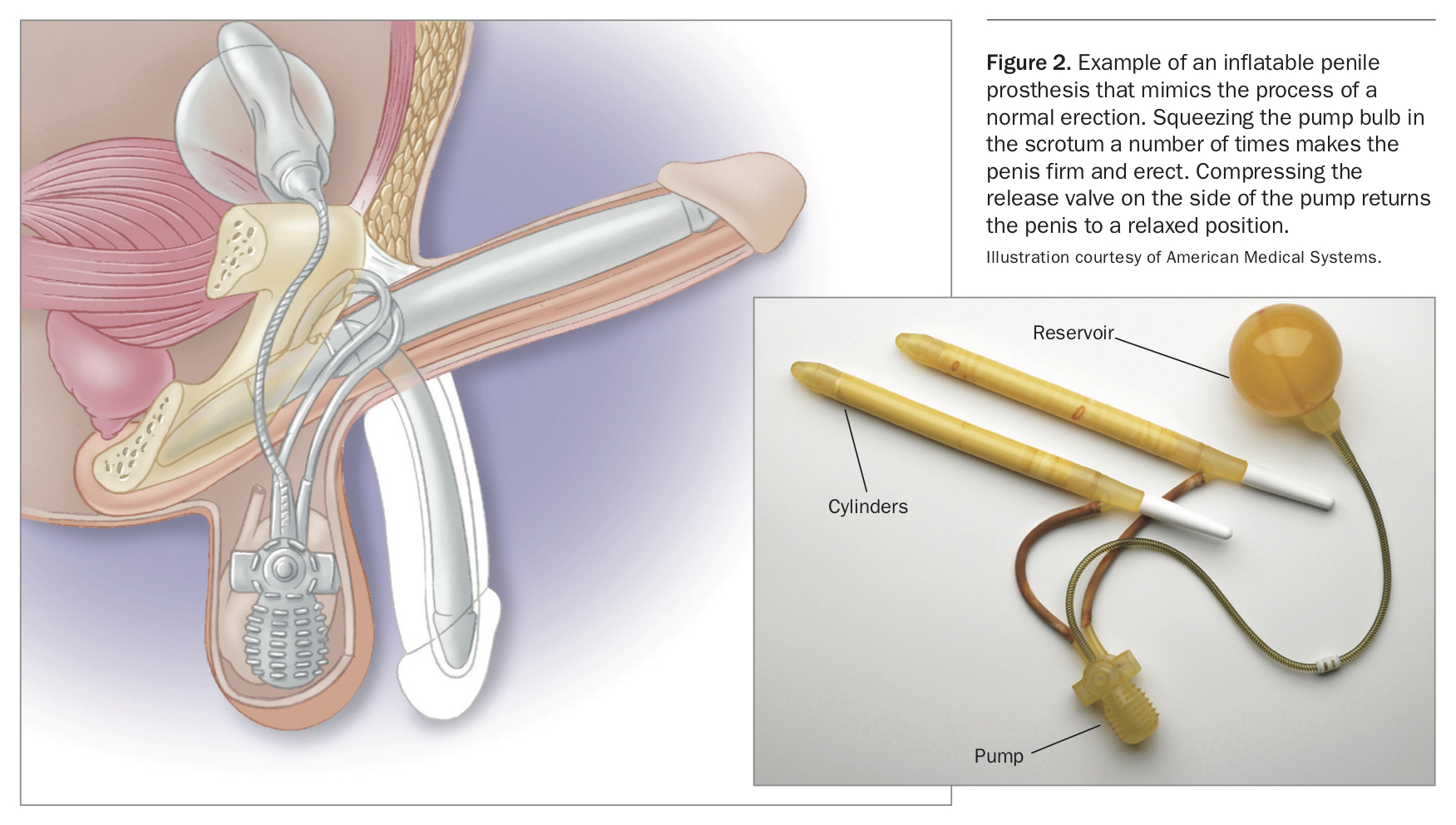
Penile prostheses
Patients with severe, pharmacotherapy-refractory ED are often best treated with the implantation of a penile prosthesis (Figure 2). Populations with a high incidence of pharmacotherapy failure include men with ED due to diabetes, radical prostatectomy, Peyronie’s disease and severe penile fibrosis. Penile prosthetic surgery has demonstrated very high long-term mechanical reliability and excellent patient satisfaction rates of more than 85%.40,41 Infection is one of the most serious complications. However, infection rates have decreased remarkably after the introduction of antibiotic-coated penile prostheses.42
{kind=link}
Treatment of ED after treatment of prostate cancer
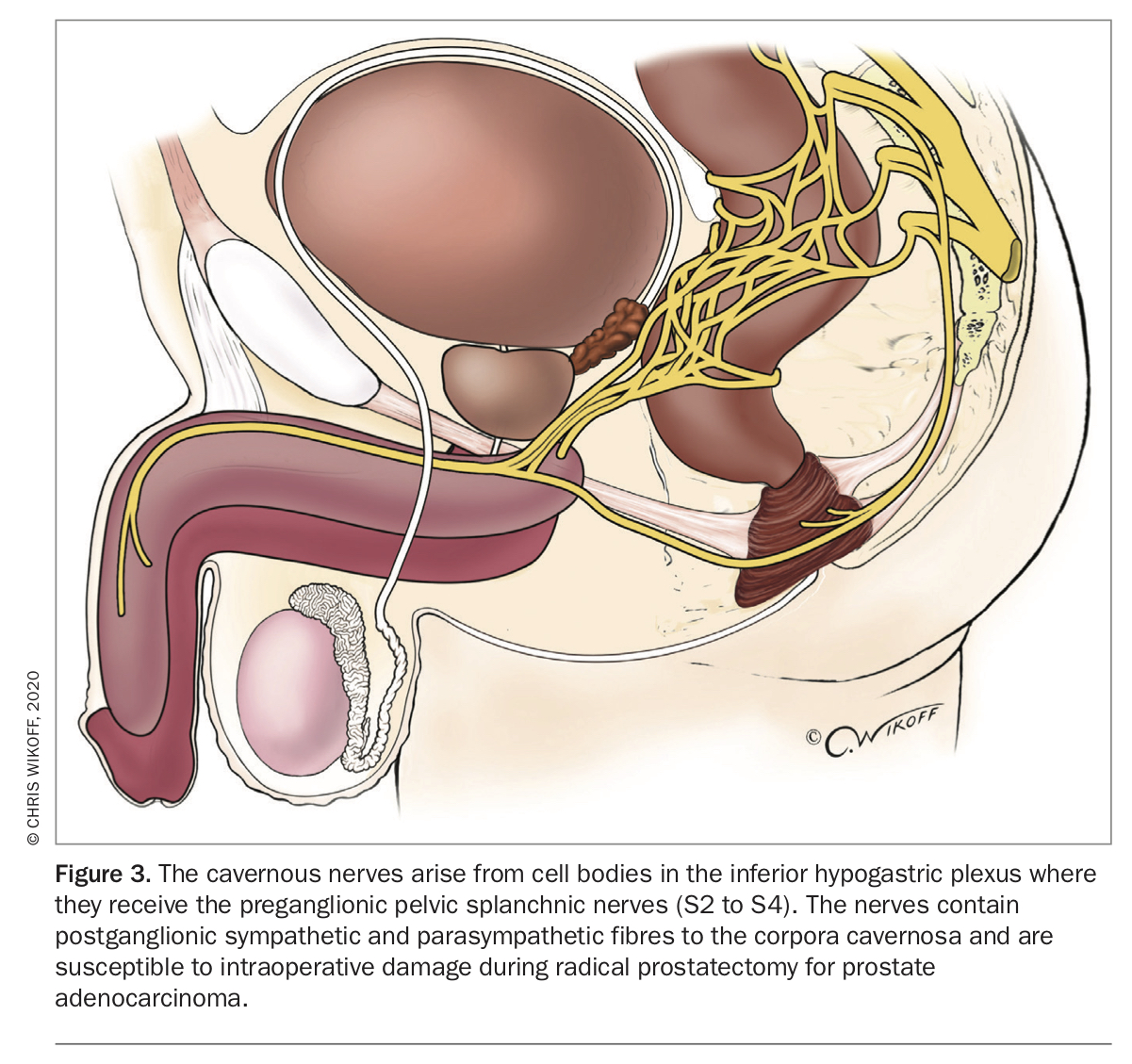
ED is a common consequence of treatment of prostate adenocarcinoma with radical retropubic prostatectomy, external beam radiotherapy, brachytherapy or androgen deprivation.43,44 The aetiology of ED after open or robotic radical retropubic prostatectomy includes operative injury to the cavernous nerves and subsequent increased hypoxia-induced production of transforming growth factor beta 1 in the corpora cavernosa (Figure 3). This leads to increased extracellular matrix deposition, inhibition of smooth muscle growth, apoptosis of corporal smooth muscle, fibrosis and eventually structurally based corporeal veno-occlusive dysfunction.43
{kind=link}
An initial challenge with a PDE5 inhibitor is important to establish baseline cavernous nerve function after radical prostatectomy, but failure to respond to PDE5 inhibitors is almost universal. This is the result of cavernous nerve injury with subsequent failure to activate the nitric oxide-cGMP pathway. Overall, about 30 to 40% of patients will eventually respond to PDE5 inhibitors after nerve-sparing radical retropubic prostatectomy.45 Response rates of up to 70% are seen in men younger than 60 years with normal preoperative erections who undergo an anatomical bilateral nerve-sparing procedure. However, intraoperative cavernous nerve neuropraxia is common during nerve-sparing radical prostatectomy, and recovery of cavernous nerve function may be protracted and incomplete. This results in a failure to respond to PDE5 inhibitors for as long as 24 to 36 months or a need for long-term use of intracavernous injection therapy.46
Preoperative counselling about the high incidence of ED and early treatment of ED after radical prostatectomy with self-administered intracavernous injection of alprostadil (starting dose of 2.5 mcg) is associated with a high response rate, return to an active sexual life, and a greater prospect of a subsequent response to PDE5 inhibitors and eventual restoration of spontaneous erections.47
Adverse effects include postinjection penile aching, often lasting for several hours, which is reported by approximately 40 to 50% of men using self-administered alprostadil intracavernous injection therapy and is the most common reason for discontinuing treatment. Treatment outcomes with vacuum constriction devices are relatively poor, and their use is characterised by relatively low levels of patient and partner satisfaction and high discontinuation rates.
Serial re-challenge with PDE5 inhibitors every one to two months will establish the extent of cavernous nerve recovery and identify candidates for PDE5 inhibitor treatment. There is early evidence to support a potential role for PDE5 inhibitors, especially long half-life PDE5 inhibitors such as tadalafil administered daily or three times weekly, as an adjunct to initial treatment with intracavernous injection therapy in promoting the return of erectile function in men after nerve-sparing radical retropubic prostatectomy.48,49
ED after external beam radiotherapy or brachytherapy is insidious and progressive. It is caused by radiation-induced microvascular endarteritis of the penile arteries, possible acceleration of pre-existing atherosclerosis and proximal corporal fibrosis. In men with ED after external beam radiotherapy or brachytherapy, the response rate is similar to that of age-matched ED control subjects.50
Androgen blockade with androgen receptor blocking drugs (e.g. cyproterone acetate, flutamide and bicalutamide) or luteinising hormone releasing hormone agonists (e.g. goserelin and leuprorelin) is often associated with hypoactive sexual desire, ED, delayed ejaculation, anejaculation and anorgasmia.51 ED due to androgen blockade can be challenging to treat, although treatment is often not requested because of hypoactive sexual desire. The response to PDE5 inhibitors is reduced as the low testosterone levels reduce expression of both the nitric oxide synthase gene and the PDE5 gene and downregulate PDE5 enzyme. Similarly, the response to self-administered intracavernous injection therapy is also reduced.
Conclusion
The introduction of oral PDE5 inhibitors has significantly changed the treatment of ED. For the 30 to 35% of men who fail to respond to oral PDE5 inhibitors, several effective pharmacological and surgical treatment options are available as salvage therapy. Busy GPs may elect to refer patients with ED that is refractory to oral PDE5 therapy to a urologist, sexual health physician or other interested specialist. GPs with an interest in male sexual health and specialists who manage sexual dysfunction can successfully treat most patients with PDE5 inhibitor-refractory ED using one or a combination of approaches. This will consequently improve the sexual and overall quality of life of patients and their partners. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.