Tonsil and adenoid disease in childhood

Recurrent tonsillitis and sleep-disordered breathing are common paediatric presentations in general practice. GPs are well placed to identify, manage and, when appropriate, refer children with diseases of the tonsils and adenoid to help improve quality of life.
- In the paediatric population, upper airway obstruction and recurrent tonsillitis are common presentations to general practice pertaining to tonsil and/or adenoid disease.
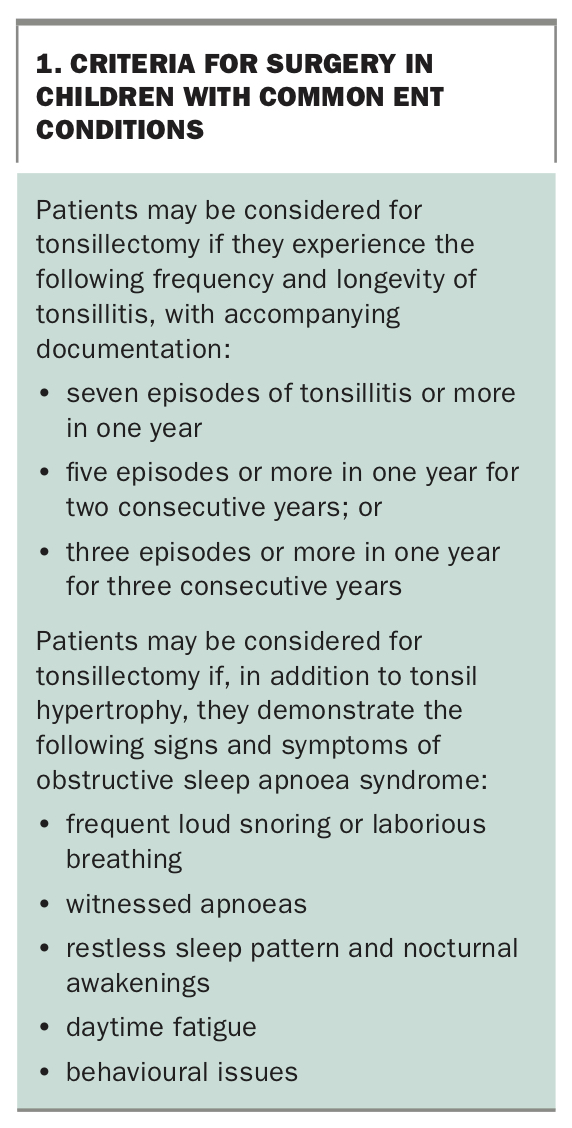
- Children with recurrent tonsillitis may be considered for surgery if frequency and longevity criteria are met and documented. Modifying factors such as febrile convulsions, antibiotic allergy and time off school may be considered in children who do not meet these criteria for surgery.
- Documenting each episode of tonsillitis in paediatric patients is recommended to help ascertain their eligibility for tonsillectomy.
- Sleep-disordered breathing describes a spectrum of upper airway breathing disorders ranging from simple snoring to obstructive sleep apnoea syndrome (OSAS).
- OSAS can severely impact on quality of life; therefore, distinguishing it from simple snoring is an important component of patient management.
- General practitioners play an important role in identifying paediatric patients with diseases that relate to the tonsils and adenoid and referring them to the ENT surgeon if needed.
In children, inflammatory and infective diseases of the tonsils and adenoid are common conditions that are managed by general practitioners and ENT surgeons. The two common presentations pertaining to diseases of the tonsils and adenoid are sleep-disordered breathing (SDB) and recurrent tonsillitis. Some children may present with both conditions.
In 2002, the Australian Institute of Health and Welfare estimated that sore throat secondary to viral or bacterial tonsillitis represented 3.7% of all visits to general practitioners in children up to 14 years of age.1 Up to 12% of children will snore at some point in their childhood and between 1 to 4% may demonstrate apnoeic episodes.2 In the period from 2017 to 2018, a total of 62,245 tonsillectomies with or without adenoidectomies were performed in the Australian public hospital system in children up to 12 years of age.3 These procedures were done for either recurrent tonsil infections or upper airway obstruction from tonsil and/or adenoid hypertrophy, and in some cases, surgery was undertaken for both indications.
In recent decades, upper airway obstruction from tonsil and/or adenoid hypertrophy has superseded recurrent acute tonsillitis as the more common indication for paediatric tonsillectomy.4 This may reflect the advent of the antibiotic era and the introduction of penicillin V in the 1960s for the management of bacterial tonsillitis. In addition, the entity of obstructive sleep apnoea syndrome (OSAS) and its potential impact on a child’s quality of life has become increasingly recognised and appreciated in recent decades, particularly with the development of polysomnography.2,4,5
This article outlines these two common presentations involving the tonsils and adenoid in children and examines management options, including the timing of referral to an ENT surgeon.
The healthy tonsil and adenoid
The palatine tonsils and nasopharyngeal tonsil (also referred to as the ‘adenoid’ or ‘adenoids’) form a circle of nonencapsulated, mucosa-associated lymphoid tissue in the upper airway. This is referred to as Waldeyer’s ring after the German anatomist who first described its embryology, anatomy and function.6 Waldeyer’s ring also includes lymphoid tissue at the tongue base (lingual tonsil) and the Eustachian tube cushions (tubal tonsils), which may be impacted by the same pathological processes that affect the palatine tonsils and adenoid.7 This ring of nonencapsulated, mucosa-associated lymphoid tissue is located in the nasopharynx and oropharynx and functions as a sieve for viruses and bacteria. It is particularly active in producing an immune response against antigens entering the upper airway in children aged between 3 and 10 years.8
The 'unhealthy' tonsil and adenoid
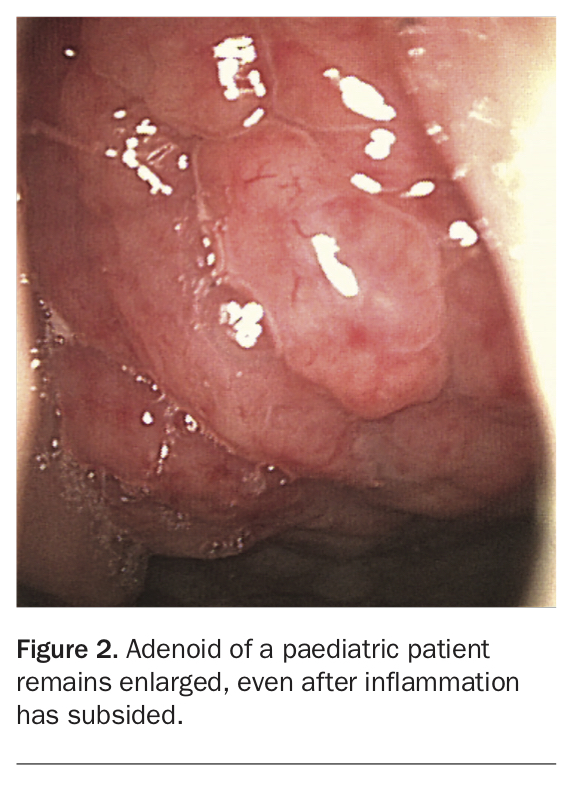
The two most common disease processes that affect the tonsils and adenoid in children are infection and inflammation. Recurrent episodes of acute tonsillitis alter the controlled process of antigen transport through the tonsillar crypts and this may affect the ability of the tonsils to afford local protection.8 The tonsils may swell up during an infective episode and may not return to their previous size (Figure 1). Similarly, the adenoid that enlarges during the inflammatory process may remain enlarged (Figure 2). Some children may have tonsil and adenoid hypertrophy without prior infection.
{kind=link}
{kind=link}
Children who experience bouts of recurrent acute tonsillitis may be systemically unwell during these episodes, whereas those with tonsil and/or adenoid hypertrophy, with or without prior infection, may demonstrate signs of upper airway obstruction like snoring and apnoea. Both groups of children may experience a reduced quality of life; therefore, considering the options for management, which may include surgery, is important to improving quality of life.
Recurrent acute tonsillitis
Sore throat as a presenting symptom can be difficult to evaluate if the oropharynx looks normal on examination. Differentiating sore throat that is secondary to inflammation of the palatine tonsils from inflammation of the posterior oropharyngeal mucosa is not always straightforward, and not all children will present with obvious signs and symptoms of tonsillitis such as sore throat accompanied by fever, odynophagia, cervical lymphadenopathy and evidence of tonsillar exudate or swelling. However, when they do present with obvious tonsillitis, the episode must be documented.
Viruses including Epstein-Barr virus, rhinovirus, respiratory syncytial virus, influenza virus, cytomegalovirus and rubeola virus have been implicated in contributing to tonsillitis by way of causing upper respiratory tract infections. Bacteria that have been implicated are Staphylococcus aureus and, notably, group A beta-haemolytic Streptococcus pyogenes (GABHS).8
Management options for tonsillitis include symptomatic measures to control fever and pain. A throat swab may be obtained. If the throat swab is culture-negative and a child continues to be unwell, in the realm of evidence-based medicine, a white cell count with differential would be ideal to confirm bacterial aetiology, pending the commencement of oral antibiotics. The antibiotic of choice should be penicillin-based, particularly in the context of a GABHS-positive throat swab. If a child is allergic to penicillin, a cephalosporin or a macrolide antibiotic such as erythromycin may be used.
The American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) has updated the clinical practice guideline for the management of tonsil disease in children aged 1 to 18 years.8 These guidelines are relevant to and supported in Australian ENT practice. Since the 1980s, the AAO-HNS has advocated for the documentation of all tonsillitis episodes in paediatric patients so that a record of frequency and longevity is available to help determine their eligibility for tonsillectomy (Box 1).8,9
{kind=link}
If a child does not meet the frequency and longevity criteria for recurrent acute tonsillitis, the following modifying factors allow for flexibility in clinical judgement on the part of the general practitioner or ENT surgeon with regard to tonsillectomy:8
- febrile convulsions from tonsillitis-associated fever
- the presence of antibiotic allergies
- systemic unwellness during each episode of tonsillitis
- time off school
- need for hospitalisation
- the potential for nonsuppurative complications from GABHS such as acute glomerulonephritis or acute rheumatic fever.
To date, the role of long-term, low-dose prophylactic antibiotics remains unclear.10 If surgery must be delayed, long-term, low-dose penicillin-based antibiotics have been anecdotally prescribed in the absence of a known penicillin allergy. Otherwise, the option of surgery is the likely endpoint of management in children with recurrent tonsillitis. Referral to the ENT surgeon should be considered if the frequency and longevity criteria have been met or when modifying factors are present.
Sleep-disordered breathing
Sleep-disordered breathing (SDB) is a term that is used to describe the spectrum of upper airway breathing disorders that range from simple snoring to OSAS.11 Parents and caregivers are typically concerned if a child's snoring becomes frequent and loud, especially when compared with that of other children. In healthy children, the most common cause of OSAS is hypertrophy of the adenoid and/or tonsils.12
Presenting symptoms of SDB may range from intermittent loud snoring to nocturnal awakenings, witnessed apnoeas, enuresis, daytime fatigue and challenging behaviour. The parent or caregiver may also report laboured breathing during sleep, as well as choking or gasping episodes.2 The distinction between simple snoring and OSAS is crucial, as there is potential for a child with OSAS to develop pulmonary hypertension, growth retardation and impaired cognition; underperform at school; and have poor quality of life.2,8,11-13
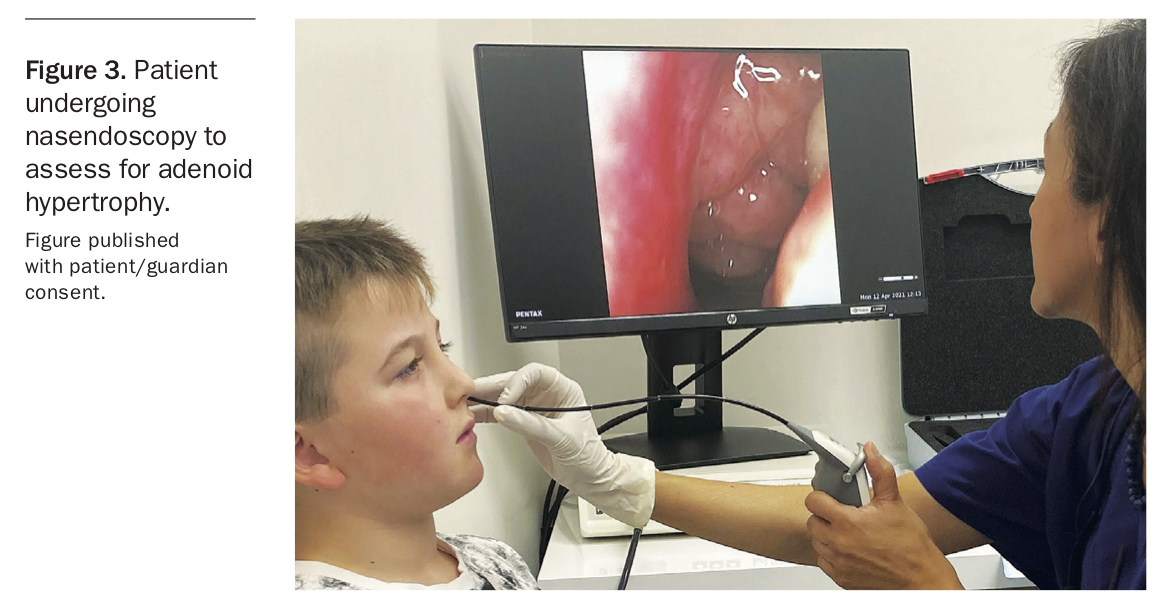
Although not validated, smartphones have proven useful for parents or caregivers to take recordings of their child’s sleep. These recordings may contribute to a confirmation of potential upper airway obstruction at the time of consultation if the child demonstrates loud snoring or laborious breathing, increased chest movements and evidence of apnoeas on audio or video. Physical examination may reveal large tonsils. If the tonsils are small, the adenoid size should be assessed for hypertrophy by nasendoscopy (Figure 3).
{kind=link}
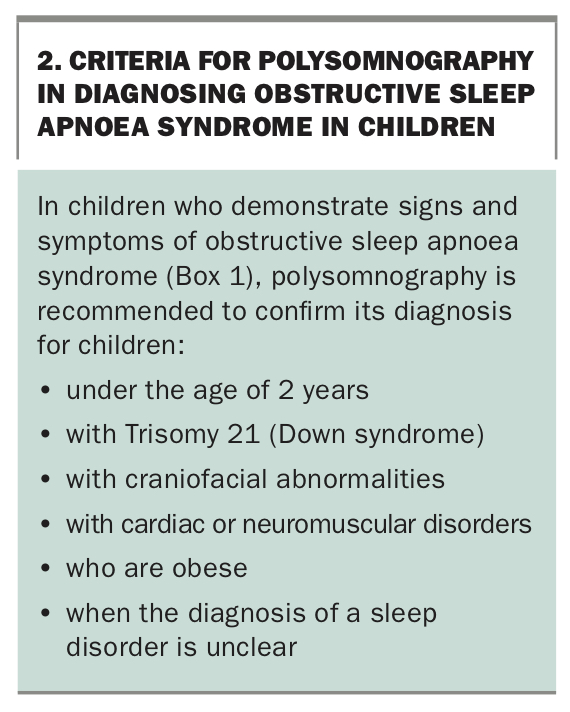
Polysomnography is the gold standard for the diagnosis of OSAS and is helpful to confirm or exclude OSAS as the cause of a child’s disturbed sleep pattern in the absence of tonsil and/or adenoid hypertrophy.8,11-13 It is a valuable tool to identify and quantitate the severity of apnoeas in children under the age of 2 years, those with craniofacial abnormalities and cardiac or neuromuscular disorders and those who are obese (Box 2).8 The results from polysomnography can determine the requirement for pre- and postoperative continuous positive airway pressure and, importantly, whether a child should be managed in a tertiary institution.
{kind=link}
In children with signs and symptoms of OSAS with adenoid and/or tonsil hypertrophy, the option of surgical removal of the tonsils and adenoid becomes the endpoint of management and referral to the ENT surgeon is recommended.
The unilaterally enlarged tonsil
A unilaterally enlarged tonsil may be of concern as lymphoma is a key differential diagnosis. The absence of enlarged lymph nodes in the neck, axillae and groins in association with a normal abdominal examination does not exclude lymphoma, and blood tests, in particular a white cell count with differential and lactate dehydrogenase test, and consultation with, or referral to, a paediatric haematologist, may be undertaken. If physical examination and blood tests are normal, a period of observation and surveillance of any change in size of the unilaterally enlarged tonsil may be acceptable. The otherwise well child with a normal physical examination and blood test results may have signs and symptoms of OSAS, thus fulfilling the criteria for tonsillectomy (Box 1). The unilaterally enlarged tonsil would be sent for flow cytometry and histopathology at the time of tonsillectomy to confirm the absence of serious pathology.
Surgery
If a child meets the criteria for surgery, complete tonsillectomy with inclusion of the tonsil capsule has been the popular choice of ENT surgeons for most of the second half of the twentieth century.14 However, this procedure, also known as extracapsular tonsillectomy, is associated with significant morbidity after surgery, in particular haemorrhage.15-17 Haemorrhage after surgery in children is concerning given their lower baseline blood volume compared with that of adults.
It is perhaps not surprising that ENT surgeons are re-exploring a historical tonsil operation that involves partial tonsil removal in children presenting with OSAS secondary to tonsil hypertrophy.18,19 The aim of this procedure is to reduce tonsil size within an intact capsule, in order to decrease upper airway obstruction. Capsule-sparing surgery, also referred to as intracapsular tonsillectomy or tonsillotomy, conceptually lends itself to lower postoperative haemorrhage rates than extracapsular tonsillectomy given the theoretical lower likelihood of breaching the wider-calibre blood vessels to the capsule, which remains intact in this operation.18 Intracapsular tonsillectomy has been demonstrated to be associated with low rates of postoperative haemorrhage and pain.18-26 However, this technique presents a dilemma, namely that of tonsillar regrowth with potential requirement for revision tonsillectomy.27,28
Intracapsular tonsillectomy is currently not included in the AAO-HNS guidelines.8,27 Data on the comparative effectiveness of intracapsular tonsillectomy compared with extracapsular tonsillectomy to manage paediatric OSAS remain limited, as is the evidence for long-term outcomes with regards to tonsillar regrowth and revision tonsillectomy.28 Nevertheless, intracapsular tonsillectomy may be an appropriate option in certain clinical contexts. Examples include in young children who may need emergent surgery for OSAS, children with developmental delay who may not be able to comply with oral intake after surgery and, importantly, children who live in remote areas who may have been denied surgical management in previous times because of the threat of haemorrhage after surgery from traditional extracapsular tonsillectomy.29
Children in remote areas
There are state- and territory-based outreach programs that provide consulting clinics for children to be assessed for disorders of the ears, nose and throat by participating ENT surgeons. Typically, when a decision is made to undertake a tonsillectomy, a child will be offered a waiting list position at an appropriate hospital with a formalised service from ENT surgeons and paediatric-trained anaesthetists who are supported by experienced nursing and medical staff. Local accommodation is provided for the patient and their family for the two-week period after traditional extracapsular tonsillectomy. This facilitates the safe and timely management of postoperative complications such as secondary haemorrhage, as the patient can be returned to hospital without delay. If this arrangement is not possible, then surgery should not proceed. There is scope for further research into the use, efficacy and safety of the intracapsular method of tonsil surgery in the context of outreach programs.
What about vaccination?
The Australian immunisation program includes vaccination against viruses that have potential to cause viral tonsillitis by way of infecting the upper respiratory tract. The influenza and measles vaccines are examples. To date, there is no available vaccine against GABHS.
Conclusion
Tonsil and adenoid disease in childhood is relatively common. It can manifest as an infective and/or obstructive process, or both. Early recognition and management of diseases of the tonsils and adenoid will allow an affected child to thrive and enjoy an improved quality of life. The general practitioner is typically the first point of contact for these patients and, therefore, plays a crucial role in the diagnosis, management and, if required, referral to the ENT surgeon. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.