Childhood obesity. An approach to management

Children's health
It is important that GPs take the initiative and sensitively address overweight and obesity in young patients. Once this initial barrier is overcome, motivating patients and their families to adopt simple lifestyle interventions can lead to significant improvement in health and psychosocial outcomes.
Children with overweight or obesity present to health professionals more frequently than children whose weight is within the healthy range. Most do not present because of concerns about weight, but rather because of issues such as recurrent ear infections, asthma, constipation or bed wetting, all of which may be exacerbated as a direct result of excessive weight gain. The first challenge for health professionals, particularly because awareness is often absent, is how to raise the issue of overweight in a child with the parents.
Raising the issue
The NHMRC Clinical Practice Guidelines for the Management of Overweight and Obesity in Adults, Adolescents and Children in Australia recommend the ‘5 As’ approach to management of obesity: ask, assess, advise, assist and arrange.1 However, parents, and especially those who are overweight or obese themselves, have difficulty recognising obesity in their children. Even health professionals find it difficult to categorise a child’s weight status by visualisation alone.
As well as lack of awareness and raising the issue, barriers to managing childhood obesity include lack of time, resources and training in the area, and lack of specific MBS remuneration. Many GPs do not routinely weigh children or raise the topic of excessive weight gain for concerns of negative parental responses. Yet most parents expect the GP to measure their child’s weight, raise issues, offer counselling on diet and exercise and provide follow-up appointments.
Ask
Having a strategy to measure a child’s height and weight at each clinic visit would simplify raising weight-related concerns and allow calculation of body mass index (BMI) and subsequent plotting of BMI-for-age using gender-specific growth charts. For busy practices, monitoring patients’ weight can be a challenge; however, a practice nurse could undertake the measurements and help to engage with the family. The process would then become standard practice and trends in weight gain could be identified and addressed early.
Growth charts can be used to start conversations about weight; for example, by saying ‘Looking at Lucy’s growth chart we can see her BMI is above the healthy range for her age. Is this something you have noticed or been concerned about?’ If the reason for the current visit was not because of weight-related concerns then a follow-up appointment could be offered by saying, ‘I realise you have not come to see me about this today, but how about we book another appointment to discuss it further?’ It is important when raising the issue to use sensitive language, avoid stigmatising or blaming and be supportive and solution orientated.
Assess
In a busy practice, time is of the essence. Developing a systematic approach to assessment that screens for problems that may need treatment or intervention would be beneficial.
History taking
On presentation, ask the parent and, in the case of adolescents, the young person themself, what their concerns are. If the concerns are weight-related, determine whether the patient or their family have previously attempted to lose weight or change their habits, and their degree of success. Thorough history-taking would include the following areas.
- Potential underlying causes (rare in childhood) and comorbidities, for example:
- sleep problems (ask about hours slept, night-time wetting, snoring, morning headache, daytime somnolence)
- systemic issues (ask about exacerbation of asthma, exercise tolerance levels, constipation, daytime wetting, lower-limb joint pain)
- psychosocial or behavioural problems (ask about bullying, school refusal, depression, attention deficit hyperactivity disorder and autism, all of which have an increased prevalence in children with obesity).
- Is there a family history of type 2 diabetes, obesity, or bariatric surgery?
- Take into account the increased risk of developing obesity and comorbidities among people of Asian, Middle Eastern, Indigenous Australian and Pacific Islander races.2
- Ask about screen time, including recreational use of small and large screens and the presence of televisions in bedrooms.
- Ask about physical activity, including how much organised versus incidental activity the child participates in, parental role modelling and family activities.
- In relation to diet, what are the eating patterns of the child and family?
Are meals regular (including breakfast). What are their snacking and drinking habits? How much fruit, vegetables and fast food are consumed? Is the television on at meal times?
Physical examination
Other than generalised or central obesity, physical examination of a child with overweight or obesity is often within normal limits. Look for acanthosis nigricans (especially of the neck, axillae and inner thigh), other skin lesions (striae, intertrigo), tonsillar size, gait and range of hip movement. Blood pressure should be measured using an appropriately sized cuff, and waist circumference can be measured to calculate the child’s waist-to-height ratio (a ratio of greater than 0.5 is associated with increased cardiometabolic risk).
Investigations
Most children with overweight or mild obesity will not require any further investigations. However, consider further investigations in patients with one or more of the following characteristics: older adolescent, significant obesity, a strong family history of type 2 diabetes, a history or physical examination suggestive of comorbidities, and short stature. If blood tests are required, they should be fasting levels and include liver function tests, a lipid profile, insulin and glucose levels, iron studies and vitamin D level. Thyroid- stimulating hormone should be measured in patients of short stature and when height plateaus prematurely. If the patient potentially has obstructive sleep apnoea then refer them for a sleep assessment.
Advise and assist
Priorities will dictate the advice given. Family-wide behaviour change is needed, which will likely benefit the health of all family members. Motivational interviewing techniques can be used to determine what the family feels they could address.3 ‘SMARTER’ goal techniques will help them to clarify goals and to focus on why they might want to make changes. SMARTER goals are specific, measurable, achievable, relative, timely and associated with an emotion and a reward. Adolescents may choose the goal and be supported by parents.
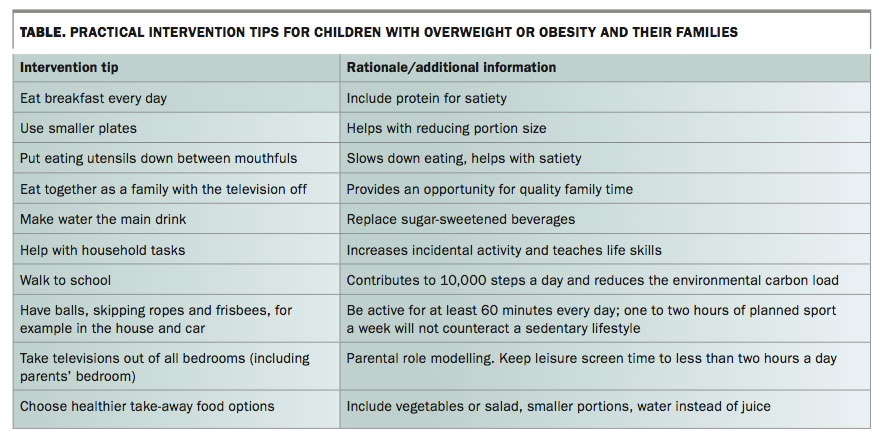
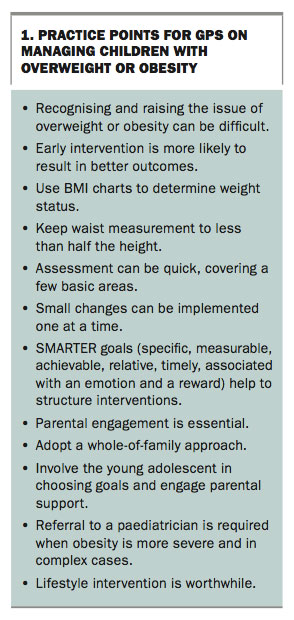
It is often easier to make small changes one step at a time. Regular support and follow up is needed for monitoring and feedback through serial measurements and discussing achievements. The table lists simple intervention suggestions, and Box 1 summarises practice points for GPs.
{kind=link}
{kind=link}
Arrange
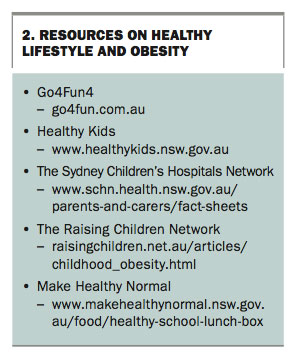
Refer the patient to local dietetic, physiotherapy and clinical psychology services for additional input if they are available, or community programs such as Go4Fun4 in New South Wales (go4fun.com.au; a free 10-week healthy lifestyle program). Resources on healthy lifestyle and obesity are listed in Box 2.
{kind=link}
In complex cases or severe obesity (BMI greater than the 99th centile for age), refer the child or adolescent to a paediatrician for further assessment and management of contributing factors, comorbidities and existing health issues that have been exacerbated. Adjunct treatments such as medications (orlistat [off-label use]), very low energy diets or consideration of bariatric surgery should be undertaken only by a specialist multidisciplinary weight-management team. Bariatric surgery may be considered in adolescents who are more than 14 years of age or postpubertal with a BMI greater than 40 kg/m2 or greater than 35 kg/m2 with comorbidities.4
Conclusion
Having a strategy for managing overweight and obesity in children and adolescents is highly important in primary practice. Lifestyle interventions can produce significant results in children and adolescents with obesity in both the primary care and tertiary settings. They are certainly worthwhile undertaking, particularly when improvements in psychosocial outcomes are observed.5 MT
References
- National Health and Medical Research Council (NHMRC). Clinical practice guidelines for the management of overweight and obesity in adults, adolescents and children in Australia. Melbourne: NHMRC; 2013. Available online at: https://www.nhmrc.gov.au/guidelines-publications/n57 (accessed June 2017).
- Fernández JR, Allison DB. Understanding racial differences in obesity and metabolic syndrome traits. Nutr Rev 2003; 61: 316-319.
- Hall K, Gibbie T, Lubman DI. Motivational interviewing techniques - facilitating behaviour change in the general practice setting. Aust Fam Physician 2012; 41: 660-667.
- Baur LA, Fitzgerald DA. Recommendations for bariatric surgery in adolescents in Australia and New Zealand. J Paediatr Child Health 2010; 46: 704-707.
- Banks J, Sharp DJ, Hunt LP, Shield JPH. Evaluating the transferability of a hospital-based childhood obesity clinic to primary care: a randomised controlled trial. Br J Gen Pract 2012; 62: e6-e12.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.