Lesbian, bisexual and queer women’s health: a guide for GPs

Gay, lesbian and transgender health
GPs can offer inclusive primary health care for lesbian, bisexual and queer women through affirming their sexual identity and understanding their specific biological and socially determined health issues, and by providing targeted referrals.
- GPs can provide effective primary health care to lesbian, bisexual and queer (LBQ) women related to their biological needs, including sexual health, contraception and achieving pregnancy.
- Negative social attitudes towards LBQ women can result in discrimination, abuse, violence and marginalisation.
- GPs should recognise discrimination as a risk factor for high levels of depression, anxiety, suicidal thoughts and substance use among LBQ women.
- Disability, ethnic minority and Aboriginal and/or Torres Strait Islander status can exacerbate existing health inequalities in LBQ women.
- Roles for GPs include referral to LBQ-inclusive services and peer support, and advocacy.
Lesbian, bisexual and queer (LBQ) women have specific health issues that require informed and sensitive care. These health issues can be categorised as either biologically determined or socially determined (Box 1). Biologically determined issues arise from health needs for women who partner or have sex with women, or gender diverse individuals. Socially determined issues arise in the face of negative attitudes. These do not differ from those of heterosexual women in the absence of marginalisation, discrimination or abuse. There are also intersectional issues where LBQ women have other minority or marginalised identities such as disability, ethnic minority or Aboriginal and/or Torres Strait Islander status. Each of these specific issues may need appropriate knowledge, skills and attitudes that are affirming and aware of the intersectionality.
{kind=link}
Biologically determined health issues
Sexual health
The sexual lives of LBQ women are diverse and fluid, with movement between identities, attractions and behaviours being common (Box 2). Women may have female partners (and may or may not identify as lesbian), partners of both binary genders (and may identify as bisexual), have partners or attractions to gender diverse people (pansexual) or be polyamorous. A disproportionate number of sex workers are LBQ women, and although many are empowered women working in legalised brothels, some are street workers and at risk of violence and coercion. Contraception is needed for some LBQ women, including for those who have sex with men or with gender diverse or transgender people who were assigned male at birth. Young LBQ women are more likely than their heterosexual peers to have an unintended pregnancy, and this is largely due to contraception messaging being targeted to heterosexual people.1
{kind=link}
There is a commonly held myth that women who have sex with women (WSW) are not at risk for sexually transmitted infections (STIs). However, this is incorrect. The Second Australian Study of Health and Relationships found that of the female participants aged between 16 and 69 years, 18.4% of lesbians, 20.4% of heterosexuals and 27.7% of bisexuals had ever been diagnosed with an STI; and 2.8%, 2.7% and 7.3% respectively had had an STI in the past year.2
The most common STIs found in WSW are bacterial vaginosis (BV), herpes simplex, vaginal candida and human papillomavirus. Concordance rates of BV between lesbian couples are as high as 80% (both positive or both negative), and this becomes important in the face of recurrent BV (which can be difficult to treat) or when planning pregnancy or gynaecological procedures.3 Bacterial vaginosis in WSW is associated with a greater number of female partners, a female partner with BV symptoms and smoking.4 Current advice is to offer testing and treatment for a female partner of a woman with BV.
Equally, WSW should be offered cervical screening. They are now a specific target group for the national cervical screening program, given evidence that some subgroups of LBQ women are under-screened.5 Safer sex for WSW relates largely to preventing transmission of vaginal secretions between vaginas by using different fingers or toys in different sites and reducing or protecting sexual contact at times of an herpes simplex outbreak.
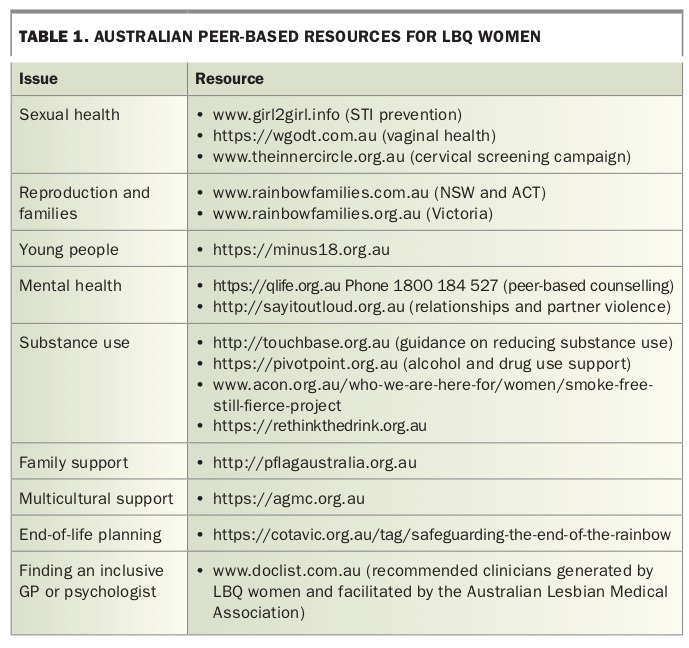
Resources for LBQ women on sexual health are listed in Table 1.
{kind=link}
Reproduction and parenting
Single and coupled LBQ women have been forming families for decades. The increasingly diverse methods of family formation include home insemination with a known donor, clinic-based insemination or in vitro fertilisation with a known or clinic recruited donor, using a partner’s egg and donor sperm to conceive, and parenting through adoption or fostering.6 Most states and territories in Australia legally allow LBQ women to access assisted reproductive technology services and adoption. Despite this access, many LBQ women prefer to have known sperm donors and inseminate at home. This enables more autonomy in conception, and involvement of the donor in the child’s life. The role for the GP in issues around reproduction includes educating women about fertile times in their cycle for insemination, and optimising safety by advising on the appropriate STI and genetic testing for the donor.
Parenting issues can also arise related to preventing social stigma and encouraging resilience in the children. However, parents can be reassured that the social, physical and mental health outcomes for children of same-sex parented families are the same as for children in any family.7
Resources for LBQ women on reproduction and families are provided in Table 1.
Socially determined health issues
Identity formation and coming out
Social attitudes regarding minority sexual orientation have a huge role to play in the health and wellbeing of LBQ women. This starts during sexual identity formation (usually around puberty) and can progress through the life stages. Although attitudes have dramatically improved over the past few years, there are still regions and cultural subgroups in which homophobia, biphobia and transphobia are prevalent.
For LBQ young people, the role of families of origin is critical to their mental health and resilience during the period of identity formation. For example, in a recent US study of 843 LBQ women between 18 and 25 years of age, up to 41% had experienced rejection from their families after coming out, and for many this had affected their self-esteem and community connection.8 Analysis of the US National Longitudinal Study of Adolescent Health showed that lesbian and bisexual young women reported lower levels of parental support than heterosexual women, and that this correlated with higher levels of depression and suicidality.9
LBQ young people from socially conservative communities can internalise the negative messaging and regard themselves as abnormal or morally corrupt. Conversely, family support builds resilience, self-esteem and wellbeing for LBQ young people.10
Affirmation of emerging minority sexual identities by a health professional can be important during the coming out period. This can include assisting the young person to find like-minded peers and supportive adults through either school or community networks.
Resources on family and multicultural support and LBQ young people are listed in Table 1.
Mental health
LBQ women are at least twice as likely as heterosexual women of any age to experience depression, anxiety and suicidal ideation. This has been related to ‘minority stress’, which is the day-to-day reality or potential of experiencing negative attitudes and threats.11 It can also involve a greater likelihood of abuse and violence from strangers and within families and intimate relationships, again at least twice as high as heterosexual women.12 Intimate partner violence (IPV) is at least as likely among female couples as heterosexual couples, and may even be higher. In the US National Violence Against Women Survey, all types of IPV were twice as likely among the lesbian and bisexual women as among the heterosexual women.13 Issues associated with IPV for same-sex couples include a family history of violence, past IPV, fusion (where the couple have few social outlets as individuals) and alcohol intake.14 Unfortunately IPV services tend to be gendered so it can be difficult for female perpetrators to seek help, and fear of discrimination in services can be a barrier to help-seeking for victims.15
The recent Australian same-sex marriage plebiscite has enabled comparison of the Household, Income and Labour Dynamics in Australia Survey data between areas with predominant ‘yes’ and ‘no’ votes. It supported the minority stress theory, finding that lesbian, gay and bisexual people living in ‘no’ areas were significantly more likely to have worse life satisfaction and worse mental health.16 Marginalisation can also be a factor, in that LBQ women might be excluded from social networks. This can be especially the case for bisexual women, or those with a disability or cultural minority identity. Another pressing issue is the ongoing use of ‘gay conversion therapy’ in Australia (generally under the guise of religious instruction or support), which can be extremely damaging.17
For LBQ women presenting with mental health issues, GPs should explore the possibility of triggers including abuse, violence or marginalisation arising from sexual identity-based discrimination. This is essential to enabling appropriate management, including referral to LBQ-inclusive and knowledgeable counsellors (Table 1). Peer support and social connection is also important to building resilience and recovery for many LBQ women. Excellent national LGBTIQ peer support is available through the QLife program, which trains and maintains peer support workers in each state and territory for phone or online counselling (Table 1).
Substance use
LBQ women are two to three times more likely than heterosexual women to drink alcohol at harmful levels, to smoke and to use illicit drugs.18,19 There are complex reasons for higher levels of use and misuse. First, substances can be used as self-medication in the face of minority stress; second, many LBQ women use substances as part of socialising with LGBTIQ communities (often in pubs, bars and clubs); and third, some LBQ women use substances as an integral part of their sexual or gender identity.20 These intersecting associations with substance use require complex interventions and targeted health promotion (Table 1).
Ageing
Issues facing older LBQ women include isolation, a history of trauma, fear of homophobia when engaging with aged care services and difficulties with end-of-life planning.21 GPs have a role in advocating for the needs of older LBQ women through understanding whether they are partnered, who their chosen family is, how they want to engage with aged care services and finding appropriately trained providers. LGBTIQ-inclusive training in aged care services has been occurring nationally since the groundbreaking National LGBTI Ageing and Aged Care Strategy was released in 2013.22 There is also a new resource to support end-of-life planning that includes information about legislative protections (Table 1).
Minority intersection health issues
Subgroups of LBQ women that are even more disadvantaged include those with disabilities, those who identify as Aboriginal and/or Torres Strait Islander, refugee and asylum seekers, and those from minority ethnic or religious groups. The influence of multiple marginalised identities on health and wellbeing includes experiences of rejection or trauma, questioning the legitimacy of their sexual minority identities, and lack of social connection through not feeling included by any community.23
LBQ women living with a disability may be reliant on personal carers who prevent their access to the LGBTIQ community or discourage sexual expression. Homelessness is another under-recognised issue, with LGBTIQ people being over-represented among Australian homelessness populations. This particularly relates to family rejection for young people, and discrimination and violence in the private rental, social and crisis housing sectors.24 There are increasing numbers of LBQ refugees and asylum seekers in Australia who are fleeing persecution based on their sexual orientation or gender identity. They face major challenges proving their refugee status because they invariably had to hide their sexual orientation in their country of origin, and may be vilified by their cultural community in Australia.
The role of the GP
Although LBQ women are likely to have a regular GP, they are less satisfied with the care they receive than heterosexual women.25 Low satisfaction is often related to inadequate specific provider knowledge, as well as concerns regarding heterosexism (assumptions of heterosexuality) or negative attitudes. Satisfaction is associated with disclosure of sexual orientation when disclosure is met with affirming attitudes, and disclosure can result in more comprehensive, high quality primary health care.26
GPs have important roles to play above and beyond standard health care for LBQ women. First and foremost is affirmation of a woman’s sexual identity and openly displaying respect for diversity. This will overcome some of the fear that many LBQ women bring to the encounter and will encourage disclosure of other stigmatised issues (e.g. sexual abuse, intimate partner violence, substance use, homelessness, social exclusion). Recognising the role of discrimination in LBQ women’s health is critical, as is understanding their preferences for referral (mainstream or LGB-specific services).
Health promotion is important in specific areas that are often deferred by LBQ women (including cervical and breast screening). Engaging with family formation planning and helping women to build resilience to LBQ-specific stressors is also positive. Advocacy regarding legal issues can be helpful, including understanding who is the nominated next-of-kin and who are in the woman’s chosen family. Further, encouraging women to have a medical power of attorney and an advance care plan can clarify medical decision making when needed.
Various guidelines and training packages on LBQ women’s health are available for GPs in need of more detailed upskilling. The Rainbow Tick accreditation guidelines have been developed by Rainbow Health Victoria (formerly Gay and Lesbian Health Victoria) at La Trobe University, and provide important whole-of-system approaches for inclusive care. GP resources are shown in Table 2.
{kind=link}
Conclusion
The health and wellbeing of LBQ women can be enhanced and maintained if they have a respectful and inclusive GP who is willing to delve a little deeper into understanding the full context of their lives. LBQ women will appreciate and welcome this approach. MT