Iron deficiency anaemia in adults: an update
Iron deficiency, and therefore iron deficiency anaemia, may result from an increased physiological requirement for iron, insufficient dietary intake, reduced absorption or excessive loss. The gastrointestinal tract is the most important source of excessive iron losses in men and postmenopausal women.
- Iron deficiency anaemia (IDA) is commonly seen in primary care and management principles include: making a confirmed diagnosis of IDA; identifying the cause of iron deficiency; correcting the deficiency.
- Serum iron level is not a useful marker for iron deficiency; the most specific serological marker for iron status is serum ferritin.
- Iron deficiency may result from increased physiological requirements, insufficient dietary intake, reduced iron absorption or excessive iron losses.
- The gastrointestinal tract is the most important source of pathological iron losses in men and postmenopausal women.
- In menstruating women the most common cause of IDA is menstrual loss; however, clinicians should be vigilant for coexisting gastrointestinal causes.
- Endoscopic investigation with gastroscopy and colonoscopy is indicated in medically fit men and postmenopausal women to exclude a gastrointestinal cause.
- Wireless capsule endoscopy may be considered if the cause of IDA remains obscure after gastroscopy and colonoscopy.
- Oral iron supplementation is practical, safe and well-tolerated. Alternate-day dosing can improve tolerability and iron absorption.
- Intravenous (IV) iron infusion is indicated in select patients, including those who are intolerant of or refractory to oral supplementation. Newer IV formulations can provide adequate iron replenishment in one dose with short infusion times and excellent safety profiles.
Iron deficiency anaemia (IDA) is frequently encountered in clinical practice and may be a difficult problem to navigate. It can have a significant impact on cognition, academic achievement, work productivity, exercise tolerance and quality of life. Iron deficiency, even without anaemia, can cause fatigue, cognitive impairment and mood changes, and in patients with heart failure can worsen the degree of heart failure. When a diagnosis of iron deficiency is made a cause must be sought and, where possible, addressed. Replenishment of iron stores with oral iron supplements is appropriate for most patients, but in those who are intolerant of iron or in whom rapid correction of iron deficiency is required intravenous formulations may be indicated.
Iron metabolism
Iron plays a central role in oxygen transport, intracellular oxygen delivery for aerobic glycolysis, DNA synthesis, and immune function. The human body contains 3 to 4 g of iron, with about two-thirds found in the red blood cells. Iron status is closely regulated through hormonal regulation. Central to this is hepcidin, a master regulator hormone secreted by the liver.
After ingestion, dietary iron is absorbed into the enterocytes of the duodenum and proximal jejunum, and exported from enterocytes into the bloodstream via ferroportin, a transporter protein. When iron stores are replete, hepcidin is released and binds to and degrades ferroportin. This prevents the entry of iron into the bloodstream. If this feedback system fails, for example through impaired hepcidin production in hereditary haemochromatosis, iron overload occurs and leads to end-organ damage. Dysregulation of hepcidin can also occur in inflammatory states. The induction of hepcidin can be attributed to the upregulation of interleukin-6 (IL-6) in acute inflammation through the JAK/STAT (Janus kinase/signal transducers and activators of transcription) 3 signalling pathway. This is the mechanism implicated in anaemia of chronic disease, which is commonly observed in patients with chronic infections, malignancies, trauma and chronic inflammatory disorders.
In healthy men and postmenopausal women only 1 to 2 mg of iron is required each day to replenish physiological losses through the shedding of enterocytes, sweat and blood loss. The daily dietary requirement of iron, however, may be much higher due to low fractional absorption of iron in the small intestine. Once absorbed, up to 70% of iron goes towards haemoglobin synthesis, 10% enters the reticuloendothelial system and the remainder is bound to transferrin proteins. Iron is stored primarily as the protein-iron complex ferritin. Ferritin is found in the liver, spleen, bone marrow and skeletal muscles.
Dietary factors in iron absorption
Dietary sources of iron can usefully be classified as haem and non-haem types. Animal products provide haem iron, which is absorbed five times more easily than non-haem iron, found in vegetables, legumes and grains. As a result, much higher quantities of non-haem iron are required to meet physiological needs. Vegetarians and vegans are therefore more likely to have iron deficiency and should be encouraged to consume items including eggs, mushrooms and nuts, which have higher concentrations of non-haem iron.
Iron absorption can also be influenced by other dietary factors. Citrate and ascorbate form complexes with iron that increase absorption, and tannates in black tea decrease absorption. Proton pump inhibitors may reduce the absorption of iron, as a low gastric pH is important to facilitate iron transport.
Definitions of anaemia and iron deficiency
Anaemia is defined by a haemoglobin concentration below the age and sex-defined normal range. Iron deficiency is an important cause of anaemia, but other causes should also be considered. IDA is typically characterised by a microcytic and hypochromic blood film, although this blood film picture may also be seen in other clinical scenarios, such as in people with thalassaemia.
The gold standard for diagnosis of iron deficiency is a bone marrow biopsy with Prussian blue staining. Fortunately, this is rarely required in clinical practice and iron status can usually be determined with noninvasive tests.
Iron deficiency is typically characterised by a low serum ferritin level (<30 mcg/L) and transferrin saturations of less than 15%. (Some laboratories use community-derived reference levels of ferritin, resulting in lower normal ranges; however, these reference populations include some patients who are iron deficient and use of the lower reference range may result in undertreatment of patients who could benefit from iron supplementation and/or investigation for a cause of iron deficiency.) Unfortunately, the diagnosis of iron deficiency is sometimes less clear. Iron deficiency may be present without anaemia. During progressive iron depletion, anaemia may be a delayed finding.
Diagnosis of iron deficiency anaemia
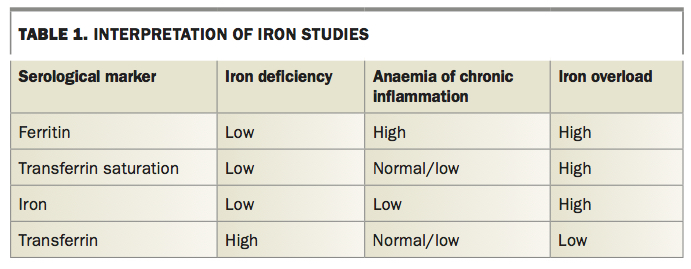
Serum iron concentration is not a useful marker for iron deficiency. The most specific serological marker for iron deficiency is a low serum ferritin concentration. A summary of how to interpret iron studies is provided in Table 1. The finding of a low serum ferritin level always indicates iron deficiency. However, a normal (or even elevated) ferritin level does not exclude iron deficiency. Ferritin is an acute-phase reactant, and acute or chronic inflammation and malignancy may result in an elevated serum ferritin level that potentially masks underlying iron deficiency. Hence, it is important to consider the clinical context at the time of interpretation. In these situations, a low transferrin saturation supports a diagnosis of iron deficiency.
{kind=link}
The soluble transferrin receptor (sTfR) has been proposed as a specific marker for iron deficiency; however, this test is not widely available. sTfR level increases with erythropoiesis in the setting of iron deficiency, and, unlike ferritin, remains normal in chronic disease and inflammation. sTfR level is not superior to serum ferritin level for diagnosis of iron deficiency in head-to-head comparisons.
In some cases, the clinician may consider a therapeutic trial of iron when the presence of iron deficiency is in doubt. The diagnosis is confirmed by resolution of the anaemia and improved red cell indices. Reticulocytosis may be seen after seven days and the patient’s haemoglobin level should increase within four weeks. A lack of response to iron supplementation is not helpful diagnostically and necessitates reconsideration of a bone marrow biopsy.
Anaemia of chronic inflammation (ACI; formerly anaemia of chronic disease) may be difficult to distinguish from IDA, and the two conditions commonly coexist. In ACI, high levels of IL-6 stimulate hepcidin production. The elevated hepcidin impairs absorption of iron and reduces availability of circulating free iron for haematopoiesis. In addition, the high hepcidin level results in a raised serum ferritin level. ACI is also characterised by reduced production of erythropoietin by the kidneys and a reduced bone marrow response to circulating erythropoeitin. These effects and reduced red cell survival all contribute to anaemia. ACI is typically normochromic and normocytic; however, a microcytic and hypochromic picture may occur, particularly when iron deficiency is coexisting.
Diagnostic workup
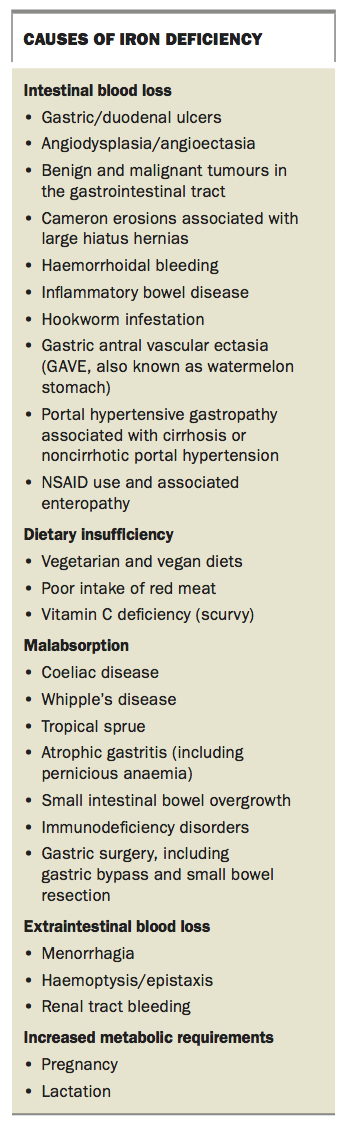
The diagnostic workup for iron deficiency starts with, and is guided by, a comprehensive history and physical examination. The most common causes of IDA are listed in the Box. The likelihood of finding a sinister underlying cause is, in general, proportional to the age of the patient and the severity of the anaemia. Iron deficiency without anaemia is rarely due to a sinister cause.
{kind=link}
In most people with IDA endoscopic evaluation comprising gastroscopy (with small bowel biopsies) and colonoscopy should be undertaken. Gastroscopy identifies the cause of IDA in about a third of patients and colonoscopy in another third. About an eighth of patients have dual pathology.
Urinalysis for haematuria may be useful in evaluating IDA, as 1% of patients with IDA have a renal tract malignancy. A substantial proportion of these patients will have overt haematuria.
Faecal occult blood testing (FOBT) is a useful screening test for colorectal cancer in asymptomatic, average-risk patients. However, in the setting of IDA, FOBT should not be used as an alternative to colonoscopy, and a negative FOBT result should not preclude endoscopic evaluation. Coeliac serological testing is useful in screening for coeliac disease in patients with suggestive symptoms or a family history. However, in the presence of IDA, serology should not replace gastroscopy with duodenal biopsy.
In frail or elderly individuals in whom anaesthetic risk is very high, abdominal CT scanning or colonography are alternatives to colonoscopy and can exclude large lesions or metastatic malignancy. However, the rationale for investigating to identify a potentially malignant condition in this cohort should be considered and discussed with the patient before embarking on investigations. Barium enema is now a largely obsolete investigation since the development of CT colonography.
Iron deficiency anaemia in premenopausal women
The aetiology of iron deficiency can be difficult to determine in premenopausal women. Menstrual losses and increased metabolic demands of pregnancy and breastfeeding are the most common causes of IDA in this cohort. An attempt should be made to quantify menstrual losses. Menorrhagia is experienced by about 30% of women of reproductive age, and self-judgement of menstrual losses can be difficult and unreliable. Coexistent menstrual and gastrointestinal losses occur in up to a third of women. Even when IDA is explained by a history of excessive menstrual blood loss, if iron deficiency persists despite addressing menstrual losses then evaluation of the gastrointestinal tract should be considered.
Iron malabsorption is more common than gastrointestinal bleeding in premenopausal women. Along with correction of iron deficiency, serum tissue transglutaminase (with serum IgA) is a useful screening test in this patient group. However, the presence of gastrointestinal symptoms or other risk factors for gastrointestinal abnormality (such as a family history of bowel cancer) should prompt consideration of endoscopic evaluation.
Obscure and occult gastrointestinal bleeding
Obscure and occult gastrointestinal bleeding is a common and often frustrating problem for patients and clinicians. Occult bleeding refers to gastrointestinal bleeding where blood loss is not clinically evident. Gastroduodenal bleeding of up to 150 mL/day for example, will not result in a change in stool colour but will cause iron deficiency over time. Obscure bleeding is defined as gastrointestinal bleeding that is persistent or recurrent, with no source identified despite initial endoscopic evaluation. Obscure bleeding can be occult, or clinically apparent with frank blood or melaena.
Interrogation of the small bowel should be considered in the setting of obscure bleeding. CT enterography has largely replaced small bowel series for radiological assessment of the small bowel. CT enterography has the advantage of being able to detect both intestinal and extraintestinal gastrointestinal causes of IDA (e.g. renal tract malignancies). However, neither small bowel series nor CT enterography is useful for diagnosis of intestinal mucosal vascular abnormalities such as angioectasia (the most common cause of obscure, small bowel bleeding).
Wireless capsule endoscopy (WCE) or ‘pill cam’ is the most sensitive investigation in the setting of recurrent or persistent iron deficiency anaemia or gastrointestinal bleeding when a gastroscopy and colonoscopy has not identified the source. WCE identifies a source of bleeding in about 60 % of patients but is not therapeutic and does not provide a tissue diagnosis. Many of the mucosal lesions identified with WCE are benign and do not require specific therapy.
After a mucosal lesion is identified by WCE, various enteroscopic techniques may be used for evaluation of the small bowel. Enteroscopy is usually reserved for obtaining a tissue diagnosis (if required) or delivery of therapeutic interventions such as treatment of angioectasias. The simplest technique, push enteroscopy, uses a longer endoscope than for conventional gastroscopy and allows visualisation of the entire duodenum and some of the proximal jejunum. Device-assisted forms of enteroscopy, such as balloon enteroscopy, are more specialised procedures with longer procedure times and greater procedure-associated risks. Balloon enteroscopy uses a specialised endoscope with an overtube that incorporates one or two balloons that are inflated and deflated in order to advance the endoscope further into the small bowel. An anterograde or retrograde approach is taken, depending on the site of interest identified on imaging or WCE.
Iron replacement
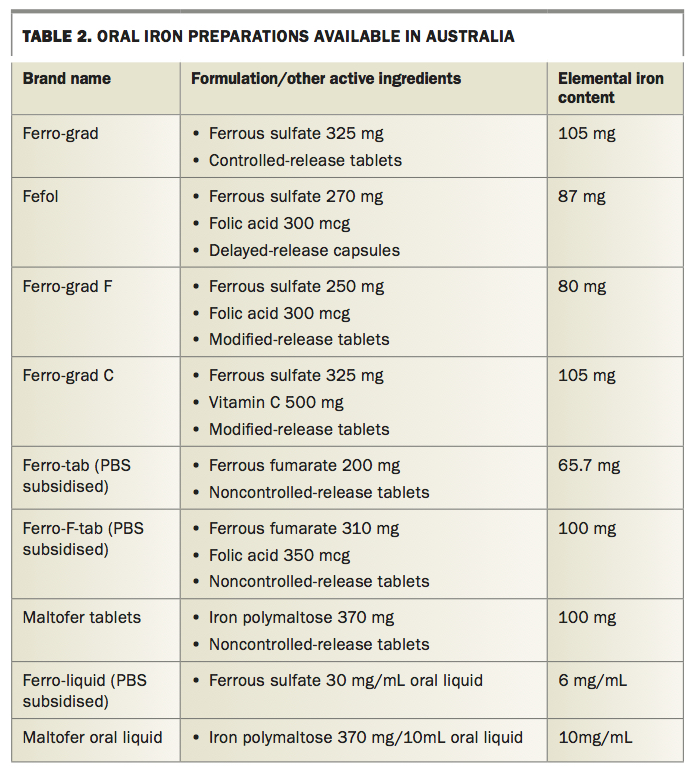
Effective management of IDA relies on iron replacement in addition to addressing the causative factor. Oral iron replacement is appropriate in most patients. It is cheap, well tolerated by most patients, effective and is available in many forms (Table 2). However, gastrointestinal side effects including constipation and nausea occur in 20 to 40% and contribute to poor adherence to treatment. An adequate dose of oral iron is more than 150 mg of elemental iron per day. Treatment should continue until anaemia has resolved (usually three to six months) and a further six months of therapy may be undertaken to ensure adequate replenishment of body stores. Failure to respond to oral iron treatment may be due to noncompliance, malabsorption, incorrect diagnosis, intercurrent disease (such as renal failure) or ongoing gastrointestinal blood loss. In patients with an adequate response to iron therapy, haemoglobin levels should rise by 20 g/L every three weeks on iron supplementation. All patients should be monitored for recurrence of anaemia or iron deficiency.
{kind=link}
There are no high-quality studies demonstrating the superiority of any one formulation of oral iron. The formulations that are subsidised under the PBS in Australia are ferrous fumarate with and without folic acid and ferrous sulfate liquid, which provide appropriate doses in a bioavailable form. Sustained-release preparations (all the available ferrous sulfate tablets and capsules) may be less effective as they are not available for absorption in the duodenum, which is the primary site for iron absorption. Liquid iron replacement allows divided daily doses but the taste may be a barrier to adherence and it can cause dental staining. Newer nonionic formulations such as iron polymaltose have equivalent efficacy to iron sulfate preparations, but may have better gastrointestinal tolerability and can be taken with food. Currently, they are more expensive than other preparations. There is emerging evidence that alternate-day, low-dose (40 to 80 mg) iron supplementation results in better absorption compared with daily dosing at the currently recommended dose of 150 mg, which raises circulating hepcidin levels to counteract iron absorption. Oral iron should be administered apart from calcium supplements, antacids and food intake to maximise absorption. Concurrent administration of vitamin C can aid absorption.
Intramuscular iron injection is painful and can lead to permanent tattooing. Intramuscular iron is poorly absorbed, and is no more effective and does not replenish iron stores any faster than oral iron supplementation. As a result, there is little place for intramuscular iron replacement in current practice.
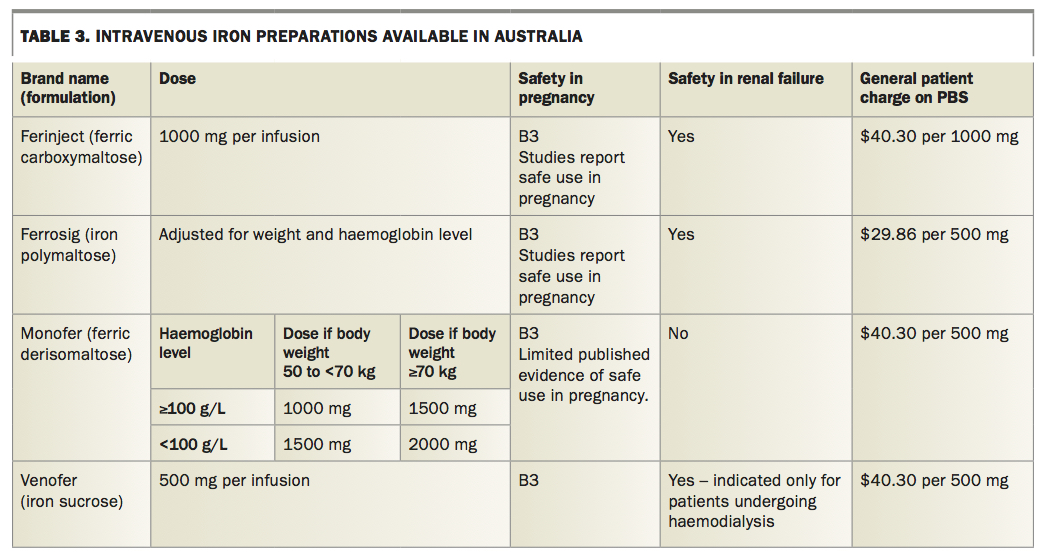
Intravenous iron replacement is appropriate for a select group of patients who cannot tolerate oral iron, or who require rapid delivery of iron. A list of currently available intravenous iron formulations is given in Table 3. Unlike the older, high-molecular-weight preparations of intravenous iron, the currently available, low-molecular-weight preparations such as iron sucrose and iron polymaltose are well tolerated, with a low risk of anaphylactic reactions. Iron sucrose is the formulation of choice for patients undergoing dialysis and receiving concurrent erythropoietin stimulating agents, in whom slower infusion times and lower doses are less important. Iron polymaltose has a longer infusion time but is less expensive and has the advantage of being dose adjusted for body weight and sex. Iron polymaltose is the preferred formulation for inpatients when prolonged infusion times are of less significance.
{kind=link}
The newest intravenous formulations such as ferric carboxymaltose and ferric derisomaltose have the advantage over other formulations of much shorter infusion times. Ferric carboxymaltose is delivered over 15 minutes at a maximum dose of 1000 mg, which renders it the most practical formulation for use in general practice or an outpatient setting. There is extensive experience of safe use of ferric carboxymaltose in pregnancy, although it does carry a B3 category from the TGA and it is generally advised to avoid IV iron during the first trimester. Ferric derisomaltose was approved for subsidisation under the PBS in February 2019. It can be administered at a dose of up to 1500 mg. Doses of up to 1000 mg can be administered over 20 minutes. Doses exceeding 1000 mg can be administered over 30 minutes. Despite the good safety profile of modern intravenous iron preparations, a small proportion of patients experience anaphylactic reactions and it should therefore be administered in a setting where resuscitation facilities are available.
Blood transfusion is not an appropriate treatment for iron deficiency anaemia, except in rare clinical circumstances, such as patients with end-organ compromise or continued, haemodynamically significant bleeding.
Conclusion
IDA is commonly encountered in primary practice. The diagnosis is usually made by correct interpretation of a full blood count and iron studies. Once the diagnosis is made, a cause should be sought through careful clinical assessment and the deficiency should be corrected, usually with oral iron therapy. Gastrointestinal bleeding is the most common cause of iron deficiency in men and postmenopausal women. In most medically fit patients with iron deficiency anaemia, endoscopic evaluation of the upper and lower gastrointestinal tract with gastroscopy and colonoscopy should be performed. MT