Transgender and gender diverse patients – providing holistic care in general practice

Gay, lesbian and transgender health
Historically, the medical needs of people who identify as transgender or gender diverse have not been well covered in medical training curricula. Despite this gap in formal training, GPs can make a significant difference to the lives of their transgender and gender diverse patients.
- ‘Transgender’ and ‘gender diverse’ are umbrella terms for people who identify with a gender that differs from their assigned sex at birth.
- The number of people who openly identify as transgender or gender diverse is increasing.
- People who are transgender or gender diverse face barriers in accessing healthcare services.
- GPs can provide safe and inclusive services for people who identify as transgender or gender diverse, as well as their families.
- GPs can maintain their patients’ gender-affirming hormone therapy.
GPs are well placed to provide holistic and affirming health care to their patients who identify as transgender or gender diverse. Clinics that provide inclusive and supportive spaces are empowering for staff and can be remedial for all patients. This article aims to provide some basic and practical information to assist GPs in providing safe, inclusive and holistic care to their patients who identify as transgender or gender diverse.
What do the terms transgender and gender diverse mean?
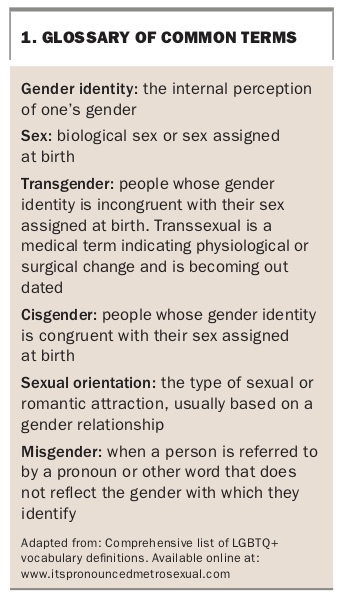
‘Transgender’ and ‘gender diverse’ are umbrella terms for people who identify with a gender that differs from their sex assigned at birth. Although some people use these terms interchangeably, ‘gender diverse’ usually includes people whose gender identity is in between the binary of male and female. People may identify as ‘genderqueer’, ‘nonbinary’, ‘gender nonconforming’, ‘pangender’, ‘gender fluid’ or ‘agender’. Some people identify only as ‘male’ or ‘female’ and do not use any additional labels, such as ‘trans male’ or ‘trans female’. A glossary of common terms is listed in Box 1.
{kind=link}
Although there are no definitive statistics, it is estimated that between 0.5 and 1% of the population are transgender or gender diverse.1,2 Until recently, being transgender was viewed as a psychiatric illness. In 2013, the Diagnostic and statistical manual of mental disorders (5th edition; DSM-V) replaced the diagnostic criteria ‘gender identity disorder’ with ‘gender dysphoria’. Gender dysphoria is the distress felt by the incongruency of a person’s gender and their sex assigned at birth. This can include the stress felt when that person is ‘misgendered’ by other people. Many transgender people do not experience gender dysphoria and thus identifying as transgender or gender diverse in and of itself is not a pathological state.3
Despite these diagnostic changes, people who are transgender or gender diverse continue to face significant prejudice and discrimination, which can negatively impact their mental and physical health. It is important to note that the prevalence of this mental distress is not necessarily a reflection of pathology, but may be related to the additional stressors that come with being a minority. This may manifest in the increased expectation of rejection and prejudice and feeling that they need to hide their identity, thus reducing their resilience and capacity to cope.4
Barriers to accessing health care
Several factors impact on whether transgender and gender diverse people feel safe in accessing health care. These include:
• fear of meeting a new healthcare provider (who might have limited experience, or be rejecting or insensitive during conversations)
• fear of physical examinations
• patient registration forms that may not provide space to record preferred name, identified gender and sex assigned at birth
• confidentiality concerns, especially during transition, as the person may not be out to other service providers or family members
• anxiety that their partner, children and parents may also face discrimination.5
Providing markers of inclusion in the physical space (i.e. waiting and consultation rooms) can promote inclusion and safety. Marker of inclusion could include: posters or a rainbow/transgender flag displayed in the waiting room; intake forms that have spaces to identify gender identity and sex assigned at birth; and resources with information for people who are transgender or gender questioning.
Physical examination
Concerns about physical examination or being treated in an insensitive manner may contribute to increased anxiety about or avoidance of accessing a new service. People who are transgender or gender diverse may be dysphoric about their anatomy or bodily functions and may be uncomfortable with overexposure:
• consider postponing a physical examination until rapport and trust have been established
• allow a support person to be present
• expose only relevant areas of the patient’s body
• allow patients time to undress and re-dress for physical examinations.
You can also prepare your patients for the likelihood of having to undress for an examination or procedure either in your rooms or for a procedure they are being referred to.
Language
The sensitive use of language when describing or enquiring about body parts or functions can ease tension around body and examination. Referring to general body parts or using the third person can neutralise the language. Some practitioners use the word ‘genitals’ rather than vagina/penis/testicles. If the person was assigned female at birth and identifies as male, refer to their ‘chest’ rather than using the word breasts and the menstrual cycle rather than your menstrual cycle. Similarly, for people who were assigned male at birth and identify female, use the words breasts rather than chest and the penis or prostate. Ask the patient:
• Who knows about your gender identity (i.e. family/friends)?
• How would you like to be called through from the waiting room?
• What pronouns do you use to describe yourself?
Clothing and prosthetics
People with breasts and without a penis or scrotum who identify as male will likely wear a chest binder to flatten and minimise the appearance of their chest and may also use a packer (prosthetic penis and scrotum). People without breasts and with a penis and scrotum who identify as female may wear a padded bra, tuck and tape their penis and scrotum, or wear underwear with prosthetics to enhance the hips and buttocks.
Making referrals
Some patients may require referral to medical specialist or allied health practitioners, or require diagnostic tests. Take care with language in your correspondence with other treating practitioners and always use the person’s preferred name, pronoun and, where appropriate, gender and sex assigned at birth in referral letters. As some referrals or procedures may be unrelated to gender, work collaboratively with your patient to determine the necessary information shared and how to best maintain confidentiality.
Being physically examined by the GP, disrobing for a procedure or imaging in a new service can be challenging. If your patient has difficulties with or requirements for physical examinations or tests, discuss with them the idea of including this in the referral letter so that the service is advised in advance and can be respectful and prepared.
Remember to:
• acknowledge (internally) the prejudice and discrimination people who are transgender face and therefore how difficult it can be to access a new service. Acknowledge your own values and how they may impact on the way you interact with a person who is transgender or gender diverse
• affirm the patient for their courage in sharing such personal information
• avoid assumptions, listen to what the patient wants/needs
• ask how best you can support your patient.
Recommendations for physical activity
If treatment recommendations include increasing physical exercise, it is important to consider potential barriers that transgender people may face in adhering to these recommendations.
Regular exercise can be difficult if the person does not have a safe place to walk or work out. Many people who are transgender wear wigs and makeup and are uncomfortable and self-conscious about sweating and wearing exercise clothing. Gyms, swimming pools and other exercise areas can be particularly costly and intimidating (for all of us) and a range of safe alternatives may need to be explored collaboratively.
Maintaining hormone therapy
Gender-affirming hormones can be offered by a gender clinic, some sexual health clinics or by experienced GPs. Transition is tailored to the individual: not all people will choose to take hormones or undergo surgery. Therefore there is no notion of a ‘complete’ or ‘partial’ transition; and it is important to affirm and support the patient in the decisions they make.
Psychologists and social workers who have experience in working with transgender people can assess, monitor and provide intervention for mental health problems and provide guidance around social, legal (e.g. name change), medical and surgical aspects of transition. Speech pathologists can be recruited to help with voice and communication. In larger centres, transition support is usually co-ordinated by a sexual health service for adults and gender clinics for children. Alternatively, an experienced private psychologist can be appropriate; however, a 10-session mental health care plan may not be enough for someone at the start of their transition and cost may be a barrier if there is a gap payment.
For people who have completed their transition, maintenance of hormone therapy, monitoring for side effects and screening for long-term complications can be well managed by their regular GP.6 In complex cases, consider collaborative care with a sexual health physician or endocrinologist.
Feminising hormone therapy
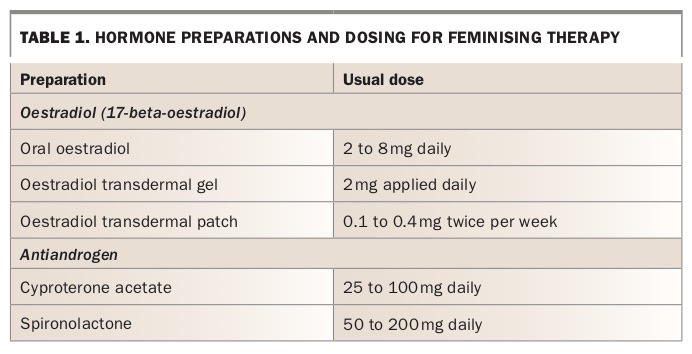
For people assigned male at birth and who identify as female, oestrogen preparations are used for hormonal feminisation therapy (Table 1). As the use of oestrogen independently does not suppress androgen production sufficiently, antiandrogens are often used in combination with oestrogen. This permits the use of lower doses of oestrogen needed to achieve the desired effects. The combination also reduces the potential side effects of high-dose oestrogen therapy.
{kind=link}
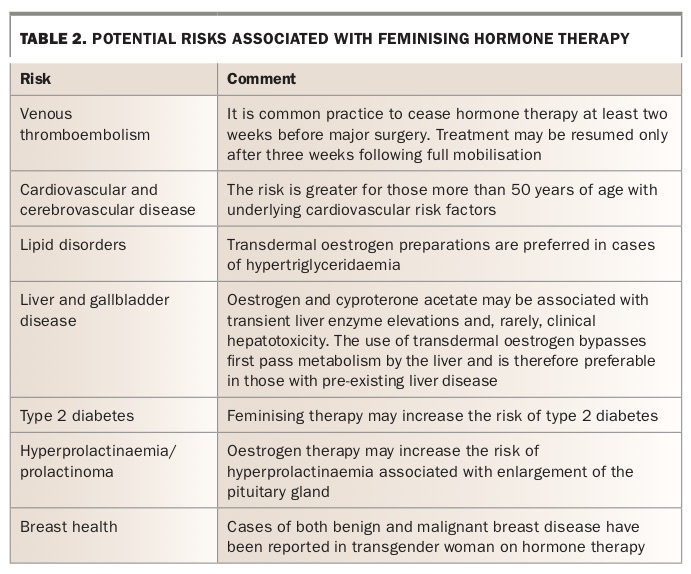
The risk of a serious adverse event is mediated not only by the medication, dosage and mode of administration, but also by patient factors including family history, age, comorbidities and lifestyle habits (Table 2).
{kind=link}
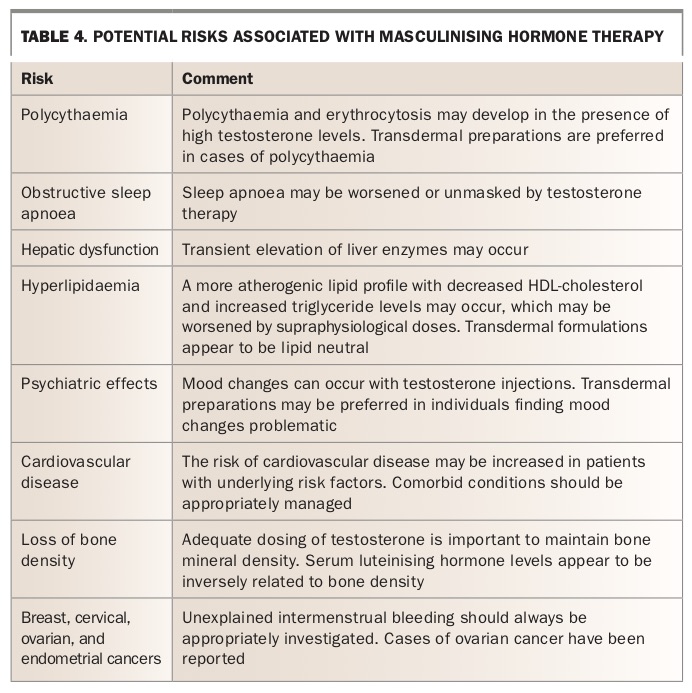
Masculinising hormone therapy
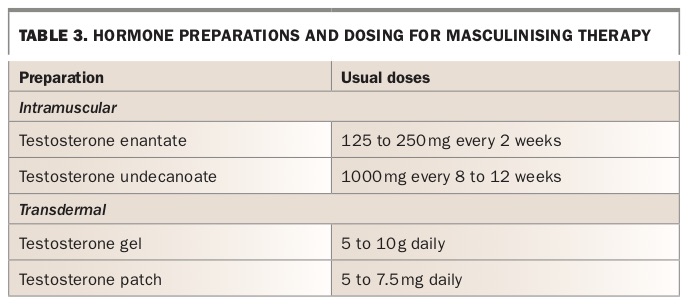
For patients who were assigned female at birth, masculinisation is achieved by testosterone therapy. The preparation and dosage is outlined in Table 3, and the risks of therapy are outlined in Table 4.
{kind=link}
{kind=link}
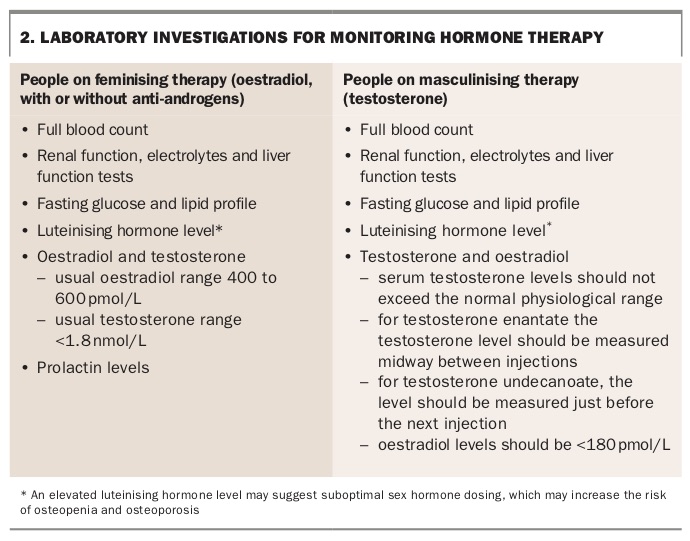
Monitoring and screening
Laboratory investigations for monitoring hormone therapy are recommended at six- to 12-monthly intervals, depending on individual risk factors (Box 2).7 It is also important to perform routine screening activities for early cancer (appropriate to the anatomy present) as per national guidelines.
{kind=link}
Sexual health
Avoid assumptions about a patient’s anatomy, the type of sex they engage in and their sexual orientation – sexuality and gender are not the same and are not related. Through an affirming and supportive but matter of fact discussion, determine what types of regular check-ups (e.g. cervical screening, mammograms) and tests (e.g. sexually transmitted infections) need to be done. Questions should be simple, open and asked without judgement. For example:
• Can you tell me, are you attracted to men, women or both?
• So that we know what types of samples to collect, are you having anal, front hole (vaginal) or oral sex, or all or any of the above?
• Do you generally top, bottom or both?
Some transgender men have front hole (vaginal) sex, however, reduced systemic oestrogen can lead to dryness and discomfort or result in tearing. Topical oestrogen can be offered and the use of a lubricant encouraged.
Contraception and fertility preservation
As gender-affirming hormones are not sufficient contraception in themselves, discuss and offer contraception to all transgender and gender diverse patients, unless they do not have the organs necessary for reproduction.
Before starting hormones, many people will have seen a fertility specialist and some will have stored eggs or sperm for use in future reproduction. Although gender-affirming hormones will not inevitably result in the loss of fertility, it is possible that a person’s ability to reproduce may be affected.
Conclusion
As a friendly inclusive service, a holistic view of the patient sees a person with strengths and challenges, fears and expectations, successes, skills and talents, history, values and relationships and everything else that other patients come with. Everyone is an individual with their own story.
Learning more about transgender medicine can be empowering for both the GP and their transgender patients (Box 3). Taking the time to attend education sessions, and providing education and resources to medical and administration staff, can assist in providing safe and inclusive services for patients who identify as transgender or gender diverse, as well as their families. MT
{kind=link}