Urinary tract infection: management in children

Urinary tract infection (UTI) can be the cause of fever in children with nonspecific presentations and constitutes an emergency in very young and unwell children. Starting empirical antibiotic treatment and collecting a ‘clean’ urine specimen for culture are essential considerations. Management of bowel and bladder dysfunction and lifestyle changes are useful adjuncts for preventing recurrent UTIs in children.
Correction
A correction for this article is published in the May 2021 issue of Medicine Today. The online version and the full text PDF of this article (see link above) have been corrected.
- Paediatric urinary tract infection (UTI) can be challenging to diagnose, especially in younger children, in whom symptoms are usually nonspecific.
- Although urine dipstick is a useful screening test, a diagnosis can only be made with a urine culture from an uncontaminated specimen.
- The risk of an underlying renal tract abnormality in children with UTI varies widely with age at presentation and sex.
- Behavioural strategies and management of constipation can be vital in decreasing the risk of recurrent UTI in toilet-trained children.
Urinary tract infection (UTI) is a common childhood infection in Australian children. A Swedish study showed 2% of boys and 8% of girls had at least one UTI by 7 years of age.1 The pretest probability of a UTI varies with patient age, sex and – in males under the age of 1 year – circumcision status. UTI is most prevalent in infants 0 to 3 months of age, with 7.2% of febrile infants in this group having a UTI. In this age group, UTIs are more common in boys than girls (8.5 vs 7.5%), and most common among febrile uncircumcised boys (21%).2 During toddler years, toilet training may lead to an increased incidence of UTI due to poor toileting hygiene, holding and urinary stasis.3 Among adolescents, UTI is more common in girls and risk is increased by sexual activity.2
Despite the high frequency of UTI, only 5% of children with UTIs will be found to have renal scarring, and very few will develop hypertension and end-stage renal disease.4,5 Of children who have a UTI, 20 to 40% have vesicoureteric reflux (VUR); however, UTI risk decreases over time due to improvement or resolution of VUR as the child grows older.6 Discussion of the treatment and prevention of UTIs in children with known underlying urogenital structural abnormalities, neurogenic bladder or renal impairment is outside the scope of this article.
Definitions
UTIs can be classified anatomically into upper or lower tract infections. Clinically these may be determined on presenting symptoms in older children; however, in younger children determining between upper and lower UTI is more difficult due to the nonspecific presenting features. Upper tract UTIs (pyelonephritis) involve the kidneys and ureters and typically present with loin pain as well as systemic symptoms including fever, vomiting and lethargy. Children with bacteriuria and concurrent fever of more than 38°C or loin pain should be considered to have acute pyelonephritis. Children with lower tract infections present with urinary symptoms such as dysuria, frequent urination, urgency and suprapubic pain.
Pathogens
Most UTIs are caused by enteric Gram-negative bacteria, with Escherichia coli being responsible for about 80% of infections.7 Infections with organisms other than E. coli are associated with higher risks of renal scarring and of underlying structural abnormalities of the urinary tract.8,9
The increasing prevalence of multidrug resistant organisms must also be considered. A recent Australian study showed that 11.4% of positive urine cultures in hospitalised children were caused by multiresistant Gram-negative organisms.10 Viral UTIs are uncommon among the paediatric population. Similarly, fungal infections with organisms such as Candida albicans are infrequently seen, but may be precipitated by immune suppression, the use of an indwelling catheter or recent prolonged antibiotic use.
Clinical assessment
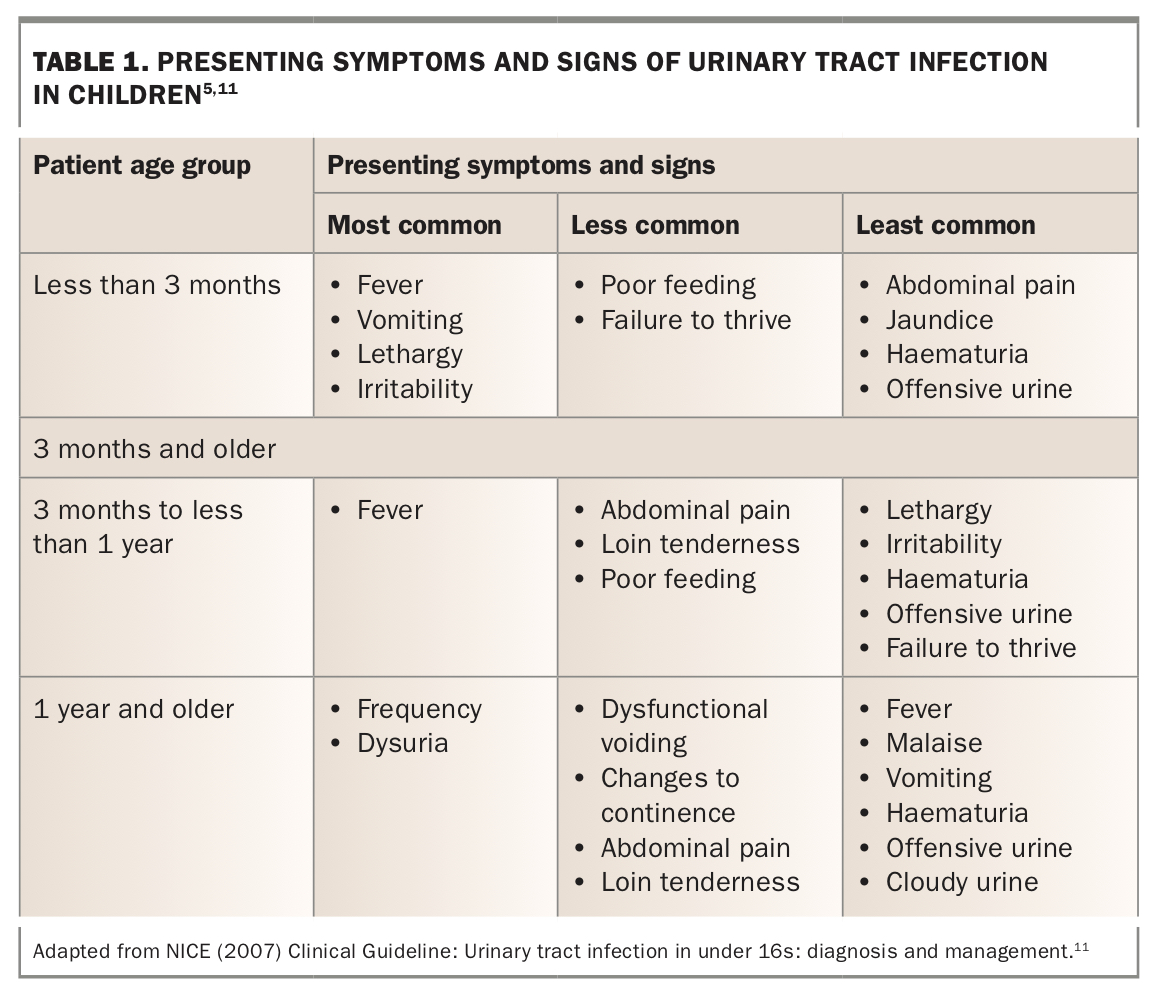
Diagnosis of UTI in children requires a high index of suspicion given the nonspecific nature of presenting symptoms in younger children. The most common presenting symptoms in infants up to 3 months of age are fever, vomiting, lethargy and irritability. Older children may complain of more classic symptoms such as dysuria, frequency and abdominal pain (Table 1).
{kind=link}
Examination
All paediatric patients with fever and/or vomiting should have their hydration status assessed, and febrile infants less than 3 months of age and patients who are in shock should be transferred to emergency care. Across the range of patients, abdominal examination is often normal; however, lower abdominal or loin tenderness may be present.
Investigations
Definitive diagnosis of UTI is made with culture of an appropriately collected urine specimen. A formal urine culture should be done for all children being treated for a presumed UTI. This is important for diagnostic confirmation, identification of the organism responsible for infection and provision of antibiotic sensitivities. In children 3 months and older who have an unexplained fever or UTI-specific symptoms, a presumptive diagnosis of UTI to facilitate timely antibiotic treatment while awaiting culture results can be made by the presence of:11
- both leukocyte esterase and nitrites positive on dipstick testing
- positive leukocyte esterase OR positive nitrites on dipstick testing in children under 3 years
- positive nitrites on dipstick testing in children 3 years or older
- bacteriuria seen on microscopy.
If the above criteria are not met in children who are 3 months or older, urine culture should be sent without commencing antibiotics if:
- leukocyte esterase alone is positive on dipstick testing in children 3 years or older
- recurrent UTI is suspected
- a febrile infection does not respond to treatment within 24 to 48 hours, if no sample has been sent already
- clinical symptoms do not correlate with a dipstick test result.
The finding of isolated pyuria is nonspecific and should be treated with caution as it may indicate other pathology with a similar clinical presentation to UTI, such as appendicitis.
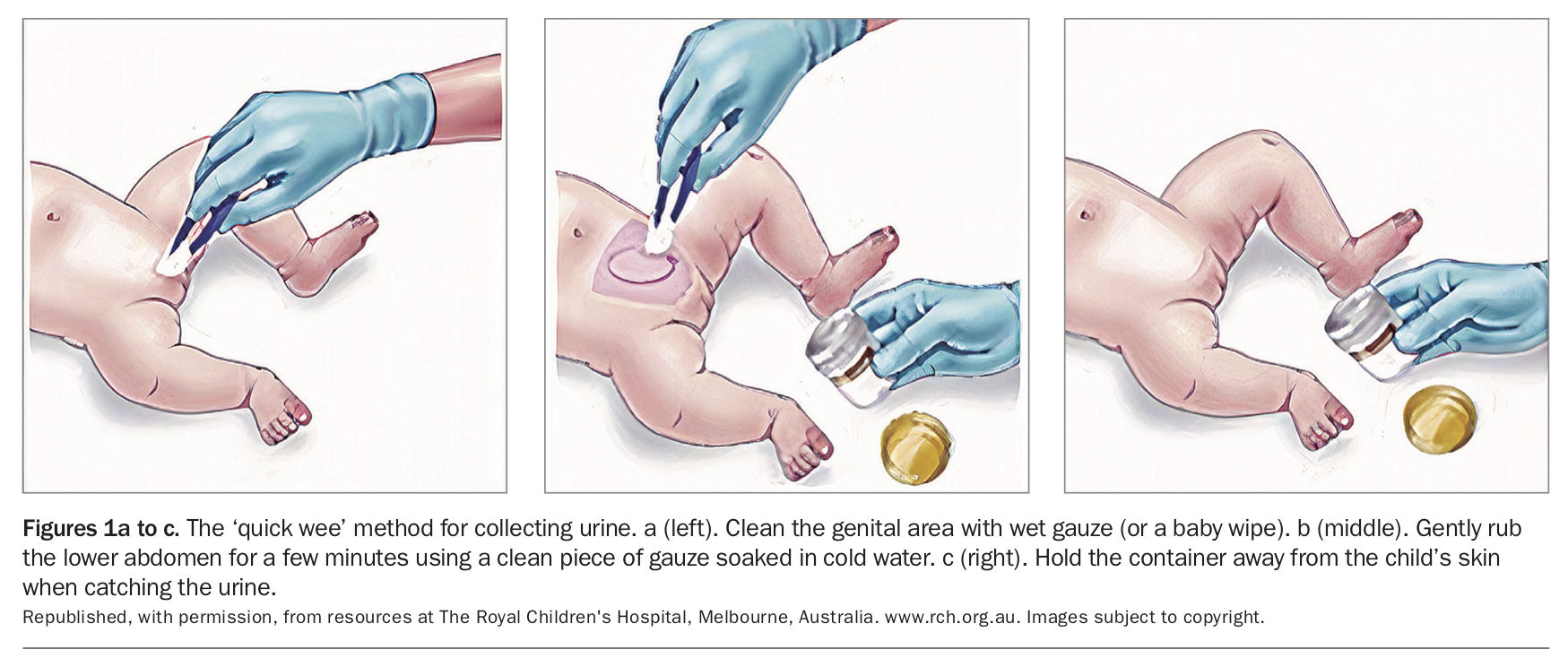
The collection of an adequate urine specimen can be challenging in children who are not yet toilet trained and are therefore unable to provide a midstream urine. Although suprapubic aspirate or in-out catheter specimens are the definitive method of urine collection for culture, they are invasive and best performed when the presence of urine in the bladder can be confirmed either with ultrasound or by delaying the procedure to 1 hour after voiding.12 The use of a clean-catch specimen is an acceptable alternative, but collection of the specimen is difficult for clinicians and parents. Using the ‘quick-wee’ method may encourage the infant to void spontaneously. This is done by using gauze soaked in cold saline to gently stimulate the baby’s suprapubic area and has been shown to increase the speed and success of urine collection compared with waiting for the infant to void spontaneously (Figures 1a to c).13 Urine bag specimens have a high rate of contamination that leads to false-positive results and are not suitable for diagnosing UTI based on culture.
{kind=link}
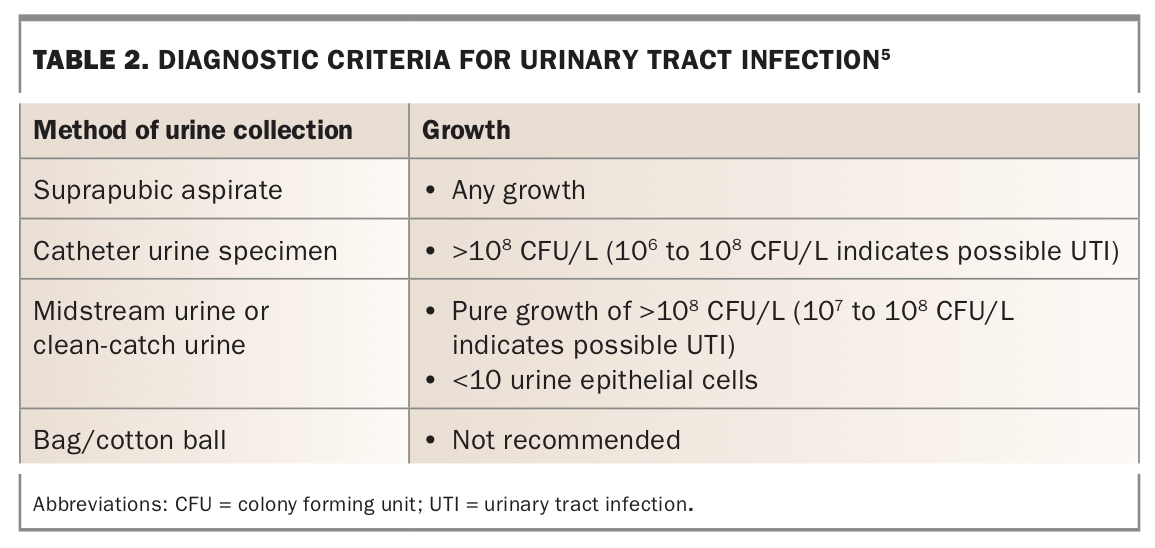
The diagnostic criteria for a UTI are outlined in Table 2. Markers of possible contamination include any growth from a bag or cotton-ball specimen; growth of more than one organism or skin commensals; or a colony forming unit count less than the amount listed in Table 2.
{kind=link}
The role of imaging
Imaging is often, but not always, indicated for children with recurrent UTIs. Increasingly, imaging is avoided for simple first time UTI, due to the time, expense and worry it may cause. Multiple different imaging modalities can be used in the assessment of UTI in children, including ultrasound, micturating cystourethrogram (MCU), dimercaptosuccinic acid (DMSA) and mercaptoacetyltriglycine (MAG3) scans.
Renal ultrasound can assess the structure of the kidneys and urinary tract and identify urinary tract dilatation. It is helpful to obtain pre- and postvoid bladder volumes in older children to assess residual urine volume. We suggest that renal tract ultrasound should be considered in children who:
- have recurrent UTIs
- have not had a second or third trimester ultrasound that has assessed the kidneys and urinary tract
- are less than 3 months of age
- have renal impairment or significant electrolyte derangement
- have a urine culture with atypical organisms (Pseudomonas spp., Staphylococcus aureus)
- do not respond to antibiotics within 48 hours with a sensitive organism
- have an abdominal mass
- have a poor urinary stream.5
VUR is the most common underlying structural abnormality leading to upper tract UTI in children. A normal ultrasound does not exclude VUR, and an MCU should be considered in children with abnormal voiding or in young children with recurrent febrile UTI. MCUs should also be performed in male children who have either bilateral hydroureteronephrosis or bladder wall thickening on ultrasound (to exclude posterior urethral valves). The child should be given prophylactic antibiotics (as per Therapeutic Guidelines: Antibiotic14) around the time of the procedure and an MCU should be delayed until at least two weeks after a UTI. MCUs are usually avoided in children after 5 years of age as they are challenging to perform in older children.
A DMSA scan is a static nuclear medicine test. It is the best test for identifying renal scarring and also provides a measure of the differential contribution to overall renal function for each kidney. DMSA should not be performed within three months of a UTI. DMSA scans are typically considered in the investigation of children with recurrent UTI, a severe episode of pyelonephritis or children with UTI and persistent renal impairment.
A MAG3 scan is a dynamic nuclear medicine test that assesses the uptake and excretion of tracer over time. MAG3 scans are less useful for assessing renal scars but are useful for assessing possible obstruction in the case of hydronephrosis or hydroureter. They also provide an assessment of differential contribution to overall function.
Management
Most children with a UTI can be managed with oral antibiotics and oral rehydration. Neonates and infants less than 3 months of age and children who are moderately to severely dehydrated, in shock or who appear unwell should be referred to hospital for assessment and a full septic screen. Children who have not responded to oral antibiotics, or those who have underlying renal tract abnormalities may require admission for intravenous antibiotics and fluids. An approach to management is summarised in the Flowchart.
Empirical antibiotic therapy
Local guidelines should be used to determine empirical antibiotic treatment, given the heterogeneity in local antimicrobial sensitivities. Suitable initial empirical oral antibiotic choices for children with urinary tract infection include:14
- trimethoprim/sulfamethoxazole 4/20 mg/kg (maximum dose 160/800 mg) 12 hourly
- or trimethoprim 4 mg/kg (maximum dose 150 mg) 12 hourly
- or cefalexin 12.5 mg/kg (maximum dose 500 mg) 6 hourly.
In children with a history of UTI, previous urine culture can also be used to guide empirical treatment.
Children should be reassessed in 24 to 48 hours, sensitivities reviewed, and antibiotics adjusted accordingly. If the child is not improving on appropriate antibiotic therapy, reconsider the diagnosis and/or consider hospital referral for intravenous therapy. If a child is improving clinically despite culture results revealing a resistant organism, antibiotics do not need to be altered. Children with Pseudomonas aeruginosa infection are more likely to have structural renal defects and may require a prolonged course of antibiotics, for which expert advice should be sought.
The most recent National Institute for Health and Care Excellence (NICE) guidelines suggest a three-day course of oral antibiotics is appropriate for children 3 months and older with lower tract UTI, and a longer 7- to 10-day course is required for those with pyelonephritis.15,16 A urine culture does not need to be performed at the end of the treatment course to confirm resolution of the UTI.
Children with dysuria but a normal urine culture result can be challenging to treat. It is wise to collect at least two midstream urine samples if there is a history of recurrent dysuria. In girls, examination of genitalia is important to exclude vulvovaginitis, a common cause of dysuria. Consideration should also be given to sexually transmitted infections in sexually active adolescents.
Management of recurrent UTI
Underlying conditions that promote urinary stasis such as structural urogenital abnormalities, neurogenic bladder, constipation and behavioural holding can also increase the risk of UTI and should be considered, particularly in children who present with their first UTI after toilet training.17 There are conflicting reports as to whether earlier initiation of toilet training is helpful in reducing the risk of UTI.18,19
Constipation is prevalent in the paediatric population and is well established as a leading risk factor for dysfunctional voiding and recurrent UTI.20 Rectal distension from faecal loading compresses the adjacent bladder outlet leading to incomplete voiding. It is vital to seek a history of constipation and bowel or bladder dysfunction. When appropriate, treatment can be initiated with dietary education and stool softeners.
Other voiding and lifestyle interventions that can be undertaken by the parent and child to reduce the risk of recurrent UTI include:
- adequate water intake of about four cups per day for toddlers, five to six cups for primary-school aged children and six to eight cups for teenagers
- regular toileting every two to three hours (it is important to request teacher involvement in this for school-aged children)
- double toileting (after the child finishes voiding, they stand up then sit back down and try to void again) to reduce the risk of a residual volume
- wiping front to back.
If available, a skilled physiotherapist can greatly assist in assessment and treatment. A specialised physiotherapist can perform uroflowmetry, which assesses voided volume and flow pattern during a void and postvoid residual volume. Interventions include age-appropriate anatomy education, help on correct toilet positioning and timed voiding programs. Continence physiotherapists can be accessed through hospitals or community paediatric continence clinics.
Antibiotic prophylaxis is not routinely recommended in children after the first UTI but should be considered in children with recurrent UTI and/or grade 3 to 5 VUR, and young infants after a severe first UTI.5 Circumcision may benefit boys in the first year of life who have recurrent UTI or high-grade VUR. Among children without renal tract abnormalities, 111 circumcisions would be required to prevent one UTI; however, this reduces to 11 in boys with recurrent UTI, and four with high-grade VUR.21 Cranberry juice and probiotics have not been shown to be of benefit in children with UTI.22,23
Criteria for referral to tertiary paediatric services
Refer to urgent specialist paediatric care for:
- infants less than 3 months with fever
- children who are seriously ill, dehydrated or in shock
- children with serum creatinine level above the reference range
- children with a palpable bladder or abdominal mass.
There is a degree of overlap between paediatric nephrology and urology services with regard to structural renal tract abnormalities. Consider direct referral to a paediatric urologist for children with significant renal pelvic dilatation (>15 mm or >10 mm bilateral) or possible renal tract obstruction. Consider direct referral to a paediatric nephrologist or general paediatrician for children with recurrent UTI, renal impairment or renal dysplasia or parenchymal defects.
Conclusion
Urinary tract infections are common in the paediatric population but prevalence and presentation vary widely with age. It is important to consider UTI as a cause of fever in younger children and infants with nonspecific presentations. Timely antibiotic treatment aims to prevent long-term renal scarring. Although a urine dipstick is a useful tool for facilitating early identification of children who need antibiotics, an appropriately collected urine culture is essential for diagnosis. Management of bowel and bladder dysfunction and lifestyle changes are useful adjuncts for preventing recurrent UTIs in children. MT
Further reading
Guidelines
Kidney Health Australia. Diagnosis and treatment of urinary tract infection in children. https://cariguidelines.org/guidelines/chronic-kidney-disease/diagnosis-treatment-of-urinary-tract-infection-in-children
The Royal Children’s Hospital Melbourne. Urinary tract infection. https://rch.org.au/clinicalguide/guideline_index/Urinary_Tract_Infection_Guideline
Information for parents
The Royal Children’s Hospital Melbourne. Urinary tract infection (UTI). https://rch.org.au/kidsinfo/fact_sheets/Urinary_tract_infection_UTI
The Royal Children’s Hospital Melbourne. Urine samples. https://rch.org.au/kidsinfo/fact_sheets/Urine_samples
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.