Understanding developmental co-ordination disorder

Developmental co-ordination disorder is a neurodevelopmental disorder that can affect a child’s daily activities, social and leisure participation, academic achievement and emotional and psychological wellbeing. Awareness and diagnosis by primary healthcare professionals will help families and children by enabling timely intervention to improve outcomes.
Developmental co-ordination disorder (DCD) is a potentially lifelong neurodevelopmental condition in which motor skill performance is delayed, awkward, slow or poorly co-ordinated to the extent that it affects everyday tasks. This can in turn affect the individual’s academic progress, social integration and emotional development. It typically occurs in 5 to 6% of school-aged children.1 Research has shown that the incidence of DCD is much higher in children who were born preterm or with low birthweight and in boys.2
DCD is one of the most underdiagnosed developmental conditions of childhood and one of the greatest causes of long-term morbidity. It is often misunderstood and misdiagnosed by health professionals, including in Australia.3 Achieving an accurate diagnosis can take two to four years for many Australian children, resulting in parental frustration and limited understanding of what lies behind their child’s difficulties.4
A recent survey of 443 Australian children with movement difficulties identified nine separate diagnostic terms that were used when children with DCD received a diagnosis.4 More concerningly, the survey found that children with DCD were more often diagnosed as having dyspraxia; although this term is often used synonymously with DCD, it is not a formal clinical diagnosis.4 Such inconsistent use of terminology is confusing for both parents and health professionals, as it may lead to misunderstanding the cause of the child’s difficulties and result in inappropriate treatment options. International clinical practice guidelines recommend that alternative labels for DCD, such as dyspraxia, should not be used.1 Therefore, promoting the consistent use of ‘developmental co-ordination disorder’, as stated in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), will standardise the approach to diagnosis and understanding of the problems involved, which should then lead to a more comprehensive approach to intervention.5
Primary symptoms
According to the DSM-5, the criteria that need to be met for a diagnosis of DCD to be made are:
- learning and execution of co-ordinated motor skills are below the level expected, given the person’s age and opportunity for learning skills
- difficulties with motor skills significantly interfere with activities of daily living and affect academic or school productivity, prevocational and vocational activities, leisure and play
- onset occurs in the early developmental period
- difficulties with motor skills are not better explained by intellectual delay, visual impairment or other neurological conditions that affect movement.5
Although international clinical practice guidelines recommend a diagnosis of DCD being made when a child is over 5 years of age, a diagnosis can be made earlier if the problem is severe and occurs across multiple environments, such as at home and preschool.1
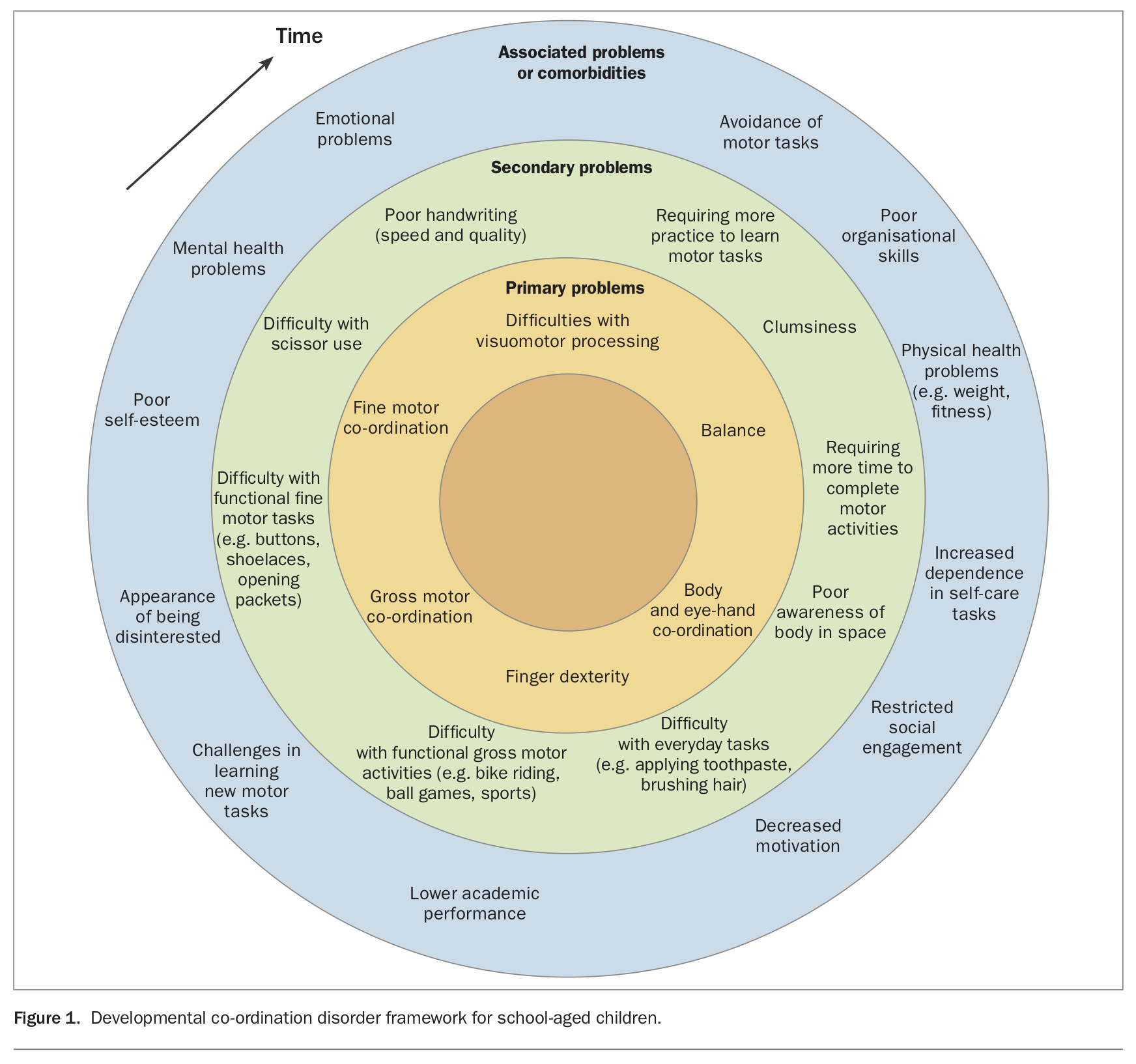
Examples of the difficulties a child may present with are shown in Figure 1. This set of symptoms may previously have been referred to as developmental dyspraxia, ‘clumsy child syndrome’, DAMP (deficits in attention, motor control and perceptual abilities) or perceptuomotor dysfunction.6,7
{kind=link}
DCD does not require a history of delay in meeting motor skill milestones for diagnosis. Rather, children can present with a range of fine motor difficulties (e.g. problems with handwriting, tying shoelaces or doing up buttons), self-care difficulties (e.g. applying toothpaste, brushing hair, using cutlery), gross motor difficulties (e.g. balancing, cycling, dancing, swimming) and planning and organising challenges (Figure 1). DCD is often not even considered because these presentations are accounted for by broader diagnostic categories (diagnostic overshadowing).8
Secondary effects
DCD affects more than motor performance. The evidence suggests that the flow-on effects of the motor challenges in DCD can include disengagement from typical family routine activities, limited social participation with peers and restricted engagement in everyday activities (Figure 1), with these becoming recurring problems for children with DCD.9-12
Larger movements, such as balance and ball skills, are considered essential prerequisites for children’s free play activities and team games and will therefore often determine whether a child is accepted or rejected by peers.10-13 If these problems are not dealt with, the impact can be detrimental and compound as the young person progresses through their education.3 In this way, DCD is similar to other neurobiological conditions that affect children, such as attention deficit hyperactivity disorder (ADHD) or specific learning difficulties, as what appear to be minor difficulties have major implications for many children in their everyday lives, particularly during their school years.9,11-13
Both parents of children with DCD and the children themselves report that DCD affects a child’s social, psychological and emotional wellbeing. Compared with parents of children without DCD, parents of children with DCD report difficulties with the child’s mood, home life and bullying. Compared with their peers, the difficulties self-reported by children with DCD include problems with mood and emotions, poorer physical and psychological wellbeing, problems with parents and problems with home and school life.14
Seventy per cent of children diagnosed with DCD will have difficulties that persist into adolescence and adulthood.15 They have greater difficulty with new complex motor tasks, such as learning to drive, and find it more challenging to gain employment.16 Research has also shown that adolescents with DCD have greater difficulties with reading and need more academic support than those without DCD. Children with DCD score more poorly on final academic assessments, which has implications for further education and employment.17
Comorbidities associated with DCD are the rule rather than the exception. For example, DCD is known to be correlated with conditions such as executive and motor planning difficulties, learning difficulties, ADHD and autism spectrum disorder.6 Overweight and obesity are over-represented in children with DCD.18
Pathophysiology and risk factors
The pathophysiology of DCD is not well understood. Its heterogeneous presentation suggests that there are several neurodevelopmental mechanisms associated with the condition. The two main hypotheses are that:
- DCD is caused by deficits in motor imagery (mental representation of movement), leading to deficits in planning motor actions
- DCD is a result of a deficit in the relationship between perception and action (learning how to control movement and co-ordinate body segments is dependent on the correct interpretation of the sensory experience).
Studies involving brain activation patterns show differences of activation loci between the brains of children with DCD and typically developing children, suggesting that children with DCD are neurobiologically different to their typically developing peers. However, these studies have been critiqued for their rigour and small sample sizes, so more research is required to confirm these findings.6
There are risk factors associated with DCD. A systematic review conducted in 2011 showed that people who had been born with very low birthweight or very preterm had a higher prevalence of, and greater odds of developing, DCD than full-term and normal birthweight children.19 Other studies have also shown more adverse neurological outcomes for preterm male than female infants, possibly accounting for the discrepant male-to-female ratio in DCD.7 In a population-based study in China that used retrospectively collected obstetric data to examine the relationship between prenatal risk factors and DCD, children with DCD were more likely to have had complications in the antenatal and perinatal period. Maternal age, threatened miscarriage at less than 20 weeks, physical distress during labour, preterm birth, chronic lung disease and newborn pathological jaundice were all found to be independently associated with DCD in school-aged children.20
Identification in primary healthcare
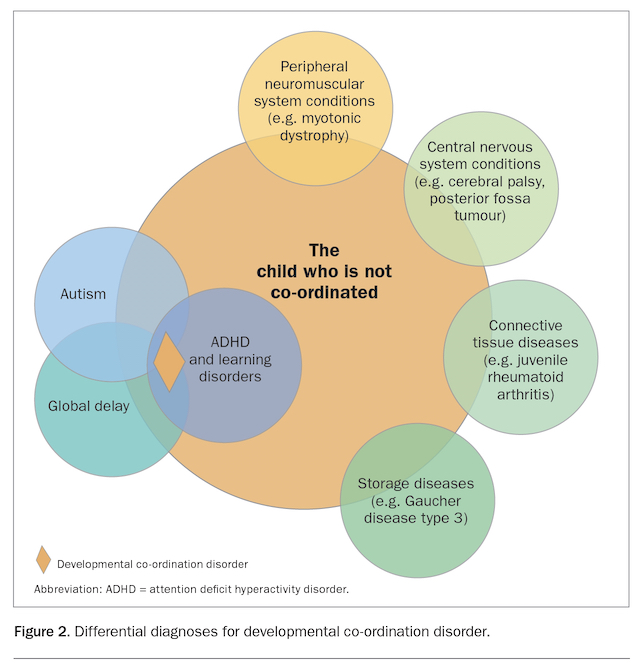
Identification of motor problems is best handled in primary healthcare. However, this advice comes with an awareness that the earlier the presentation, the more undifferentiated the signs can be. Hence, although early identification is advisable, it is also important to consider differential diagnoses when a preschool-aged child presents with difficulties suggestive of DCD. Other conditions that may need to be excluded are those involving the peripheral neuromuscular system or central nervous system, connective tissue or storage diseases, or broader problems such as developmental delay or autism (Figure 2).6-8 DCD is most often diagnosed in school-aged children who present with learning difficulties.
{kind=link}
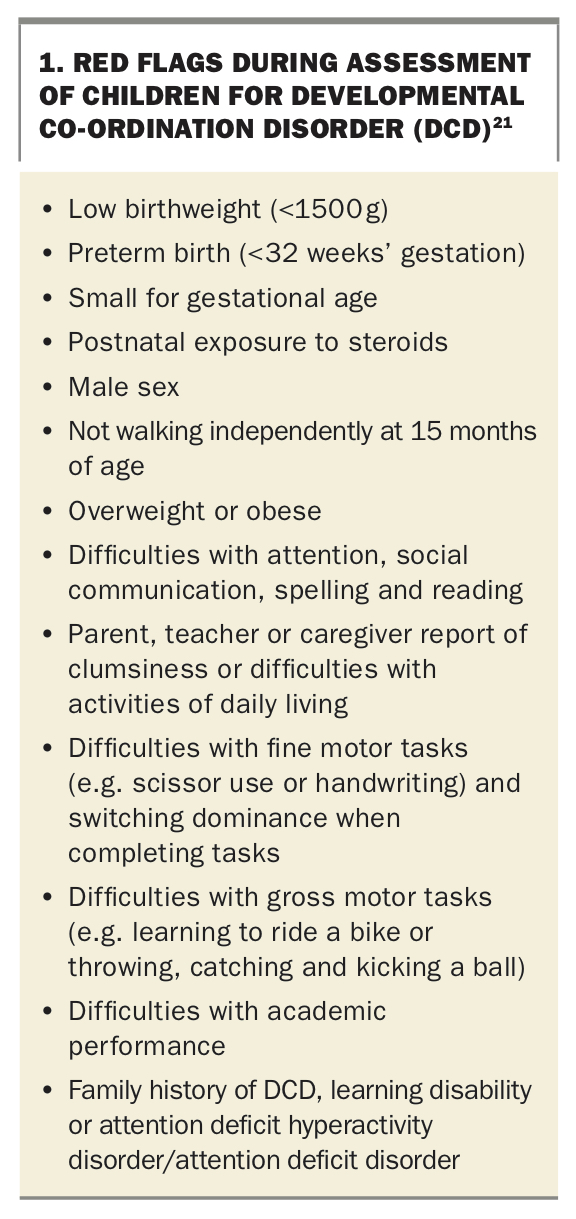
When investigating the possibility of DCD in a child, red flags that suggest further assessment is indicated are shown in Box 1.21 The Developmental Coordination Disorder Questionnaire (DCDQ) is a valid clinical reporting tool for identifying children aged 5 to 15 years who have motor co-ordination difficulties, and it can assist in the diagnostic process. The DCDQ is a brief questionnaire containing 15 statements about a child’s engagement in motor skills. GPs can provide the DCDQ to parents for them to take home and rate their child’s skills using a five-point rating scale and bring it back for review at a following appointment. Total scores are calculated to provide information on whether there is an ‘indication of DCD’, ‘suspected DCD’ or ‘probably not DCD’. The questionnaire is available at no cost at www.dcdq.ca. For children aged 3 to 5 years, the Little DCDQ is available for a nominal fee.
{kind=link}
Diagnostic process
As there are multiple dimensions to DCD, it is recommended that the diagnostic process include multidisciplinary assessments. This often involves a paediatrician, occupational therapist, physiotherapist and psychologist. If there are concerns about other developmental areas, referral to relevant specialists, such as a speech therapist, learning specialist or autism/ADHD specialist, is recommended. It is helpful if GPs are familiar with their respective local health pathways and referral processes for these specialists. A GP’s local HealthPathways website can provide more information.
An algorithm to guide primary care physicians through the assessment and management of a child with DCD is shown in the Flowchart.
Intervention
Whether a diagnosis of DCD is made in early childhood or not, interventions that tackle functional problems should be put in place to facilitate better outcomes.6-8 Research has shown that intervention has a moderate to large effect for children with DCD, with task- oriented approaches generally having the strongest evidence.22 For example, the Cognitive Orientation to (Daily) Occupational Performance (CO-OP) treatment approach has strong evidence to support its effectiveness.23 This approach actively engages the client in cognitive strategies to find solutions to problems. Occupational therapists are increasingly trained in CO-OP and can provide intervention directed at specific family- and client-centred goals that relate to improved functional (occupational) outcomes and reduction in core symptoms. Physiotherapists may also be able to provide intervention targeting gross motor skills more specifically.
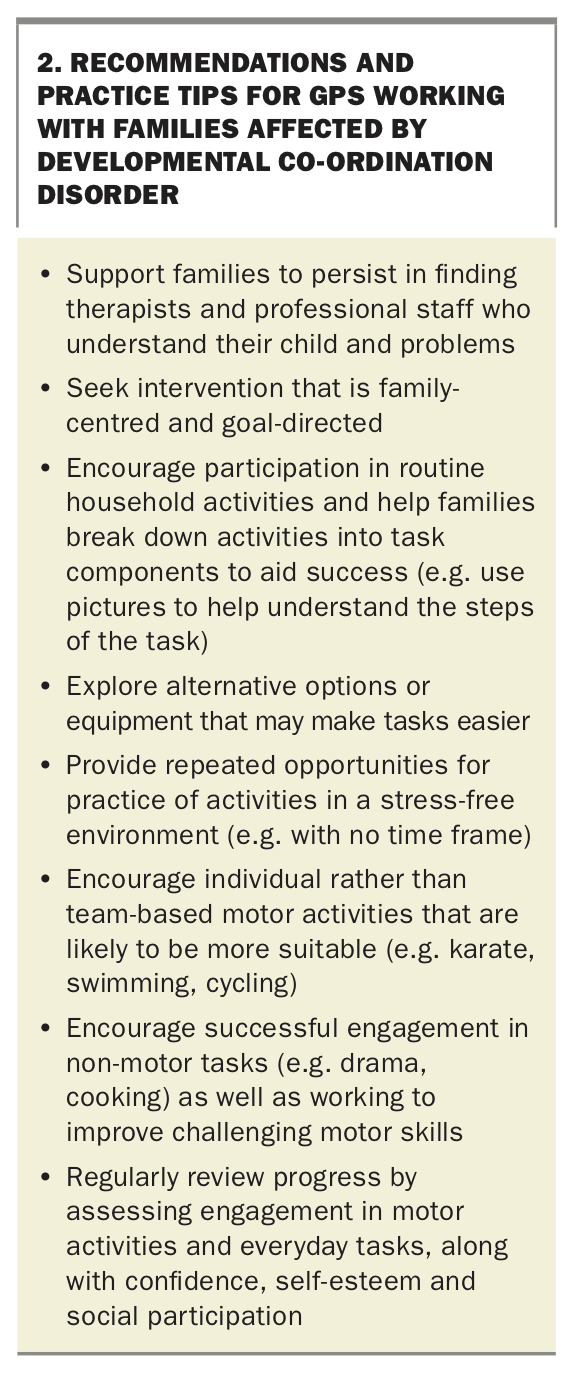
Some recommendations and practice tips for GPs working with families affected by DCD are given in Box 2. Research shows that intervention directed towards performing everyday tasks and social consequences is most beneficial to families and children affected by DCD. Social participation was perceived by parents to be of utmost importance.24 GPs can also help parents to better understand DCD and their child’s problems by directing them to resources such as the information provided on the Australian Parenting website (https://raisingchildren.net.au/guides/a-z-health-reference/development-coordination-disorder-dcd) or an information sheet on occupational therapy for children with DCD (www.schn.health.nsw.gov.au/files/attachments/ot.dcdinfosheet-schn.pdf).
{kind=link}
Conclusion
DCD is a neurodevelopmental disorder that is under-recognised and underdiagnosed. It has a significant impact on children’s participation in everyday activities, social and leisure participation, academic performance and emotional and psychological wellbeing. Without intervention, many difficulties persist into adolescence and adulthood.
Children with DCD present with a range of difficulties, from fine and gross motor problems to learning and academic difficulties. A diagnosis of DCD is typically made after 5 years of age. Primary health care practitioners are best placed to identify and assess motor problems and facilitate referral for appropriate intervention. Research shows that providing targeted, goal-directed intervention is effective and that early intervention will minimise secondary emotional, psychosocial, social and learning difficulties. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.