Hoarseness: a patient profile-based guide to diagnosis and management

Hoarseness of voice is a common symptom with many possible causes, and thorough history taking is essential to identify the underlying aetiology. Persistent hoarseness requires prompt evaluation, especially for professional voice users, such as singers and teachers, and high-risk individuals showing red flag signs. An array of office-based diagnostic and therapeutic tools is now available for managing laryngeal disorders.
Dysphonia is defined as any impairment of voice production. Hoarseness is a symptom that is considered to be a subset of dysphonia and refers to a perceived rough, harsh or breathy quality to the voice.1 About a third of the world’s population experiences hoarseness during their lifetime.2,3 A wide array of causes, ranging from structural lesions secondary to misuse or overuse of the voice, infections, premalignant and malignant disorders, and neurolaryngeal problems, can cause changes in voice.
Laryngologists often work in a multidisciplinary fashion with speech and language pathologists and other medical specialists in managing patients with dysphonia. For example, they may work with neurologists for treating patients with Parkinson’s disease and laryngeal dystonia, with gastroenterologists for patients with reflux disease, and with respiratory physicians for the management of chronic cough and underlying lung disorders.
Primary care physicians tend to see a higher proportion of acute voice problems, such as viral laryngitis, whereas otolaryngologists generally become involved in the setting of more subacute and chronic problems.4 Viral laryngitis is the most common cause of acute hoarseness in the community. It is typically self-limiting and should resolve within five to seven days. Supportive treatment, including hydration and steam inhalation, is indicated. Voice rest is advisable to reduce the risk of more permanent damage to the vocal folds, such as scarring.
In rural and regional areas, mild and early dysphonia may receive less attention, due to perceived low morbidity and often limited or delayed access to otolaryngologists. A keen ear and thorough history taking can assist greatly in triage of these patients and prediction of the potential underlying aetiology. Assessment of the dysphonic patient by history and physical examination includes, but is not limited to:
- recent surgical procedures involving the head, neck or chest
- recent intubation
- presence of concomitant neck masses
- respiratory distress or stridor
- other medical illnesses and drug intake
- history of smoking
- whether the patient is a professional voice user.
This article uses a patient profile-based approach to cover the most commonly associated diagnoses for patients with persisting hoarseness (of more than one week). It is important to understand that patients may not have all the symptoms or features in the scenarios described here, or they may have additional symptoms, lesions or compensatory changes, depending on their disease or abnormality. For dysphonia that does not improve despite conservative measures, a laryngoscopy is strongly recommended.3 Specialist referral is highly recommended for any patients not showing dramatic improvement within three to four weeks, especially if they are professional voice users. Common causes of hoarseness of voice are shown in the Table, and practice points are summarised in the Box.
{kind=link}
{kind=link}
Scenario 1
A primary school teacher presents with a six-month history of rough voice, pain in the neck while speaking, vocal fatigue and inability to meet vocal demands at work. Her symptoms are aggravated by speaking and much worse by the end of the week. Her voice improves with rest (on weekends and holidays) but never normalises. Differential diagnoses include:
- nodules
- polyps
- cysts
- pseudocysts
- scarring
- varices
- ectasias
- other fibrovascular lesions
- muscle tension dysphonia.
Voice professionals (akin to vocal athletes) are more likely to encounter phonotraumatic lesions of the vocal cords, which generally occur from heavy use or suboptimal vocal techniques without use of amplification devices. The ‘striking zone’ between the anterior and middle third of the vocal cord is most often affected, due to increased shearing forces in this area.
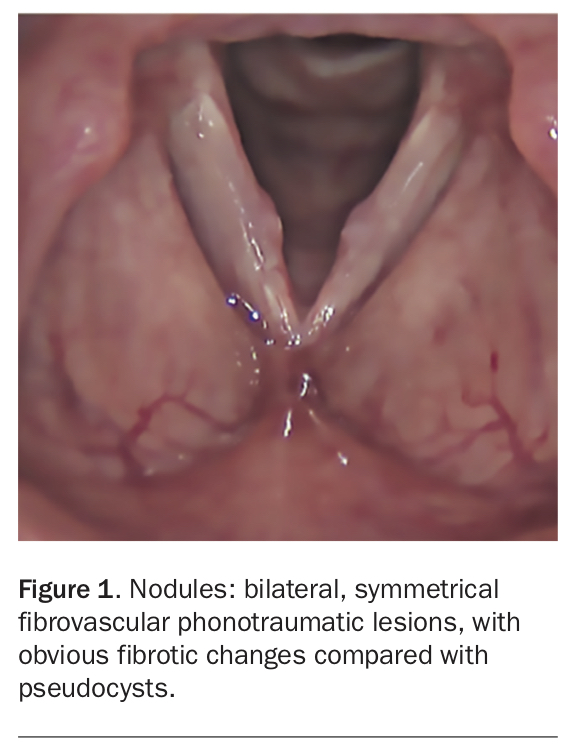
Acute injury can manifest as vocal haemorrhage and inflammation. Chronic trauma can cause excess collagen and fibrin deposition in the basement membrane, leading to nodules (Figure 1), or can induce capillary injury in the vibratory layer, known as the superficial lamina propria, with escape of blood and local reaction to this insult leading to oedema and, finally, polyp formation (Figure 2).5,6
{kind=link}
{kind=link}
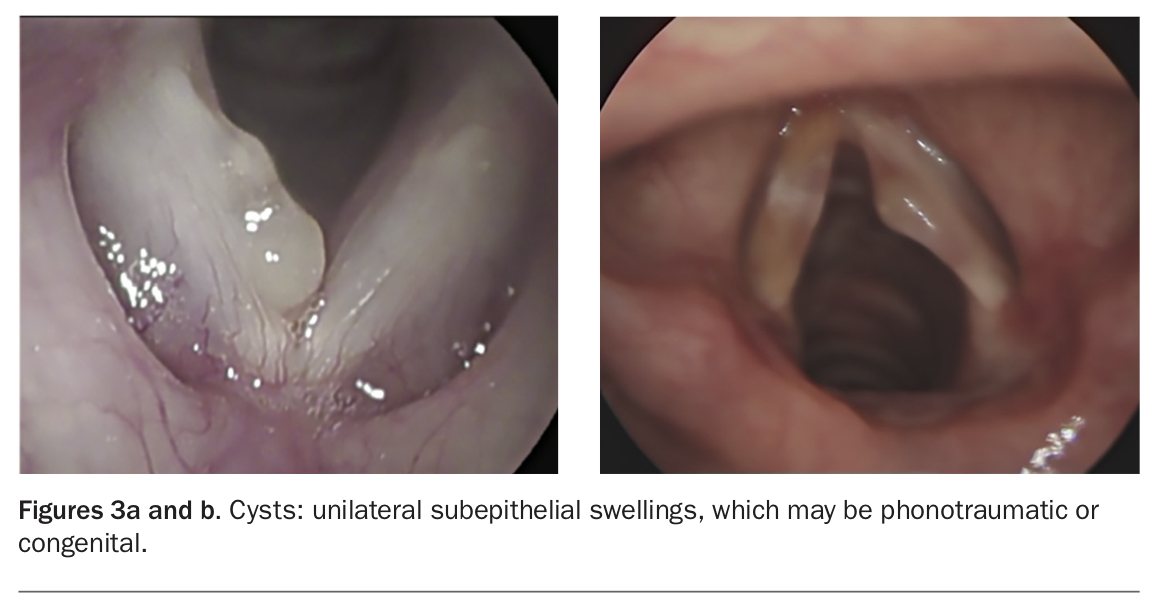
Cysts can be either epidermoid cysts (arising from epithelial cell rests found under the surface layer) or mucous retention cysts (formed due to obstruction of a mucous gland) (Figure 3). They may or may not be related to vocal misuse or overuse. If a cyst ruptures on the epithelial surface, it can form an open cyst, manifesting as a sulcus pocket that can collect inflammatory debris and exudate, causing stiffness to vocal fold vibration.
{kind=link}
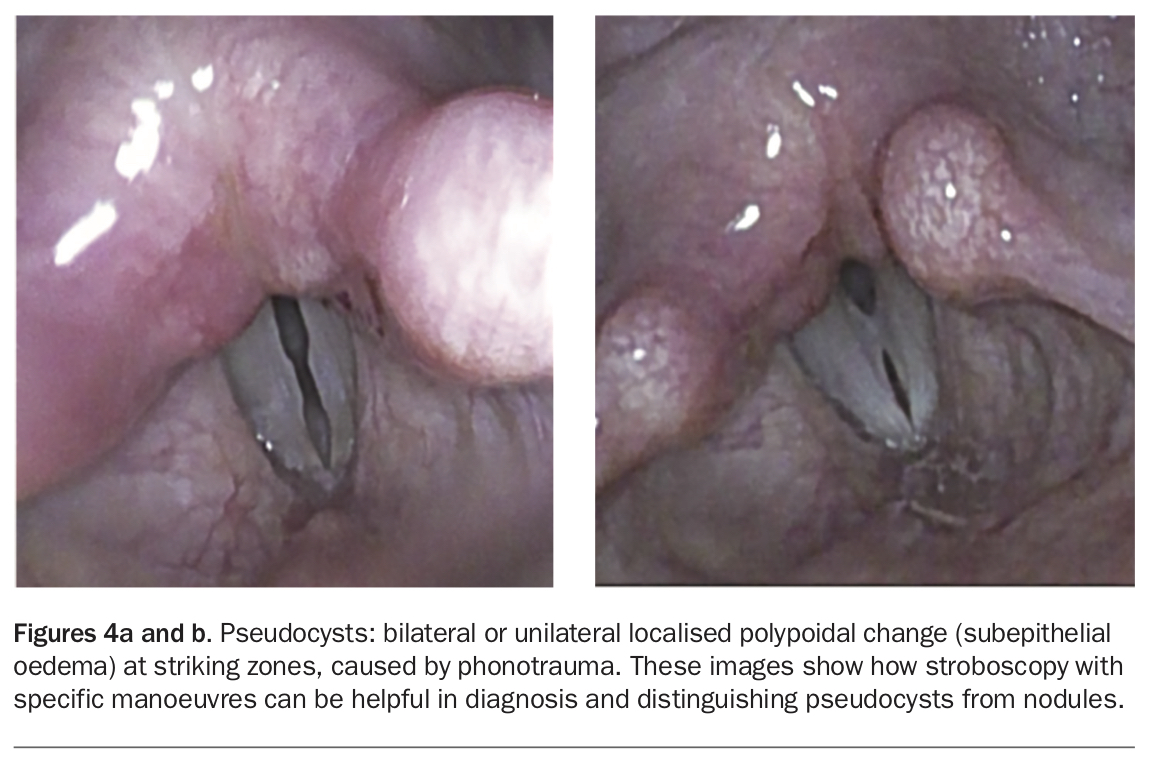
Pseudocysts are distinct entities presenting as localised subepithelial oedema, often associated with underlying glottal insufficiency (Figure 4). They can be present in professional voice users or in people with underlying vocal cord paresis (partial weakness); hence, they have also been referred to as paresis podules.7 Pseudocysts may be a precursor to nodules or polyps.
{kind=link}
Apart from these common lesions, a professional voice user is prone to scarring and fibrosis. All phonotraumatic lesions ultimately cause impairment of vocal fold vibration, leading to a hoarse or rough voice. Secondary glottal insufficiency can occur due to air escape, leading to a breathy voice. The false vocal cords above the true vocal folds try to compensate for underlying air escape, leading to inappropriate or excessive muscle tension and resulting in perilaryngeal pain.
Muscle tension dysphonia represents voice disorders characterised by excessive or inappropriate tension of the laryngeal and anterior neck muscles during phonation. In the absence of obvious laryngeal mucosal and neurological lesions, the condition is referred to as ‘primary’ and is believed to result from improper use or inefficient technique. It may also occur secondary to laryngeal problems as an attempt to compensate for inefficient closure (often known as ‘secondary’ or ‘compensatory’ muscle tension dysphonia).8
Laryngopharyngeal reflux (LPR) is a common cofactor in the hoarse patient but rarely the primary diagnosis. LPR of gastric contents can be acidic or nonacidic, and liquid or gaseous. LPR can affect the voice by causing direct laryngeal inflammation or, more commonly, by aggravating throat clearing and other hyperfunctional behaviours by way of throat irritation. Underlying hiatus hernias, oesophagitis and motility disorders may give clues to the presence of LPR, but patient-reported outcome measures, such as the Reflux Symptom Index, are the most useful clinical tools in diagnosis and management of LPR.9
Laryngeal granulomas usually occur posterior at the vocal process or arytenoid cartilage and present as unilateral tenderness and throat clearing, with or without dysphonia. LPR is most often the causative factor, although intubation can also cause this problem, especially in female patients.
Diagnosis and management
Involvement of a speech pathologist is highly desirable for treating patients with phonotraumatic lesions or hyperfunctional behaviours. Common hyperfunctional behaviours include suboptimal patterns of vocal usage (akin to inefficient running or weightlifting techniques), which cause squeezing of accessory neck musculature and creation of muscle tension to project the voice, sing or talk for prolonged periods. Cessation of smoking and vocal health measures, such as proper hydration, minimising consumption of drying agents including alcohol and caffeine, avoidance of phonotraumatic behaviour such as throat clearing and shouting, vocal warm-ups and voice rest, are recommended.10 Reflux dietary and lifestyle modification, along with antacid alginate therapy, is optimal initial conservative management for throat irritation.11 There is limited evidence for use of proton pump inhibitors in treating voice disorders.
Laryngoscopy is essential for an accurate diagnosis and is desirable before initiating empirical medical management. Beyond this, laryngeal stroboscopy allows visualisation of vocal fold mucosal wave vibration in slow motion. This helps identify nonvibratory segments of the vocal fold, asymmetries in vocal fold tension and air leakage during phonation (glottal insufficiency), guiding accurate diagnosis and optimal management. There are numerous patient-reported outcome measures (relating to voice, singing voice, reflux, cough, etc) that are useful for gauging symptom severity, triaging patients and monitoring response to treatment.
Small vocal cord polyps, nodules, varices and ectasias may respond well to conservative treatment with voice rest and speech therapy, but ongoing phonotraumatic behaviour must be dealt with to prevent recurrence. Cysts are not as responsive to conservative measures and require phonosurgery.
Scenario 2
A 65-year-old man presents with a short history of weak, breathy voice and an inability to project his voice above background noise. He has an associated history of swallowing difficulty (coughing on thin fluids) and phonatory dyspnoea (running out of breath while speaking). Differential diagnoses include:
- paralysis
- paresis
- presbyphonia (age-related voice changes)
- vocal atrophy
- sulcus and scarring
- spasmodic dysphonia.
Glottal insufficiency translates to a gap between the adducted vocal folds. Inadequate or inefficient glottal closure causes air leak, giving a breathy quality to the voice and leading to reduced maximum phonation time. Potential underlying causes include paralysis or paresis (complete or partial weakness) of one side, vocal fold bowing secondary to ageing or atrophy, and poor neuromuscular control, as seen in patients with brainstem lesions, motor neurone disease, Parkinson’s disease or myasthenia gravis. Apart from the glottic gap, high vagal damage can affect pharyngeal and supraglottic sensation, placing the patient at higher risk of dysphagia and aspiration. Lower vagal lesions can occur iatrogenically during neck, spinal or cardiothoracic surgery and usually spare supraglottic sensation. Recurrent silent aspirations may manifest as recurrent chest infection or pneumonia, with significant morbidity.12 Parkinson’s disease and myasthenia gravis can also present with glottal insufficiency and dysphagia; hence, a thorough systemic neurological examination to assess strength, tremor, coordination and gait is imperative. Note needs to be made of articulatory difficulties (e.g. slurred speech), velopharyngeal insufficiencies and regurgitation problems.
Vocal fold atrophy causes glottal insufficiency secondary to loss of muscle mass and bowing and is more common with advanced age and rapid weight loss. Essential tremor of the voice is another age-related and usually autosomal dominant inherited cause of dysphonia. It presents with an unstable tremulous voice that is best appreciated on sustained phonation and may also manifest in other parts of the body as benign essential tremor.
Non-neurological causes of a breathy, weak voice include vocal fold scarring or sulci, which can be congenital or occur secondary to phonotrauma, laryngeal surgery or radiotherapy.
Spasmodic dysphonia is a rare but debilitating voice condition. It is a focal laryngeal dystonia that is task-specific to speech and most often manifests with a tight, strained voice quality. The adductor variant of spasmodic dysphonia causes increased effort and phonation breaks while speaking, whereas the abductor variant causes breathy voice breaks. Patients may present with the classical history of experiencing improvement with the use of alcohol or anxiolytics or during singing, shouting or laughing, and aggravation during stressful situations. Vocal tremor is present in more than 40% of patients with spasmodic dysphonia.13 Some patients find that certain tactile or proprioceptive manoeuvres, such as scratching the ear – so-called sensory tricks – can improve speech fluidity. Thus, good history taking, including neurological examination and simple voice assessment tasks, can go a long way toward suggesting aetiology. Voice assessment tasks include sustained phonation to elicit tremor and to measure maximum phonation time on a sustained ‘ah’ (normally longer than 15 seconds in women and 20 seconds in men).
Diagnosis and management
Red flag signs of aspiration or swallowing dysfunction in combination with hoarseness should prompt a thorough neurological evaluation and referral to an otolaryngologist. Early referral to a speech pathologist can help with safe swallowing strategies and voice rehabilitation.
Permanent treatment of glottal insufficiency using Gore-Tex (W. L. Gore & Associates) or silicone implants can reduce air leakage, thereby improving loudness of voice and decreasing the effort required to speak. Temporary vocal fold fillers can often be given as an outpatient procedure under local anaesthesia, giving significant improvement in voice and swallow function while patients wait for recovery, which may take up to six to 12 months, assuming the nerve pathway is intact. Although implants and fillers are an option for treating patients with presbyphonia and Parkinson’s disease, the latter responds best to voice therapy.14
The gold-standard treatment for spasmodic dysphonia and essential tremor of voice remains laryngeal botulinum toxin injections, with few surgical options showing consistent, functional and reproducible results. Neurodegenerative disorders are treated in conjunction with neurologists.
Scenario 3
A 75-year-old man presents with a short history of a progressive painless roughness in his voice. An associated history of smoking, neck swelling and mild breathing or swallowing difficulty may be present. Differential diagnoses include:
- laryngeal dysplasia
- cancer
- benign tumours
- polypoid corditis.
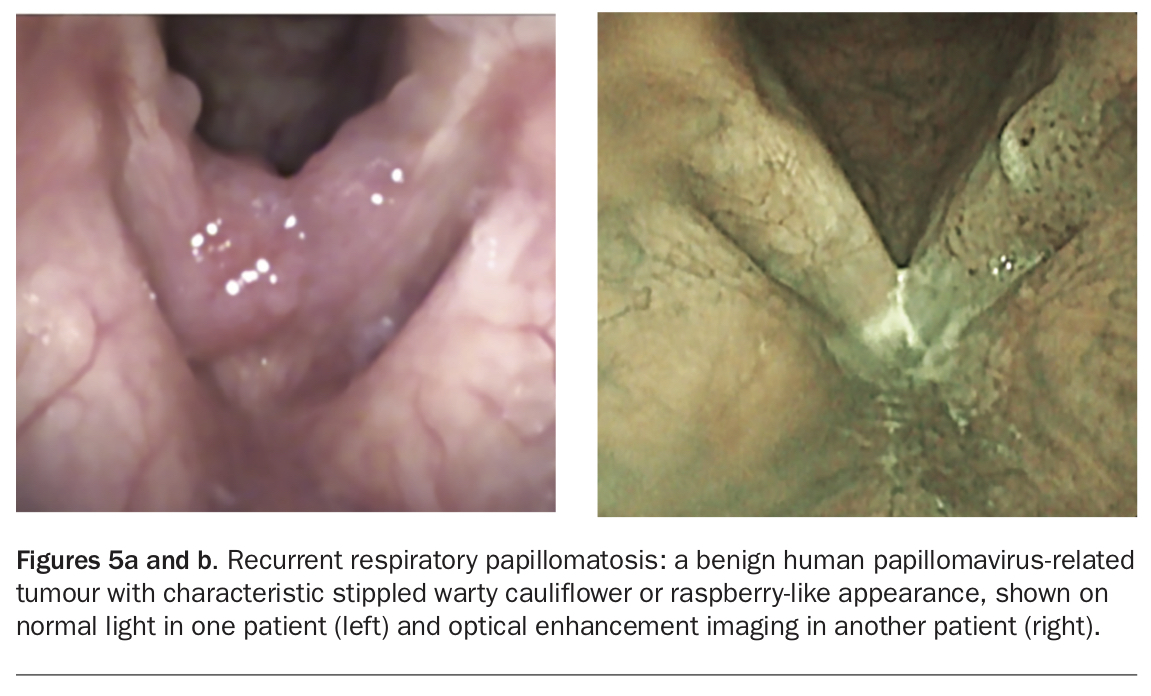
The most common tumours of the larynx are malignant squamous cell carcinomas or benign respiratory papillomatoses. Recurrent respiratory papillomatosis is a benign epithelial tumour caused by human papillomavirus (HPV), usually types 6 and 11 (Figure 5). It affects 1 to 4/100,000 people, with peaks of onset in childhood, early adulthood and late adulthood.15 The juvenile-onset variant (thought to be vertically transmitted during birth) is more extensive, multifocal and recurrent in nature and poses the danger of airway compromise. The adult-onset variant (caused by horizontal transmission of HPV between adults) is less aggressive but associated with progression to carcinoma in situ in 7% of patients and to invasive squamous carcinoma in 2%.16 On close examination, it is possible to see red pinpoint dots within the lesion, which signify blood vessels within the papilloma. Juvenile-onset recurrent respiratory papillomatosis is now on the decline in Australia after inclusion of the quadrivalent HPV vaccine in the Australian vaccination program.17
{kind=link}
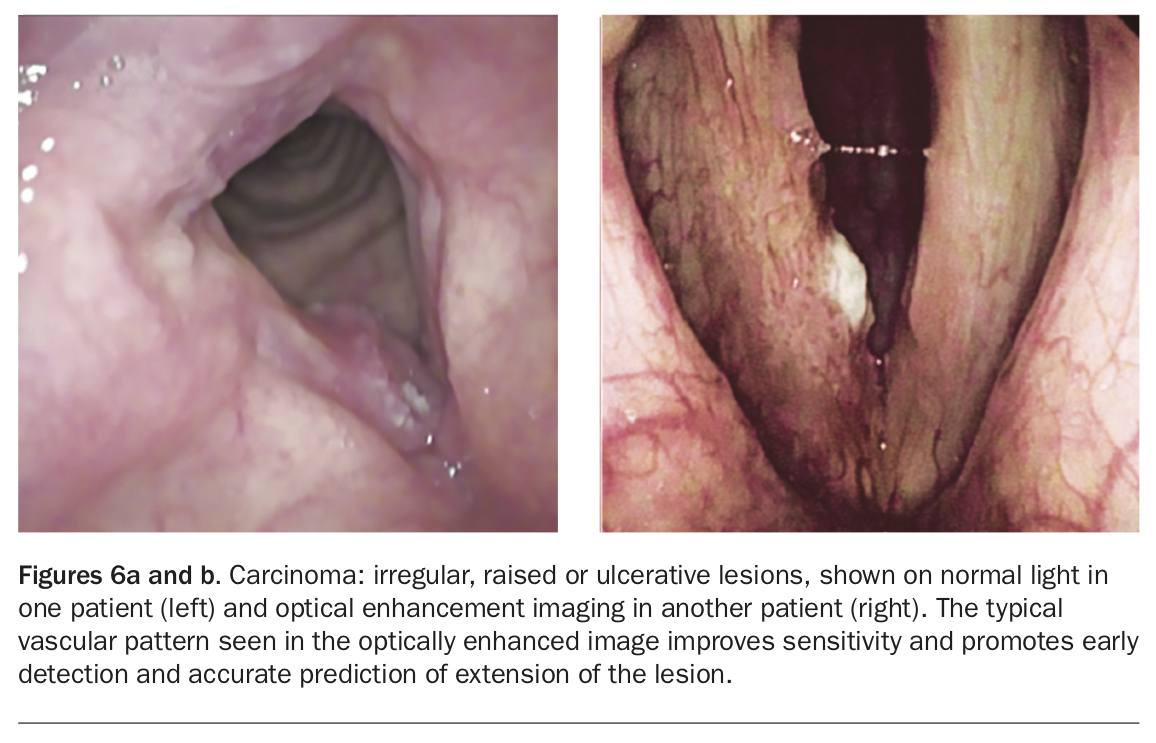
Squamous malignancies of the larynx affecting the vocal folds usually present with progressive and painless voice change. Supraglottic and pharyngeal tumours may have only mild symptoms of foreign body sensation or referred otalgia, until they grow large enough to cause dysphagia, dyspnoea or dysphonia or they metastasise to cervical lymph nodes. Subglottic tumours are less common and may present with cough or dyspnoea. Smoking and alcohol consumption are major risk factors, as is age alone. Early detection can aid early management, which translates into better treatment success and better functional voice outcomes. Modern technologies that show improved sensitivity and diagnostic accuracy and allow earlier detection and treatment, including stroboscopy and optical imaging with high-definition cameras, are generally available in dedicated laryngology centres (Figure 6).
{kind=link}
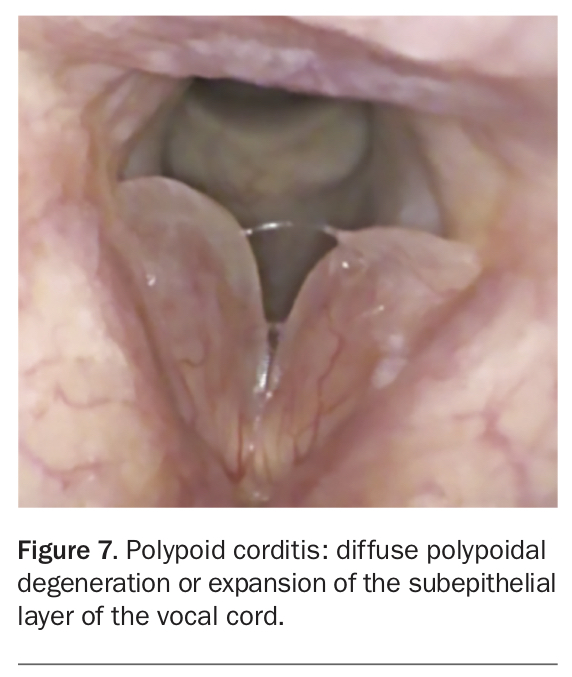
Another cause of rough voice in smokers is polypoid corditis, also known as Reinke’s oedema. As the name suggests, this represents diffuse polypoidal change in the Reinke’s space (superficial lamina propria) of the vocal cord (Figure 7). This condition classically presents in middle-aged women exhibiting phonotraumatic behaviour after exposure to irritants like tobacco smoke, leading to a peculiar low-pitched, husky voice.18 Although the polypoid change in this condition is itself benign, dysplasia is often seen in the overlying epithelium, related to smoking.
{kind=link}
Diagnosis and management
Red flags prompting immediate referral to an otolaryngologist for evaluation of dysphonia include significant smoking history, dyspnoea, dysphagia, odynophagia, otalgia and concomitant neck lump. New surgical technologies, including angiolytic lasers, have made minimally invasive and office-based treatments of premalignant lesions, benign phonotraumatic lesions and respiratory papillomatosis possible. These laser procedures are well tolerated by most patients and are associated with lower morbidity and cost to the healthcare system.
Other considerations in evaluating a hoarse patient
In general practice, the above profiles would cover about two-thirds of patients. However, for the significant number of patients who do not fit these profiles, other frequent and some uncommon diagnoses should be considered.
For patients with underlying asthma and chronic obstructive pulmonary disease treated with steroid inhalers or long-term oral steroids, myopathy or atrophy may cause voice changes. Localised immunosuppression can cause fungal or bacterial laryngitis, which will present with a hoarse voice, with or without associated pharyngitis causing dysphagia.
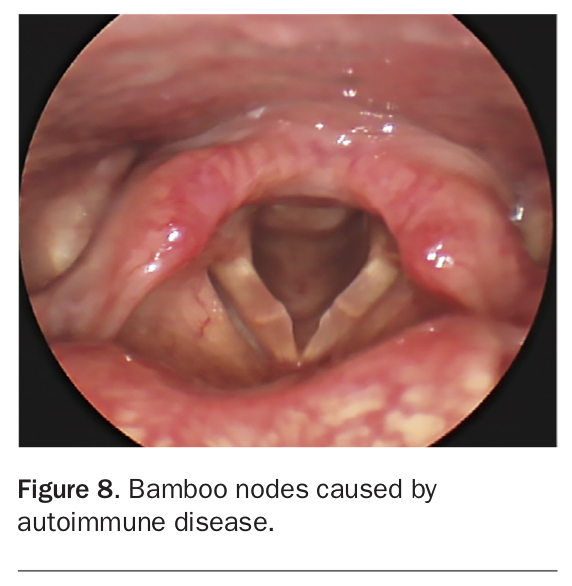
Systemic or autoimmune diseases, such as rheumatoid arthritis and systemic lupus erythematosus, may present in the larynx as submucosal thickening of the vocal cords in the form of bamboo nodes or rheumatoid nodules (Figure 8). These result in a rough and breathy voice or even cricoarytenoid joint fixation impairing vocal fold mobility. They can be medically managed with systemic steroids or vocal fold steroid injection; this should be done in a multidisciplinary fashion in conjunction with a rheumatologist. Clinicians should not routinely prescribe corticosteroids to patients with dysphonia before the larynx has been visualised.3 Sarcoidosis and granulomatosis with polyangiitis rarely affect the voice but can affect the laryngeal airway.19 The larynx is the most common location in the head and neck for localised amyloidosis, with the supraglottis being more affected than the true vocal cords. Amyloid deposits appear as nodular submucosal growths, pale to pinkish red in colour, with dysphonia being the most common symptom.19
{kind=link}
Physicians should also keep in mind various possible patterns of glottic or subglottic stenosis, which can cause voice change in a small subset of patients. Stenosis is possible after laryngeal trauma, especially with thyroid cartilage fracture and mucosal disruption. Intubation-related trauma is more often associated with posterior glottic stenosis, which can cause ulceration, adhesions or dislocations of the arytenoid cartilage and impairment of vocal fold mobility. Chemical or inhalational injuries also cause damage to the laryngeal mucosa and can predispose to stenosis in the future.
Conclusion
A hoarse voice is never normal and has an array of multiple potential aetiologies. Persistent hoarseness requires prompt evaluation, especially for professional voice users and high-risk individuals showing red flag signs, to ensure optimal outcomes. General practitioners have an important role in appropriate identification, triage and early management of patients with voice problems. Laryngoscopy with stroboscopy is the gold-standard diagnostic modality. A wide array of office-based diagnostic and therapeutic tools is now available for management of laryngeal disorders, making dealing with voice disorders less morbid and more patient friendly. MT