New horizons in migraine therapy: CGRP monoclonal antibodies
Migraine is one of the most common and disabling diseases worldwide. However, few disease-specific treatments exist. Calcitonin-gene related peptide (CGRP) monoclonal antibodies are a new class of medication for migraine that represent a welcome addition to our armamentarium for migraine.
Migraine is the most common neurological disease worldwide, affecting over one billion people. Worldwide, it is the second leading cause of age-adjusted disability life years (DALYs).1 In Australasia, it is the leading neurological cause of DALYs, ahead of stroke (which is second), epilepsy (sixth) and multiple sclerosis (10th).1 The health economic burden of migraine is significant and has been estimated at $35.7 billion, with $14.3 billion in direct health costs throughout Australia in 2018.1,2
Until relatively recently, few disease-specific treatments or preventives for migraine existed. Calcitonin-gene related peptide (CGRP) monoclonal antibodies are a new class of medication for migraine that represents over 40 years of research and development. This article discusses the role of CGRP monoclonal antibodies in management of patients with migraine.
Reducing the burden of migraine
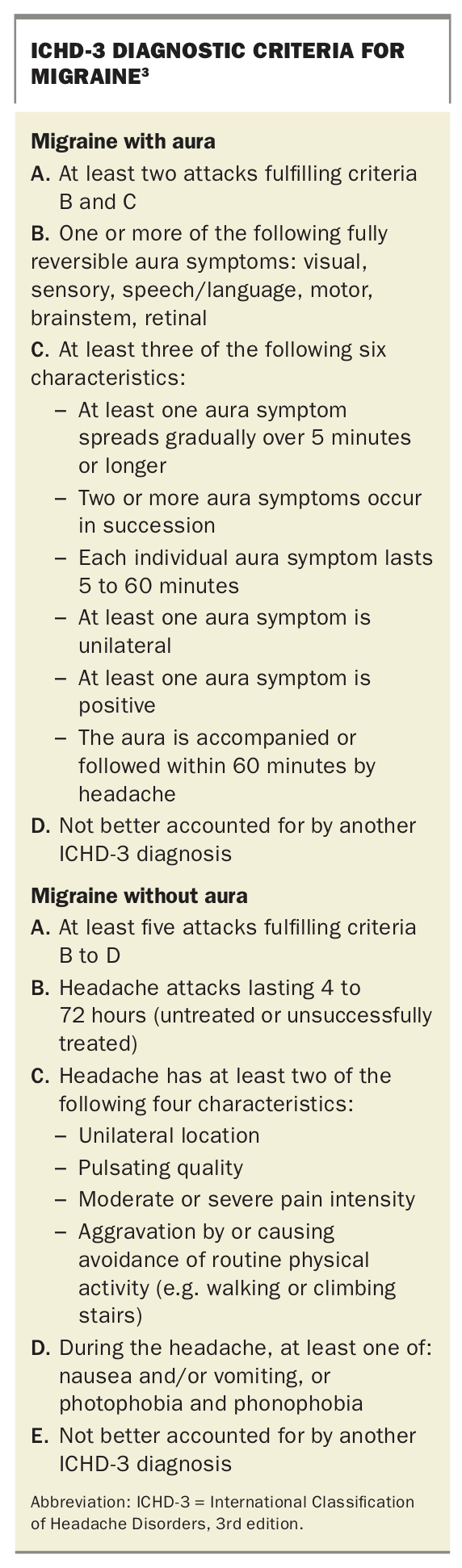
The key to reducing the burden is recognising and diagnosing migraine. The diagnostic criteria for migraine are listed in the Box.3
{kind=link}
The brief ID migraine questionnaire has a sensitivity of 0.84 (95% CI 0.75 to 0.90) and specificity of 0.76 (95% CI 0.69 to 0.83) for diagnosing migraine.4 Two or three positive responses to the following three questions suggest a diagnosis of migraine.
- In the past three months with your headaches:
– Have you felt nauseated or sick to your stomach?
– Has light bothered you a lot (or a lot more than when you do not have headaches)?
– Have your headaches limited your ability to work, study, or do what you needed to do for at least one day?
After migraine is recognised, clinicians can reduce its burden by:
- developing an effective acute treatment strategy, generally a combination of NSAIDs, triptans and antiemetics, and
- limiting the number of attacks per month by optimising lifestyle factors and preventive medication.
Every year, in 2.5% of patients with episodic migraine (less than 15 attacks per month), the condition transforms to chronic migraine (15 or more headache days per month, of which at least eight are migraines), with associated negative impacts on quality of life and healthcare use. The key modifiable risk factors for progression are inadequate preventive medication, overuse of acute medications, obesity, depression, anxiety and stress. A key barrier to reducing the frequency of attacks is the tolerability of preventive medication. In one study, only 70% of patients were still taking their preventive medication at six months, with side effects commonly reported as a reason for stopping.5-7
CGRP monoclonal antibodies
CGRP is a neuropeptide that is expressed in trigeminal neurons, as well as widely throughout the body. Through the trigeminocervical system, CGRP has been implicated in the generation of pain in migraine.8 Several monoclonal antibodies that target CGRP have been developed as treatments for migraine.
Three of these CGRP monoclonal antibodies are available in Australia:9-11
- erenumab targets the CGRP receptor
- fremanezumab and galcanezumab bind to the ligand CGRP itself.
All three are administered subcutaneously. A fourth monoclonal antibody that also targets the CGRP ligand but is administered intravenously, eptinezumab, has been developed but is not currently approved by the TGA.
How well do CGRP antibodies work?
Overall, CGRP monoclonal antibodies appear to be effective in the prevention of migraine. In phase three trials in people with episodic migraine, the percentage of patients who halved the number of their monthly migraine days (50% responder rate) was between 45 and 60% for each of erenumab, fremanezumab and galcanezumab, compared with 28 to 38% for placebo. This equated to approximately four less migraine days per month with the CGRP monoclonal antibodies.8
When trialled in people with chronic migraine, the CGRP monoclonal antibodies also showed efficacy, with a 50% responder rate of between 28 and 41%, or five to seven fewer migraines per month. Efficacy for each medication in phase 2 and 3 trials is summarised in Figure 1 and Figure 2.8 However, as each trial was performed on different patient populations and not head-to-head, direct comparison of efficacy is not possible.
{kind=link}
These promising trial data appear to translate into the ‘real world’. Several Australian headache neurologists have pooled their collective experience with erenumab in a cohort of 170 patients with refractory chronic migraine (86% having not had an adequate response to five or more preventive medications, and 95% having trialled botulinum toxin). In this group, the 50% responder rate was 46.5%, or 10 fewer migraine days per month after six months.8,12
When are CGRP antibodies used?
The CGRP monoclonal antibodies erenumab, fremanezumab and galcanezumab have been trialled and may be used in patients with high-frequency episodic migraine (10 to 14 migraine days per month) or chronic migraine as a preventive medication.
At the time of writing, galcanezumab is expected to be made available on the PBS in June 2021, restricted to patients with chronic migraine treated by a neurologist who have unsuccessfully trialled three preventive medications and are not receiving botulinum toxin. Treatment response should be assessed after eight to 12 weeks of therapy.
Fremanezumab has been recommended for PBS listing for chronic migraine by the Pharmaceutical Benefits Advisory Committee (PBAC) but is yet to be listed on the PBS, and erenumab has been withdrawn from the PBS process. As such, erenumab and fremanezumab are available only via private prescription at a cost per month of $695 and $283, respectively.
Side effects
Common side effects
Overall, these medications have been well tolerated, with a few shared side effects. Local injection site reactions occur in about 5% of patients, and 3 to 6% experience fatigue. Nasopharyngitis and sinusitis were reported in both placebo and active groups (2 to 6%). The most common side effect appears to be constipation. Real-world data suggest constipation may occur in 10 to 20% of patients, as opposed to the 1.4 to 2.1% reported in trials.8
Theoretical and potential side effects
It is worth noting that, although our early experience with these medications has been favourable, they are a new class of medication that modulates a neuropeptide that is widely expressed throughout the body. Off-target effects may be possible.
The primary concern rises from the role of CGRP as a mediator of vasodilation, raising a theoretical concern about its effect on coronary or cerebral artery vasoconstriction. To address this, a trial assessed the effect of CGRP inhibition on patients with stable angina, and reported no reduction in exercise tolerance or ECG changes. However, the effect of long-term blockade has not been assessed.13
The CGRP monoclonal antibody therapies may worsen hypertension, and the FDA has included a postmarket warning label. Given patients with cardiovascular disease were excluded from the trials, European guidelines advise against their use in this cohort.14
Several other physiological actions of CGRP should be considered in deciding whether these medications are appropriate. CGRP strengthens the blood-brain barrier, promotes mucosal integrity in the gut, and may shift the immune system to a more anti-inflammatory phenotype.15 Caution is therefore needed in patients with conditions such as multiple sclerosis, peptic ulcer, Crohn’s disease and pre-existing autoimmune disease. Long-term CGRP inhibition may have an impact on bone density.8 These concerns are largely theoretical at this stage, with no clear evidence as to whether or not they will be practical impediments to use.
Precautions and interactions
Trials of these agents recruited nonpregnant patients aged 18 to 65 years who had no significant psychiatric, cardiovascular or hepatic comorbidity. As such, there is no experience in the paediatric or geriatric population, and no human data on use during pregnancy or lactation. CGRP has a role in placental development, and so use by pregnant or breastfeeding women is not recommended.
The CGRP monoclonal antibody medications are not metabolised by cytochrome P450 enzymes, and as such are unlikely to interact with other P450 inducers or inhibitors. However, the impact of significant hepatic impairment on their metabolism is not known. Mild to moderate renal impairment does not require dose adjustment.
What needs monitoring?
As with any preventive medication, treatment response should be assessed, through measures of number of headache days and quality of life at baseline and eight to 12 weeks after starting the medication. Side effects, both serious and mild, should be monitored by the prescribing physician. Routine blood tests are not mandatory but could be useful. Our practice is to assess the full blood count, liver and renal function, inflammatory markers, vitamin D and thyroid function tests. Baseline and ongoing blood pressure measurement is also advised.
Other CGRP targeted therapies
In addition to the CGRP monoclonal antibodies, several other medications for both acute treatment and prevention of migraine are on the horizon. The first group are small molecule CGRP antagonists (gepants), including atogepant, rimegepant and ubrogepant. These medications have all undergone phase 3 trials for acute treatment of migraine and are now being investigated as possible migraine preventives. Currently, they are not available in Australia and have not been registered with the TGA.
A new class of acute therapies that target the 5-hydroxytryptamine 1F (5-HT1F) receptor are under development. Known as ditans, they are a sister group to the triptans (5-HT1B/1D receptor agonists). However, the ditans are being developed to avoid the vasoconstricting effect of the triptans. They are undergoing clinical trials.
Advantages of CGRP monoclonal antibody therapies
There is considerable excitement among headache specialists about the CGRP monoclonal antibody therapies for migraine. Reasons include the following.
- These medications are remarkably well tolerated, which is especially welcome as many patients report difficulty with standard preventive treatments for migraine.
- Monthly injections reduce the risk of nonadherence and pill burden for patients.
- The similar results across the class of medications, first in trials and now in real-world practice, suggest that the observed benefits are genuine.
- A small group of patients show complete or near-complete remission from migraine attacks, an outcome not often seen with oral migraine preventive agents.
An overview of migraine treatment and the role of CGRP therapies is shown in the Flowchart.
Conclusion
CGRP monoclonal antibodies are the first of a new class of migraine agents to arrive in Australia. Trial and real-world data show they are safe and effective for the vast majority of patients. Ongoing monitoring for possible long-term side effects of this class of medications is advisable. However, they represent a welcome addition to our armamentarium for migraine.
COMPETING INTERESTS: Dr Hutton has served on advisory boards for Sanofi-Genzyme, Novartis, Teva, Eli Lilly, Allergan and Lundbeck; has been involved in clinical trials sponsored by Novartis and Teva; and has received payment for educational presentations from Allergan, Teva, Eli Lilly and Novartis. Associate Professor Stark has served on advisory boards for Novartis, Teva, Eli Lilly, Allergan and Lundbeck; and has received payment for educational presentations from Allergan, Teva, Eli Lilly and Novartis. Dr Ray, Dr Cheng, Dr Zhang: None.
Disclaimer
This article is for general information purposes and the approved product information should be consulted before prescribing any discussed medications.