Monkeypox – what GPs need to know
Monkeypox was identified in Australia for the first time in 2022, with a rising number of cases and human-to-human transmission occurring globally. A heightened awareness of the risk factors for and clinical manifestations and management of monkeypox will ensure a timely and co-ordinated response to help prevent further outbreaks.
Monkeypox is a zoonotic disease transmitted from rodents and primates to humans. Although outbreaks in humans have occurred in the past, these have been largely confined to endemic areas of the Congo Basin and West Africa, and the result of animal-to-human contact. Human cases of monkeypox have been identified in Australia for the first time in 2022, with human-to-human transmission increasing globally. GPs should be aware of the typical presentation of monkeypox, those and are at high risk of contracting the virus who may benefit from available vaccines and management options for patients with monkeypox.
History and epidemiology
Monkeypox virus is a double-stranded DNA virus within the orthopoxvirus genus. It is a close relative of the virus that causes smallpox, which was the first human disease to be eradicated by vaccination, in 1979. It is a large brick-shaped, enveloped virus measuring 200 to 250 nm.1
The monkeypox virus was identified in a Danish laboratory in 1958.2 The infection was first discovered in captive monkeys but was recognised as a human zoonosis in 1970.3 Until the 21st century, monkeypox was confined to the tropical rainforests of the Congo Basin and West Africa. A total of 13 outbreaks in endemic countries, each of 11 or less cases, were reported between 1970 to 2003.1 In 2003, the first outbreak occurred outside Africa after a shipment containing infected rodents was imported from Ghana to the USA. Further infection occurred in American native prairie dogs, resulting in more than 70 human cases.4 An outbreak of 19 identified cases occurred in Sudan in 2005, and further intermittent outbreaks within the Congo Basin and West Africa, along with imported cases to Israel, the UK, Singapore, and the USA had been reported this year, with the largest outbreak of over 200 confirmed cases occurring in Nigeria in 2017.4 Cases within Africa have been increasing in urban areas, along with an increased proportion of cases being from human-human transmission events.5
Recently, the WHO convened a meeting to align monkeypox nomenclature to best current practice. An open forum is also underway to assign a new disease name to monkeypox.6 Traditionally, monkeypox was divided into two clades based on geography, with renaming based on Roman numerals. Consensus is to now refer to the former Congo Basin (Central African) clade as Clade I and the former West African clade as Clade II. Additionally, Clade II consists of two subclades (Clade IIa and Clade IIb), with IIb referring to the group of variants circulating in the current global outbreak.6 Historically, Clade I has been more virulent and transmissible than Clade II.7
Life cycle and transmission
Monkeypox virus has sustained transmission within various animal hosts in endemic regions, meaning that eradication of the disease is not feasible.8 Until now, there has been limited human-to-human transmission, with only sporadic spill-over events into the human population. The natural host of the monkeypox virus is largely undefined, but the Gambian pouched rat and rope squirrel are the most likely candidates, with many other species likely susceptible to infection.2 Sooty mangabeys and other primates can also act as reservoirs.
In the 2003 US outbreak, prairie dogs were noted to be amplifying hosts, infecting many of the human cases. Further, monkeypox virus was detected in prairie dog lung tissue, indicating infection via large respiratory droplets.9 Other modes of transmission include direct contact with infected animals and fomites, and consuming infected meats. Usually, animal-to-human and human-to-human transmission requires relatively close contact with blood or bodily fluids, including respiratory secretions or fluid from skin lesions. Before the current outbreak, almost all cases of monkeypox in people outside Africa were linked to travel to endemic countries.
Current global situation
The current outbreak started in Europe in May 2022, with the WHO declaring the global monkeypox outbreak a ‘public health emergency of international concern’ on 23 July, 2022.10 As of 7 September, 2022, over 52,000 cases across 102 countries and territories have been reported globally, with most cases occurring in Europe and the USA.11,12
Current situation in Australia
Before May 2022, cases of monkeypox had not been identified in Australia. On 28 July, 2022, Australia’s Chief Medical Officer declared monkeypox a communicable disease incident of national significance.13 As of 1 September, 124 cases of confirmed or probable monkeypox have been reported to the National Notifiable Diseases Surveillance System in Australia (64 in Victoria, 48 in New South Wales, five in Western Australia, three in Queensland, two in the Australian Capital Territory and two in South Australia).14 Although most cases were acquired overseas, a small proportion were acquired within Australia.
State health departments are working together to identify cases in a timely manner and undertake contact tracing to detect further cases as part of a national public health response. Treatment and vaccine guidelines are under review.15 The Communicable Diseases Network Australia (CDNA) and the Australian Health Protection Principal Committee have ongoing oversight over the public health response to the outbreak in Australia. The CDNA had developed national guidelines, which are available online (www.health.gov.au/resources/publications/monkeypox-virus-infection-cdna-national-guidelines-for-public-health-units).
Why have cases increased?
Over the past 30 years, the number of monkeypox cases has been rising, with an increasing proportion caused by human-to-human transmission.16 The ongoing sporadic outbreaks around the world are suspected to be related to the eradication of smallpox and the cessation of mass vaccination campaigns, which provided up to 85% protection against monkeypox.17 Other factors, such as population growth, climate change, urban expansion, deforestation, proximity to infected animals, international travel and evolutionary changes in the virus, may also be contributing to increased transmission and case numbers.18,19 The current global outbreak has seen a change in the traditional modes of transmission, with increased human-to-human transmission events a key factor in the widespread dissemination of the disease. Genomic studies show that the current global outbreak is caused by Clade IIb viruses and investigations are underway to further understand the current change in epidemiology and pattern of transmission.20
Preventing the impact
Several measures can help reduce the risk of infection with monkeypox virus. Healthcare workers should use appropriate personal protective equipment and precautions when in contact with people with suspected or confirmed infection, including wearing a fit-tested particulate respirator or P2/N95 mask during tasks such as showering patients or aerosol-generating procedures.21 Hospitalised patients should be managed under droplet and contact precautions.
Infected patients should remain in isolation at home, away from other household members, until all lesions have crusted, scabs have fallen off and fresh skin has formed beneath, and only leave to seek medical attention or as directed by public health advice. Household members should practice good hand hygiene and avoid contact with the infected individual and any items that person may have come into contact with, including linen, towels and clothing. The usual duration of isolation is two to four weeks. Laboratories should be informed in advance of the arrival of any samples from suspected or confirmed cases, so that appropriate precautions can be implemented.
Vaccines available for monkeypox
Vaccines against smallpox can be used pre- and postexposure and are highly likely to be effective in preventing monkeypox and reducing disease severity; however, further study is needed. Vaccination before exposure is recommended for optimal protection. Postexposure vaccination should ideally be given within the first four days after exposure but vaccination up to 14 days after exposure is thought to reduce severity of illness.22
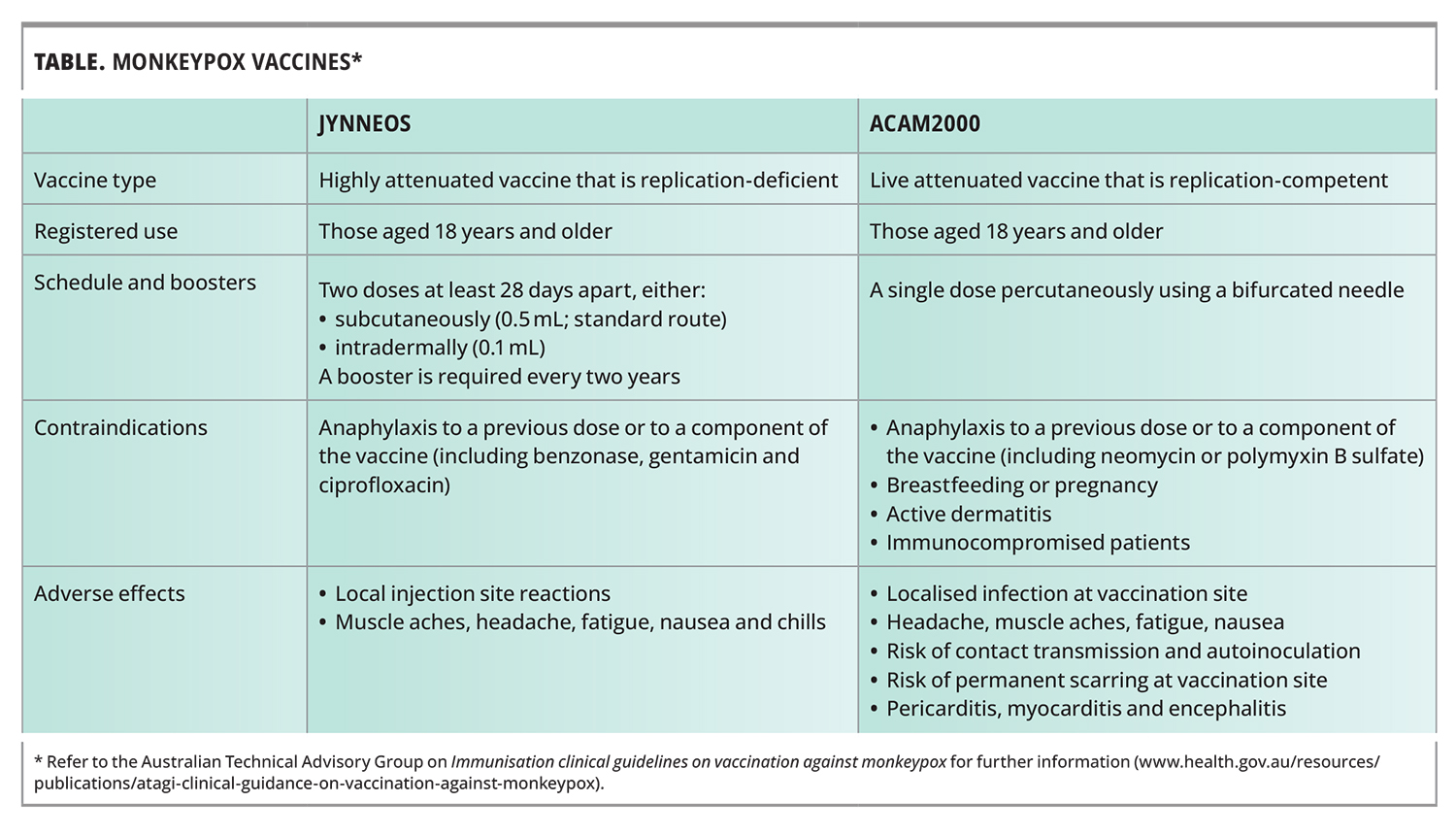
Two smallpox vaccines are currently available for the prevention of monkeypox: the third-generation JYNNEOS vaccine and second-generation ACAM2000 vaccine (Table). The JYNNEOS vaccine contains the modified vaccinia virus Ankara – Bavarian Nordic. This is a live virus that does not replicate in human tissue. Two doses are given subcutaneously four weeks apart, with peak protection occurring two weeks after the second dose; a booster is required every two years. JYNNEOS is the preferred vaccine for use in Australia because it is easier to administer, has a safer side-effect profile and can be used in immunocompromised individuals.22,23 The global supply of JYNNEOS is currently limited; therefore, vaccination is only recommended for high-risk groups.
{kind=link}
The ACAM2000 vaccine contains a clone of first-generation smallpox virus strains cultured on tissue. It is a single-dose live-attenuated vaccine that requires specialised training to administer via percutaneous scarification using a bifurcated needle. This results in a localised infection at the vaccination site and patients should be advised of appropriate wound care and the risk of permanent scarring. The vaccine should not be administered to patients who are severely immunocompromised, have active atopic dermatitis or are pregnant. It provides peak protection within 28 days and requires a booster every three years.
Who is at risk?
A recent global case series of 528 patients showed that 95% of transmission events occurred via sexual activity. The average age of patients was 38 years, with 98% of patients being gay or bisexual men. Of those, 41% were living with HIV infection, mostly well controlled.24 Monkeypox virus has been detected directly from seminal fluid, respiratory droplets, and skin lesions.24 Close contact during sexual activity contributes to the ongoing circulation of the virus. Based on these data, groups who are at high risk of contracting monkeypox and should be recommended for vaccination, including postexposure prophylaxis, include:
- men who have sex with men, including those living with HIV or taking HIV pre-exposure prophylaxis, those with a recent history of multiple sexual partners, participating in group sex or who attend sex on premises venues and those with recent sexually transmitted infections
- sex workers
- immunisation providers administering second-generation ACAM2000 vaccine
- anyone in the above risk categories who is planning travel to a country experiencing a significant monkeypox outbreak, with vaccination recommended four to six weeks before departure.23
Clinical manifestations
Patients in the current outbreak of monkeypox differ from historic sporadic monkeypox cases in Africa, which presented with many widespread lesions and had a mortality rate of up to 10%. Many of these cases were likely caused by Clade I monkeypox, unlike the current outbreak. Although current cases still have both cutaneous and systemic manifestations, the number of skin lesions is a less prominent manifestation and the symptoms less severe.
The incubation period of monkeypox is usually between six to 13 days but can range from five to 21 days.4 Systemic symptoms may begin as a prodrome before the skin lesions appear and typically manifest with lymphadenopathy, fevers, fatigue and malaise. Lymphadenopathy (mostly inguinal) is common, occurring in 56% of individuals in one case series, and is one of the distinguishing features from smallpox.25 These systemic symptoms can also occur after the appearance of skin lesions.
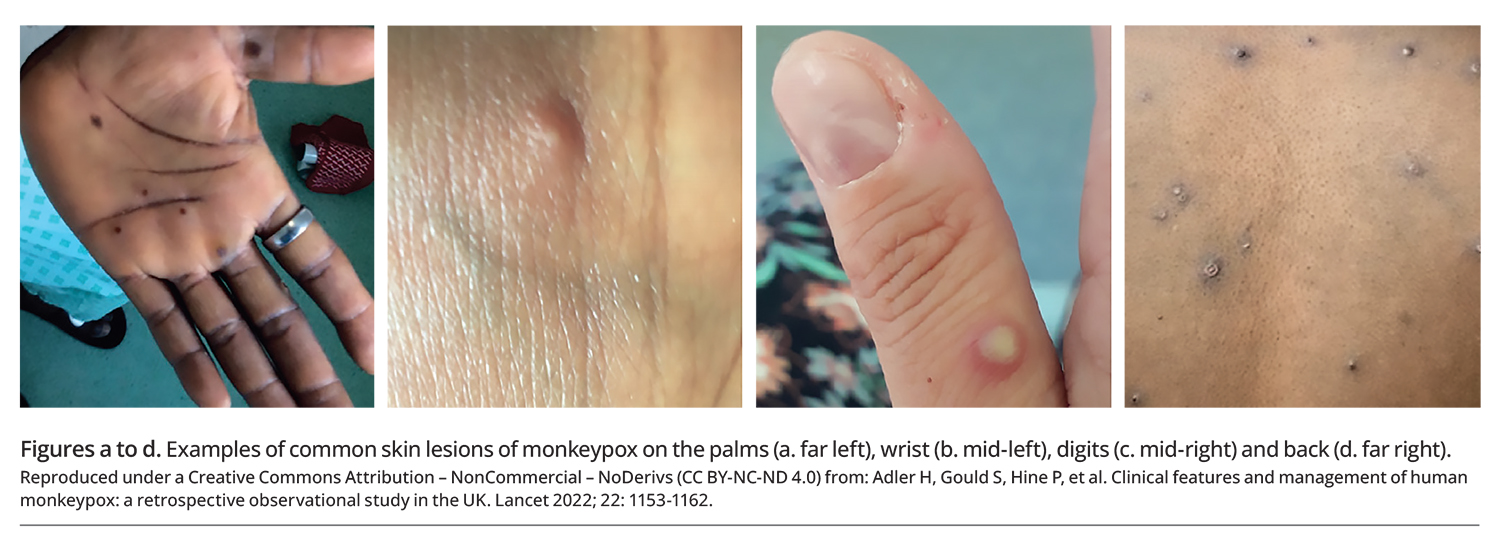
Skin lesions occur in 95% of patients, with the anogenital area being the most commonly affected site, followed by the trunk and limbs (Figures a to d). The face, palms and soles can also be affected.24 The dermatological manifestations most often present with a vesiculo papular rash but a macular rash, single or multiple ulcers, an eschar or crusted lesions can also occur.24,25 Multiple skin lesions with these varying appearances can present simultaneously. Oropharyngeal symptoms have also been reported and include pharyngitis, tonsillitis, odynophagia, epiglottitis and oral lesions.
{kind=link}
Types of sexual practice has been shown to correlate with disease presentation. For example, people who have receptive anal intercourse are more likely to develop proctitis and systemic symptoms, whereas those who have receptive oral sex have high rates of ulcerative tonsillitis.26 Immunocompromised people, including those living with HIV and with a CD4 count of less than 0.2 x 109 cells/L) may be at higher risk of developing severe disease.
Secondary bacterial infection and cellulitis can occur around the skin lesions and are common in skin lesions on the penis.25 Rare complications include pneumonitis, encephalitis, myocarditis and keratitis, which can lead to vision loss.24
Diagnosis
Skin lesions should be vigorously swabbed using flocked swabs. Two swabs should be taken for separate monkeypox PCR and viral testing. Ideally, two to three lesions from different locations or with different appearances should be sampled. New flocked swabs should be used to collect oropharyngeal swabs or, for patients with proctitis, rectal swabs.
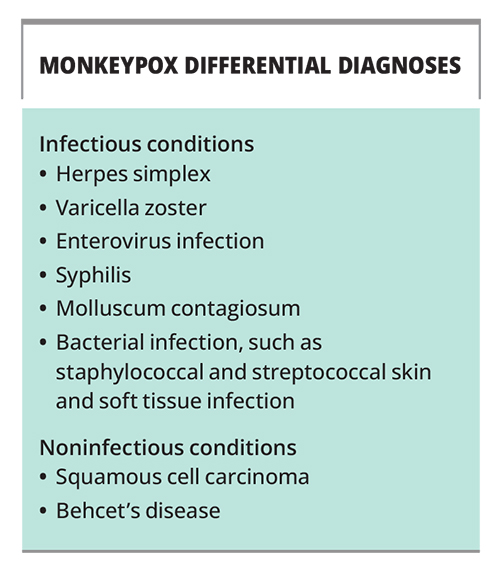
Each specimen should be first placed in a separate biohazard sample bag, and then all the sample bags should be put into a second outer biohazard specimen bag, along with the request form. A monkeypox PCR test should be requested, along with tests for the common differential diagnoses (Box). Noninfective causes, such as squamous cell carcinoma or Behcet’s disease, should also be considered. If bacterial infection is suspected, a separate swab should be used to send tissue from the skin lesion for microscopy, culture and sensitivity testing.
{kind=link}
Management
The initial assessment of anyone presenting with a new skin lesion with or without systemic symptoms should include a detailed sexual and travel history to assess their epidemiological risk. Examination should include an external genital and anorectal examination, given the high frequency of skin lesions in this area, with relevant swabs taken as detailed above. Public health authorities should be notified of any suspected or confirmed cases.
Most cases of monkeypox are self-limiting and patients can be managed in the outpatient setting. For patients with severe disease or in those at risk of severe disease (e.g. immunocompromised patients), antiviral therapy can be considered; however, this should only be given in consultation with an infectious diseases or sexual health physician. The preferred antiviral is tecovirimat for 14 days, which has been previously used for smallpox. It can be given orally or intravenously and dosing is weight-based. Studies on the safety and effectiveness of tecovirimat for monkeypox are currently being undertaken; however, at the time of writing, no data are available. Vaccinia immunoglobulin may also be considered to treat monkeypox and is the preferred option for complications after ACAM2000 vaccination. The use of cidofovir is also being investigated.27
Occasionally, patients with severe rectal pain secondary to proctitis require hospital admission for symptom management. Severe proctitis can make defaecation difficult and local anaesthetic gel, stool softeners and analgesia may be needed. Oropharyngeal lesions can also be painful, making oral intake difficult, and affected patients may require rehydration or nutritional support.
People with confirmed monkeypox should isolate at home until all their skin lesions have crusted over, scabs have been shed and a new skin layer has formed. The duration monkeypox virus remains in semen and the infectiousness of viral shedding in semen is currently unclear. It is therefore recommended that people with monkeypox abstain from sex for the duration of their infection and use condoms when engaging in sexual activity for an additional eight weeks after they have recovered.24 Treatment guidelines are available online (https://www.health.gov.au/resources/publications/monkeypox-treatment-guidelines).
When to refer
GPs should alert their local public health unit of any patient suspected of having monkeypox before sending a tissue sample for diagnosis. Infectious diseases and public health authorities should be notified of any confirmed cases to ensure a timely co-ordinated response in regards to isolation, contact tracing and symptom management.
Conclusion
The current global outbreak of monkeypox has been associated with usually mild, self-limiting symptoms; however, the systemic and cutaneous manifestations can be variable. Returned travellers and men who have sex with men and with multiple sexual partners are most at risk. Healthcare practitioners need to have a heightened awareness of patients with these epidemiological risk factors who present with new skin lesions, and consider monkeypox as a differential diagnosis. Local public health units should be contacted about any confirmed or suspected cases. MT
COMPETING INTERESTS: None.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.