Iron infusions in general practice

Intravenous iron infusions offer a safe and efficacious alternative to oral iron for the replacement of iron in selected patients with iron deficiency, with or without anaemia. Intravenous iron formulations differ in recommended infusion rate, maximum dose per infusion and adverse effect profile, giving clinicians a choice for administration in the outpatient setting.
Iron deficiency is a health condition in which iron availability is insufficient to meet the body’s needs.1 In 2017, 1.3 billion people worldwide were affected by iron deficiency.2 The prevalence of anaemia in Australia is highest among children (13.3% of those aged under 5 years), pregnant women (15.7%) and nonpregnant women of childbearing age (8.2%), with iron deficiency estimated to contribute to anaemia in 25% of children and 37% of women.3,4
Causes of iron deficiency may be categorised into inadequate oral intake of iron, malabsorption in the gut and excessive blood loss, with menstrual and gastrointestinal losses most common. This article provides an overview of the management of iron deficiency, focusing on the use of intravenous iron in primary care.
Iron homeostasis and deficiency
Iron is an essential element for all body cells. It is fundamental for erythropoiesis but also plays a role in immunity, DNA synthesis and as a cofactor in many enzymatic reactions.5 Iron is either obtained from the diet and absorbed in the small intestine or recycled from senescent red blood cells.5
Ferroportin is the key iron transporter located on the basolateral membrane of enterocytes and macrophages of the reticuloendothelial system, where it exports iron into the systemic circulation. Ferroportin is negatively regulated by hepcidin, a hormone released by the liver in response to lipopolysaccharide and interleukin-6 in the context of systemic inflammation.6
Absolute iron deficiency is a state when total body stores of iron are inadequate to meet demand. In contrast, functional iron deficiency occurs when, despite adequate total stores, iron is unable to be mobilised for erythropoiesis. This can occur in the setting of inflammation, where hepcidin levels are raised, leading to downregulation of ferroportin, trapping iron in enterocytes or macrophages.7
Recognition of iron deficiency
Iron deficiency may be asymptomatic or may result in fatigue, reduced cognitive function, hair loss, restless legs, adverse pregnancy outcomes and anaemia.8
A serum ferritin level less than 30 mcg/L is considered diagnostic of iron deficiency, with a sensitivity of 92% and a specificity of 98%.9 However, serum ferritin is an acute phase reactant and therefore a false normal or high level may occur in states of inflammation, resulting in diagnostic uncertainty. Hence, markers of inflammation such as C-reactive protein, erythrocyte sedimentation rate, or faecal calprotectin in states of intestinal inflammation may need to be measured to interpret iron studies.
The WHO defines diagnostic cut-offs for iron deficiency in the setting of inflammation as a ferritin level less than 30 mcg/L in children aged under 5 years and less than 70 mcg/L in older children and adults.10 However, clinical practice guidelines have used ferritin levels up to 100 mcg/L or more to define iron deficiency in the setting of inflammation.11,12
Management
The management of iron deficiency includes both the replacement of body iron stores and investigation for an underlying cause. Iron can be replaced through oral or parenteral routes. Investigation for the cause of iron deficiency was summarised in the March 2022 issue of Medicine Today.13
There are limited indications for the use of red blood cell transfusions to treat iron deficiency; the British Society of Gastroenterology suggest that red cell transfusions should be reserved for those with severe symptomatic anaemia and haemodynamic compromise.12 In this context, patients should be hospitalised to facilitate more invasive monitoring and management.
The recommended dietary intake of iron is 8 to 10 mg daily in adults, with higher requirements in women of reproductive age, because of iron losses in menstruation, and pregnant women.14 Dietary modifications have a role in the primary prevention of iron deficiency but are ineffective for the treatment of established iron deficiency.
Contraindications and precautions to iron supplementation
Iron supplementation should be avoided in patients with known iron overload, such as those with haemochromatosis and haemosiderosis. Intravenous iron is contraindicated in the first trimester of pregnancy.15
Oral versus parenteral iron replacement
The choice between oral and intravenous iron replacement depends on several factors, including the severity of the associated anaemia, local availability of iron preparations and the ability of the patient to tolerate the side effects of oral iron. For most patients with iron deficiency, oral iron replacement is the appropriate first-line therapy and has the advantages of being cheap, readily available, generally effective when taken correctly and safe. Although iron and vitamin C are commonly prescribed together, a recent randomised controlled trial showed that oral iron alone was equivalent to oral iron plus vitamin C in regards to the rise in haemoglobin and ferritin levels at two weeks, with no difference in reported adverse effects between the groups.16
The tolerability of oral iron is limited by gastrointestinal side effects in 20 to 50% of patients, including abdominal pain, constipation, diarrhoea or nausea, leading to discontinuation of therapy.17 Strategies to reduce the frequency of gastrointestinal side effects include changing to alternate-day dosing and switching formulations.18
Parenteral iron is preferred for patients with intolerance or lack of efficacy of oral iron, symptomatic or severe anaemia, chronic kidney disease, cardiac failure or anaemia associated with malignancy, and for patients with conditions that interrupt the absorption of oral iron (previous gastrectomy or bariatric surgery, or inflammatory bowel disease). Intramuscular iron injections are no longer recommended because of the risks of pain at the injection site, poor absorption and skin staining; intravenous iron is preferred.19,20
The benefits of intravenous iron over oral replacement are the rapid replacement of bodily iron stores, low rates of side effects and favourable safety profile. Although both oral and intravenous iron replacement have been shown to increase haemoglobin levels in patients with anaemia, intravenous iron is associated with a greater rise in haemoglobin.21
Intravenous iron
Four formulations of intravenous iron are currently available in Australia:
- ferric carboxymaltose
- ferric derisomaltose (also known as iron isomaltoside)
- iron polymaltose
- iron sucrose.
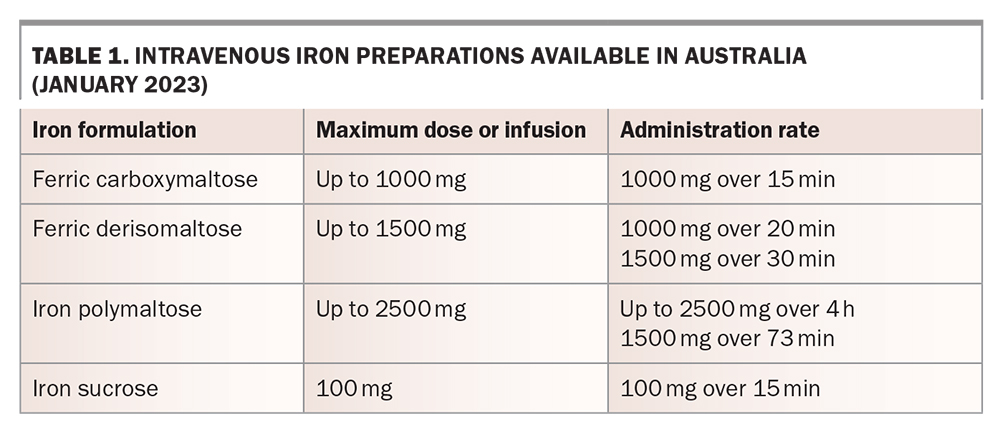
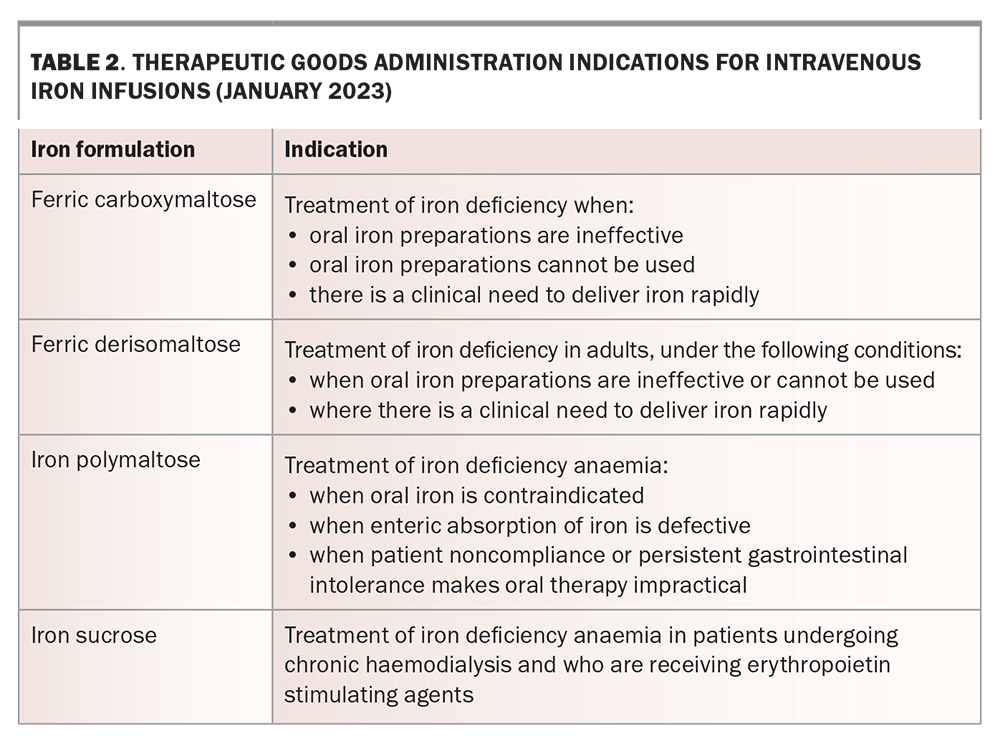
The choice of intravenous iron formulation depends on multiple factors, including duration of the infusion, maximum dose able to be administered in a single infusion and safety profile (Table 1). Iron sucrose is predominantly administered to patients with chronic kidney disease undergoing haemodialysis. The Australian product information for iron sucrose recommends a dose of 100 mg per dialysis session, but 200 to 300 mg has been reported as safe for administration.22-24 Iron polymaltose may be administered in large doses of up to 2.5 g in a single infusion, with a generally recommended infusion duration of four to five hours. A shorter infusion time of 73 minutes for doses up to 1.5 g has been shown to have a satisfactory safety profile.25
{kind=link}
The newer formulations of intravenous iron, ferric carboxymaltose and ferric derisomaltose, have the advantage of allowing rapid administration, enabling outpatient administration. The higher cost of these formulations may be offset by the savings associated with the shorter time in infusion chairs and less nursing requirements.26 The current TGA-approved indications for each iron preparation are summarised in Table 2.
{kind=link}
Calculating the dose of intravenous iron
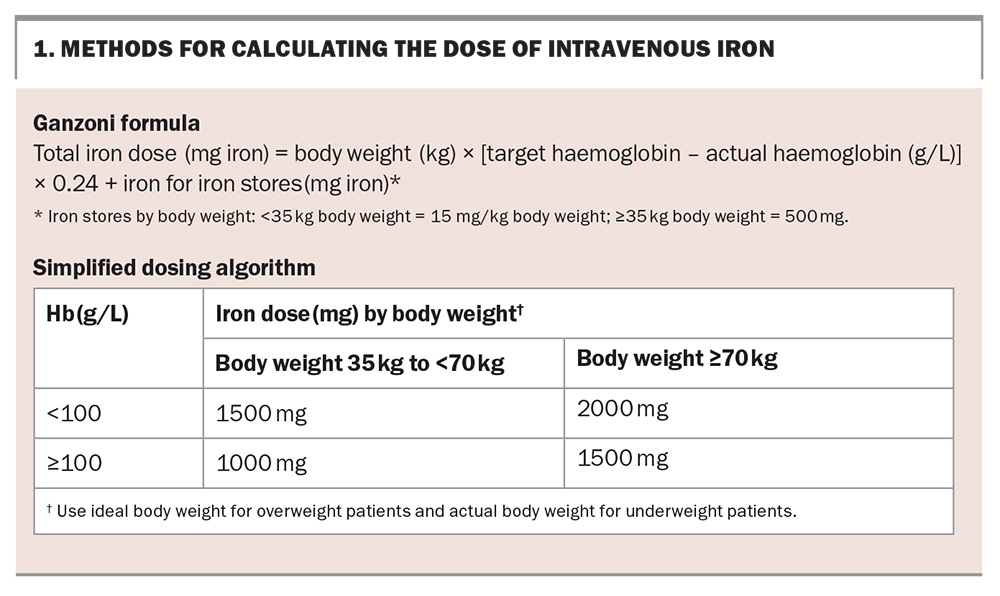
There is no standard dose of intravenous iron. Each patient will have a unique total body iron deficit, which is the amount of iron replacement required to replenish the body’s stores. This deficit can be calculated using the simplified iron dosing algorithm or the Ganzoni formula to determine the number of doses of the preferred iron preparation required (Box 1). Iron infusions should be prepared and administered in line with local guidelines.
{kind=link}
Expected effects of intravenous iron
Intravenous iron is expected to increase haemoglobin by 20 to 30 g/L over eight weeks.27 It has been shown to improve self-reported fatigue in adults with nonanaemic iron deficiency, to reduce the need for perioperative blood transfusions when given preoperatively to patients with iron deficiency anaemia, and to improve New York Heart Association status in patients with heart failure.28-30 The response to intravenous iron supplementation should be checked with a full blood count and iron studies between four and eight weeks after treatment.12 International guidelines do not include recommendations for monitoring reticulocyte count.
Adverse effects of intravenous iron supplementation
Infusion reactions
Infusion-associated adverse effects occur in 10 to 40% of patients during or up to two weeks after intravenous iron administration. These include headache, flu-like symptoms, arthralgia and myalgia.
Infusion reactions are uncommon, but Fishbane-type reactions comprising flushing, chest tightness and dyspnoea may occur. These are thought to be a manifestation of nonallergic complement activation-related reactions rather than allergic hypersensitivity.31 Mild to moderate infusion reactions may be more common with certain iron formulations, occurring in 8.7% of patients who received ferric derisomaltose compared with 2.1% of patients who received ferric carboxymaltose in one study.32 These reactions are best managed by temporary cessation of the iron formulation, ensuring resolution of symptoms, then recommencement at a slower rate of infusion.33
Serious or severe hypersensitivity reactions have been described in 0.3 to 1% of patients in clinical trials.34-36 In these situations, the infusion is best ceased for a few minutes, waiting for resolution of symptoms. Clinics administering iron infusions should be equipped with resuscitation equipment, and staff trained in basic life support. True anaphylaxis to modern intravenous iron formulations is rare and may comprise angioedema, stridor and hypotension. In such situations, management as appropriate for anaphylaxis should be instituted.
The patient’s vital signs (temperature, pulse, respiratory rate and blood pressure) should be monitored for signs of hypersensitivity reactions during the infusion and for 30 minutes afterward.
Iron extravasation
Staining at the cannula site caused by iron extravasation can be permanent. This usually results from an inadequately sited cannula; therefore, checking cannula patency before administration of iron is mandatory. Informed consent for this complication should be obtained before the infusion.
Delayed adverse effects
Delayed adverse effects occur in 15 to 30% of patients up to two weeks after an iron infusion. Symptoms include headache, flu-like symptoms, fatigue and lethargy.37 These symptoms are generally self-limiting, but patients should be informed of their possibility and provided with written instructions on what to do and whom to contact in case of the occurrence.
Hypophosphataemia
Hypophosphataemia has been documented after administration of all intravenous iron formulations, typically with a nadir at one to two weeks. The risk of hypophosphataemia is higher with ferric carboxymaltose (40 to 70%) than with other formulations (generally under 8%).38-40 Although hypophosphataemia is transient and asymptomatic in most patients, it may be persistent and severe in a small proportion. Cases of persistent hypophosphataemia with osteomalacia and fractures have been described, mostly following repeated infusions of ferric carboxymaltose.41 Hypophosphataemia is likely mediated by a transient increase in intact fibroblast growth factor-23 due to inhibition of its cleavage, resulting in phosphaturia.42
Risk factors for developing hypophosphataemia after intravenous iron include malnutrition, repeated iron infusions, baseline hypophosphataemia and the use of concomitant antiresorptive therapy (denosumab and bisphosphonates).43 Patients with chronic kidney disease are protected from intravenous iron-induced hypophosphataemia.44 Routine monitoring of phosphate after iron infusion is not currently recommended but may be required in selected patients at high risk of hypophosphataemia.
In patients with a history of hypophosphataemia secondary to ferric carboxymaltose who require ongoing iron infusions, an alternative iron formulation such as ferric derisomaltose or oral iron replacement should be considered.45
Conclusion
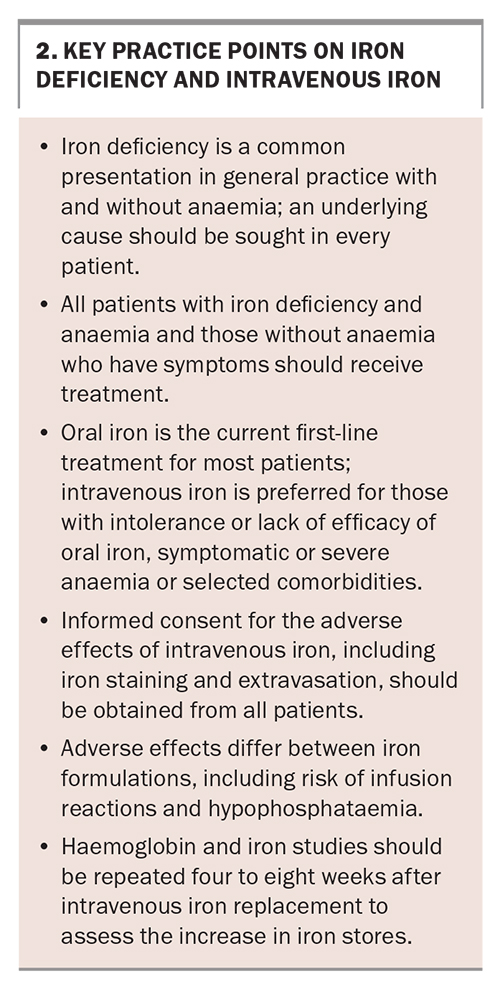
Iron deficiency is a common problem encountered in general practice. Key practice points on iron deficiency are summarised in Box 2. Patients with iron deficiency, especially those with anaemia, should receive iron replacement, coupled with investigation for the underlying aetiology. Intravenous iron allows for rapid iron replacement and is safe in the outpatient setting for most patients, but different profiles of dosing and adverse effects warrant consideration by clinicians. MT
{kind=link}
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.