Managing patients on a vegetarian or vegan diet

Dr Moghaddas is a Fellow in the Department of Clinical Nutrition and Metabolism, Monash Medical Centre, Melbourne, Vic.
Dr Marks is Unit Head in the Department of Clinical Nutrition and Metabolism, Monash Medical Centre, Melbourne, Vic.

Increasing numbers of people are following vegetarian and vegan diets in which some key nutrients may be deficient. Screening for common deficiencies should be considered, as well as other potential causes or contributors.
- Vegetarian and vegan diets can provide adequate nutrition but may require additional planning, particularly for those transitioning to such diets for the first time.
- Assessing whether nutrition is adequate is particularly important for vegans and for patients during pregnancy and while breastfeeding due to increased requirements.
- It is important to screen for common nutrient deficiencies (in particular vitamin B12 deficiency in vegans, given its prevalence).
- All. deficiency may not be due to diet alone; alternative causes or contributors should be considered.
- For those eating a more limited range of foods, a complete multivitamin can help meet daily requirements, but specific supplementation may be required.
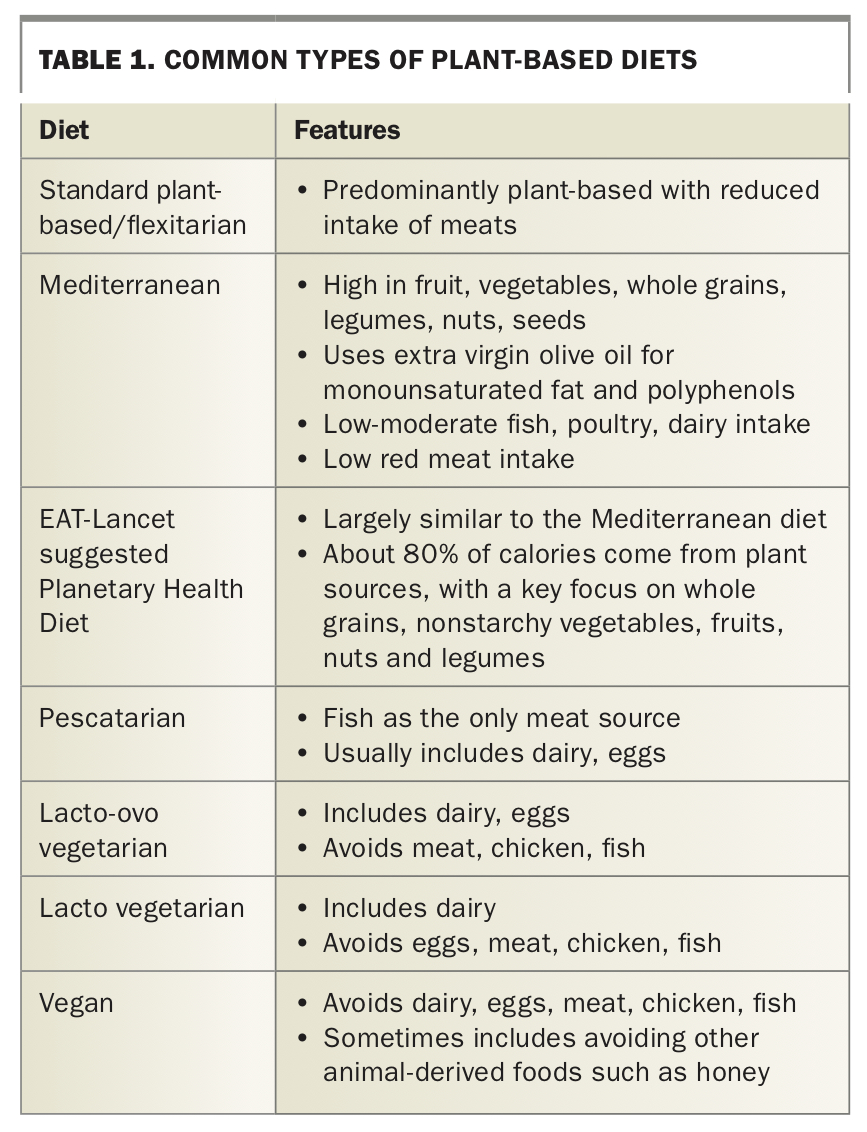
Plant-based diets have continued to garner increased interest and be adopted by the general population due to their well-established health and environmental benefits.1-3 Plant-based diets reduce or completely avoid the consumption of foods sourced from animals. This encompasses a range of individual diets, which are summarised in Table 1. From a global perspective, the EAT-Lancet commission highlights the benefits of a larger scale adoption of a plant-based diet, estimating that up to 24% of total deaths among adults could be prevented while also improving planetary health through a reduction in greenhouse gas emissions and more efficient cropland and water usage.3 Overall, the key to any healthy plant-based diet is the focus on nutrient-dense plant foods that are generally lower in saturated fat and the avoidance of refined carbohydrates. This article focuses on managing patients on vegetarian and vegan diets rather than a flexitarian diet.
{kind=link}
The current numbers of Australians eating a vegetarian or vegan diet are not well established. The last national government- conducted survey specifically looking at special diets was undertaken in 1995.4 Of all respondents, 3.7% reported being on a vegetarian diet, with a higher proportion being female (4.9% vs 2.6%), and of these, over 5% were aged 16 to 44 years. More recently, the Roy Morgan research group estimated that 12.1% of the population in 2018 ate a mostly vegetarian diet, up from 11.2% in 2014 and 9.7% in 2012, with the largest demographic being young, educated people.5 Perhaps a greater global awareness, concern for animal welfare, and/or easy access to like-minded people and groups through social media, rather than health or religious reasons, drives this.
For the purpose of this article we will focus on some key nutrients that may be deficient in a vegetarian or vegan diet. Protein, iron, zinc, vitamin B12, calcium, iodine and polyunsaturated fatty acids (PUFAs) are a particular focus.
Protein
All protein within the human body serves a function and none is stored as energy reserves, unlike fat and carbohydrates. Certain amino acids are defined as essential, meaning that the body cannot synthesise these and they are required in the diet. Adequate protein and energy intake is important to avoid catabolism and breakdown of muscle. Reassuringly, protein deficiency is relatively rare outside of those on markedly restricted diets, the elderly or those with chronic illnesses.
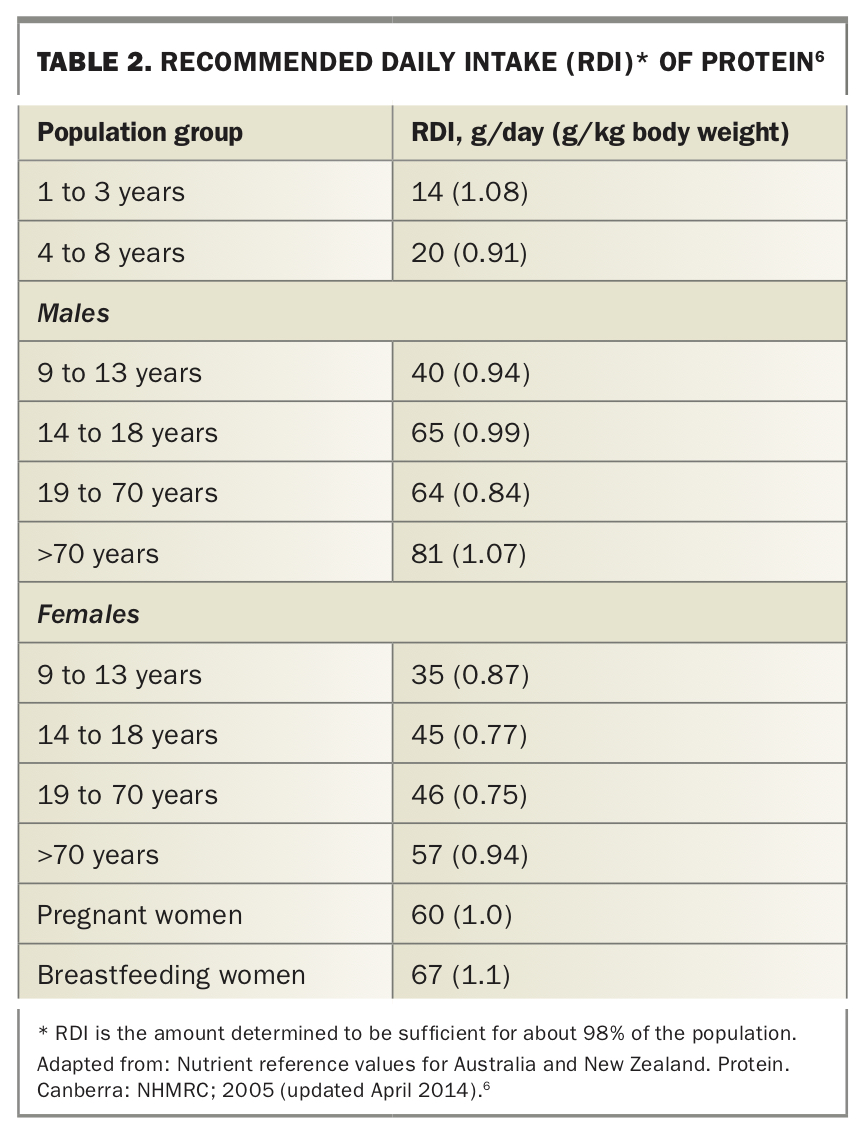
The current nutrient reference values for Australia and New Zealand propose that the acceptable range for protein is 15 to 25% of daily energy intake to also ensure adequate micronutrient ingestion (minimum amount for protein alone is about 10%). This equates to roughly 0.8 to 1 g/kg of body weight, and weight-based dosing is more accurate, particularly in those on reduced-calorie diets (Table 2).6 It is important to note that all elderly patients and patients with chronic disease need to meet a higher protein intake to minimise age-related sarcopenia, with evidence supporting an intake above current Australian recommendations at 1 to 1.2 g/kg for the healthy older patient and up to 1.5 g/kg in those with chronic disease and higher risk of malnutrition.7-10
{kind=link}
Vegetarians and vegans on average have lower protein intakes than omnivores, although most still meet the target intake and sarcopenia is not increased.11-13 Vegans, and younger women generally, tend to get 10 to 15% of daily energy from protein.
There is a difference in the quality of protein available in different foods. Animal proteins (including dairy, eggs) provide a large amount of all essential amino acids. Of plant-based protein sources, soy-based proteins are nutritionally complete;14 however, other sources do not have all the essential amino acids in sufficient quantities.15 Vegetarians should be encouraged to eat a variety of protein-rich foods to ensure they are getting all essential amino acids and sufficient trace elements. Incorporating soy products including soy milk and tofu, whole grains, legumes and nuts allows vegetarians to meet their target intake; and for lacto-ovo vegetarians the use of dairy and eggs in the diet makes this somewhat easier to achieve (see Table 3 for protein content of some common foods16). Protein supplementation is usually not required.
{kind=link}
Iron
Iron is the most abundant trace element in the human body and serves a vital role in the transport of oxygen around the body via haemoglobin. About 60% of iron is within haemoglobin and 25% is stored as ferritin and haemosiderin, mainly in the liver. The remainder has important functions in myoglobin and cellular activities.17
Absorption
Iron stores are tightly regulated through efficient recycling of iron in haemoglobin and intestinal absorption.18 Men both absorb and excrete (via intestinal cells sloughing away) about 0.8 mg/day of iron, whereas menstruating women need to absorb up to 1.4 mg to cover menstrual losses.17
Iron in the diet is present as haem iron and nonhaem iron. Haem iron is found only in meat and accounts for 30 to 70% of the iron content of meat.19 It is the most readily absorbed form, with 15 to 35% being absorbed. In contrast, 10% or less of nonhaem iron is absorbed.20,21 In a standard diet, haem iron accounts for up to 40% of all iron absorbed despite making up a small percentage of iron intake.4
The lower bioavailability of nonhaem iron is due to the requirement for ferric iron to be reduced to ferrous iron before being absorbed. In some plant foods, absorption is further impaired by the presence of inhibitors such as phytate and polyphenols. There are many enhancers of nonhaem iron absorption in plant-based foods, including vitamin A, beta-carotene and organic acids, of which vitamin C is the most potent enhancer.21-23 Vitamin C is involved in the reduction of ferric to ferrous iron, aiding absorption of nonhaem iron while also counteracting the common dietary inhibitors.21,23 Absorption of nonhaem iron is also increased in response to iron deficiency, largely through the downregulation of hepcidin.24
Interestingly, some studies have shown haem iron to be associated with an increased risk of coronary artery disease and metabolic syndrome.25-27 It is thought that haem iron can induce oxidative stress and lipid peroxidation; however, it should be noted that the deleterious effects of haem iron appear to mostly occur in the context of red meat, with its associated saturated fat, nitrate and cholesterol.28
Requirements
The amount of iron absorbed from food is lower for those eating a vegetarian diet than those incorporating meat products. It is estimated that for those eating a standard diet 15 to 18% of dietary iron is absorbed, whereas for a healthy vegetarian diet rich in cereals and vitamin C this is closer to 10%. Of note, in an unbalanced vegetarian diet low in vitamin C, iron absorption can be as low as 5%.29
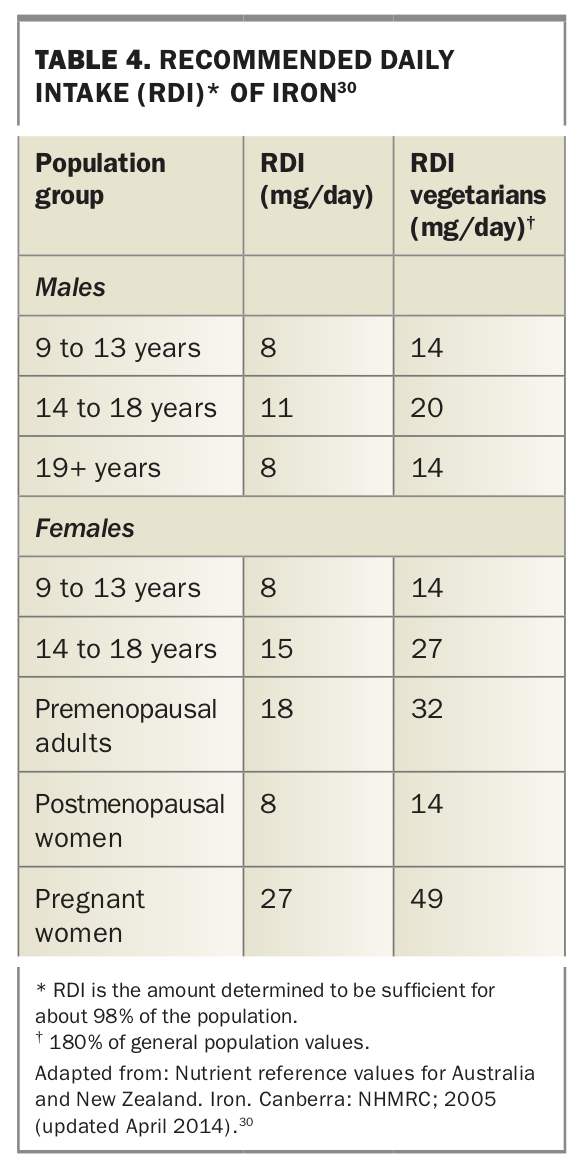
The current recommended daily intake (RDI) for iron is summarised in Table 4;30 and the iron content of some common foods is shown in Table 3.
{kind=link}
Deficiency
Iron deficiency is one of the most common nutrient deficiencies and can occur to various degrees, ranging from reduced iron stores to functional deficiency and iron deficiency anaemia. Iron deficiency can present in a variety of ways depending on the level of depletion and associated anaemia. Even without accompanying anaemia and its associated symptoms, iron deficiency is commonly associated with fatigue, weakness, muscle cramps and restless legs. These symptoms improve quickly once iron stores are replaced.
The most common cause of iron deficiency is menstrual blood loss, as 1 mL of blood contains 0.5 mg of iron. Young women are most at risk of iron deficiency due to the increased demand for iron while growing combined with menstrual loss.31 Women with menorrhagia are at highest risk as they lose in excess of 40 mg of iron a month.32 People on vegetarian and vegan diets tend to have lower baseline ferritin levels so are more prone to iron deficiency secondary to menstrual loss, particularly if eating a diet with less cereals and grains.11,18,20,33,34
Although low dietary iron intake is a risk factor for iron deficiency, it should be noted that iron deficiency usually only occurs in those with a predisposing risk factor such as menstrual blood loss, pregnancy or dialysis. It is much less common for men over 16 years and postmenopausal women to develop iron deficiency, and even in other women and adolescent girls it is important to exclude other causes.
As a minimum, it would be prudent to screen for coeliac disease and take a history to exclude overt gastrointestinal pathology. If iron deficiency, and in particular iron deficiency anaemia, occurs in men or postmenopausal women, or is recurrent in women without menorrhagia, there should be a low threshold to investigate for gastrointestinal (GI) pathology. This can first be done noninvasively via faecal occult blood testing and Helicobacter pylori stool antigen testing but should progress to endoscopic evaluation to exclude an occult GI malignancy. Studies have shown that up to 20% of patients with definite iron deficiency anaemia have a GI malignancy or high-risk adenoma identified on endoscopic evaluation, with men over 18 years and women over 45 years together having the highest incidence, at 27%.35
Zinc
Zinc is a vital trace element and the second most abundant after iron, with the body containing on average 1.5 g to 2.5 g, although less than 1% of the body’s zinc supply is in plasma.36,37 Zinc is involved in a wide range of cellular processes and plays key roles in growth, tissue repair and wound healing in addition to metabolism and immune function.38,39
Absorption
Zinc is primarily absorbed via the proximal small bowel, and to a lesser extent via the ileum and colon. Only 20 to 40% of dietary zinc is absorbed. Similarly to iron, zinc absorption is inhibited by phytate found in plant foods, particularly unrefined cereals, legumes and nuts;40 however, this can be overcome partially by using certain food preparation techniques, such as soaking dried legumes and sprouting some legumes and consuming fermented soy foods.41 Plasma zinc levels are tightly regulated through reduced endogenous zinc losses (via the GI tract and, in severe deficiency, urine) and increased gut absorption in response to low zinc levels.42
Requirements
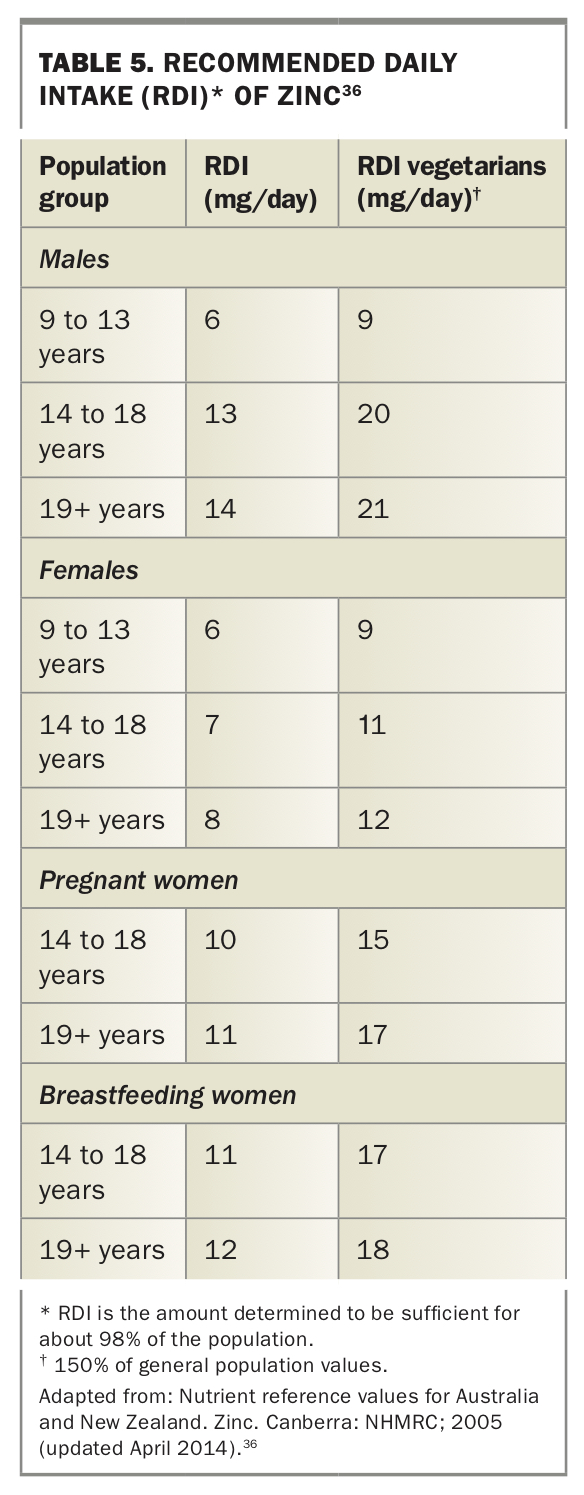
Zinc is available from both animal and plant food sources. Meat, fish, poultry and cereals are the major dietary contributors. Due to the higher phytate content in the diets of vegetarians and vegans, the RDI is 50% higher for vegetarians than nonvegetarians, at 12 mg/day for women and 21 mg/day for men (Table 5).36
{kind=link}
Inadequate dietary zinc intake is a common problem among all people regardless of the specific diet followed. It has been shown that over 50% of men and women have intakes below the RDI.43,44 Dietary zinc intake is often similar between vegetarians and nonvegetarians; therefore, vegetarians meet a lower percentage of the RDI that is specific to them.44 Nevertheless, people on well-planned vegetarian and vegan diets do not appear to have lower serum zinc levels than omnivores.44,45 Key dietary sources for vegetarians and vegans are highlighted in Table 3.
Deficiency
Zinc deficiency can manifest in a wide variety of ways. In younger populations, dietary deficiency can impair growth velocity and result in delayed sexual maturation. In addition, zinc deficiency can result in impaired wound healing, immune dysfunction, altered taste and hair loss.
Overt dietary zinc deficiency in the absence of marked dietary restriction is uncommon.46 The most common causes of zinc deficiency are malnutrition and malabsorptive states (e.g. inflammatory bowel diseases, short gut syndrome, pancreatic insufficiency, post gastric bypass). In addition, pregnancy and breastfeeding increase the risk of zinc deficiency.46
Due to the nonspecific signs of zinc deficiency, there should be a low threshold to consider this in high-risk populations. Serum zinc measurement does not always correlate with total body stores, particularly in the presence of inflammation or low albumin. Nevertheless, a normal serum zinc level can be reassuring. As zinc is relatively safe in doses up to 100 mg/day and low cost, in patients in whom there is concern for zinc deficiency, it is not unreasonable to provide supplementation and assess for symptom improvement over time.47 For those who may not have adequate dietary intake, a multivitamin containing zinc is likely to be sufficient supplementation.
Vitamin B12
Vitamin B12, also called cobalamin, is an essential, water-soluble vitamin that plays a vital role in the formation of haematopoietic cells and myelin and, in conjunction with folate, DNA synthesis.
Absorption
Vitamin B12 in food is protein-bound and is dissociated by stomach acid and pepsin. The dissociated B12 is subsequently bound by R-binders in saliva before being transported to the duodenum where pancreatic proteases cleave the R-B12 compound, allowing vitamin B12 to bind to intrinsic factor, which is itself released by gastric parietal cells. Once bound to intrinsic factor, vitamin B12 can be absorbed in the ileum.48,49
It is thought that active intestinal absorption is limited to 1 to 2 mcg per meal.50 The rate of B12 absorption is inversely proportional to the amount ingested and ranges from 11% for liver to over 60% for chicken.51 Some B12 can be absorbed passively without the need to bind intrinsic factor although this occurs at an inefficient rate of less than 1%. High-dose oral supplementation takes advantage of passive absorption and as such can be used in people who are deficient in intrinsic factor such as those with pernicious anaemia.52
Requirements
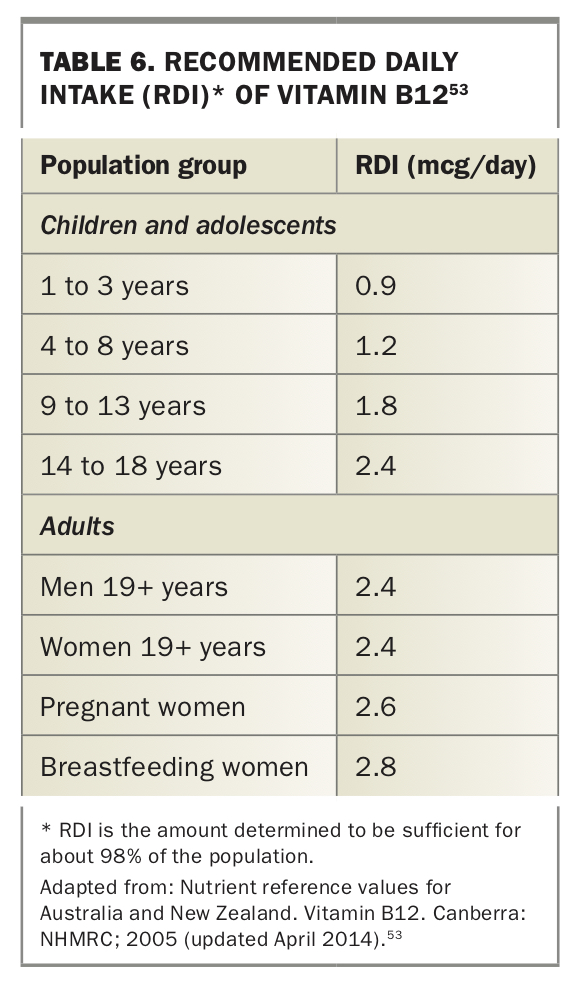
The current RDI for vitamin B12 is 2.4 mcg and is the same for all adults regardless of age. Higher levels are required during pregnancy and lactation (Table 6).53 The intake recommended for the elderly is the same despite some evidence to suggest that B12 deficiency is increased in this group, with a large study showing 5% of people over 67 years of age had overt vitamin B12 deficiency.54
{kind=link}
Vitamin B12 cannot be synthesised by humans and is found exclusively in animal products and thus is a major concern with regard to vegetarian and, especially, vegan diets. One study identified that more than 50% of those on a vegan diet and 7% of those on a vegetarian diet had vitamin B12 deficiency. In contrast, only 0.2% of nonvegetarians were vitamin B12 deficient.55 There are only limited vegan-friendly products fortified with vitamin B12 in Australia, the most accessible being fortified soy milk (Table 3).
Deficiency
The most well-known manifestation of B12 deficiency is megaloblastic anaemia, in which there is nuclear cytoplasmic dyssynchrony and abnormal erythroid precursors on blood film. In the absence of a blood film, macrocytosis with a raised mean cell volume may be noted. However, it is not uncommon for B12 deficiency to present without anaemia. Demyelination due to instability of myelin sheaths can result in peripheral neuropathies and neuropsychiatric abnormalities. These can range from very subtle (only elicited through dedicated examination) to overt. It is crucial that B12 deficiency is detected early and treated aggressively, as neurological damage can be irreversible if delayed.49,56
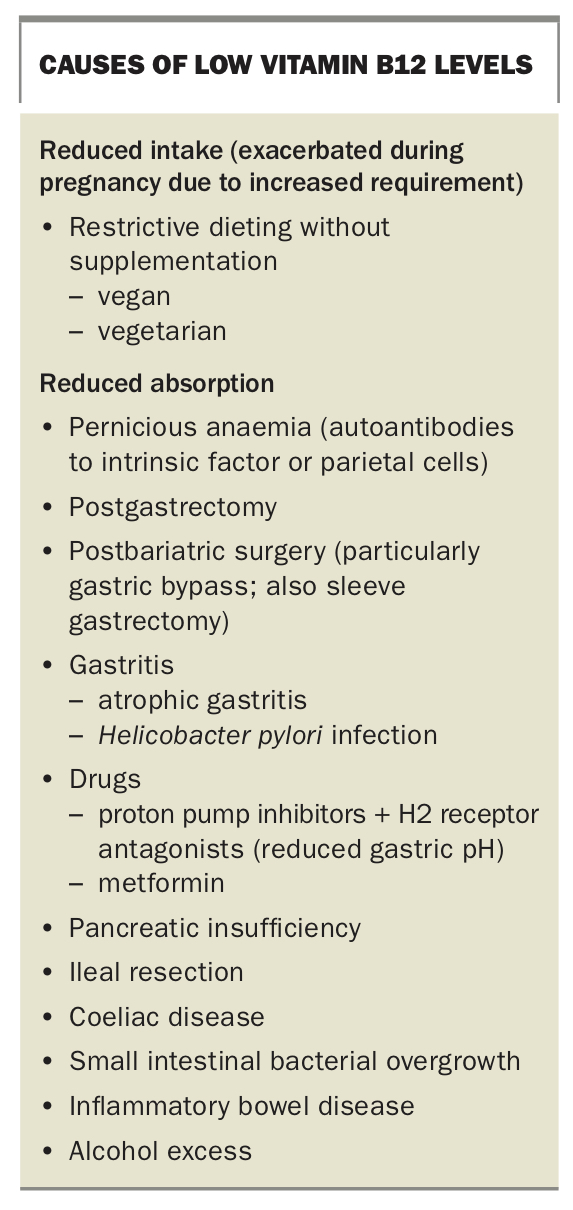
There are several causes of B12 deficiency, and these can be broadly broken down into reduced intake and reduced absorption (Box). ‘Food cobalamin malabsorption’ describes B12 deficiency despite normal dietary intake and is related to the inability to dissociate B12 from protein in the stomach. This is more often seen in the elderly population and is commonly associated with conditions reducing the acidity of the stomach, such as atrophic gastritis, and with long-term antireflux therapy.49,57,58
{kind=link}
Approach
It is reasonable to test total vitamin B12 levels yearly in those on vegan and vegetarian diets, as well as holotranscobalamin level if vitamin B12 level is low or borderline. Testing is currently funded by Medicare.
In patients with suspected or confirmed B12 deficiency, a thorough examination should be performed to establish whether there are any baseline signs of neurological compromise such as peripheral neuropathy, which may present subtly. Folate and vitamin B12 testing are generally ordered together, although folate level is rarely low in those with dietary B12 deficiency, owing to its abundance in plant foods. Folate deficiency is generally associated with malabsorptive states.
People on a vegan diet can only ingest sufficient vitamin B12 by supplementing their diet with adequate amounts of fortified soy products; those on a vegetarian diet are able to ingest some vitamin B12 from dairy and eggs.
Given the safety and low cost of supplementation, it is reasonable to suggest oral vitamin B12 supplementation to all vegan patients and to vegetarians who have minimal dairy or eggs.
Calcium
Calcium is vital for bone health and cellular functions, particularly neuromuscular and cardiac functions. Most calcium is stored in bone. Plasma levels are closely regulated by a variety of factors with the key regulators being parathyroid hormone and vitamin D. Calcium levels are regulated via intestinal absorption, bone resorption/formation and reabsorption from and excretion in urine.
Absorption
Dietary calcium is primarily actively absorbed in the duodenum and proximal jejunum, and a smaller amount is absorbed passively throughout the length of the bowel.59 Calcium absorption in the gastrointestinal tract is dependent on activated vitamin D. Absorption may be reduced by binding to certain anions, including oxalates and phytates, and forming insoluble salts. Calcium absorption from foods rich in oxalic acid (such as spinach, beans) or phytic acids (seeds, nuts, grains) can be markedly reduced. Absorption from soy milk is often close to that from cows milk, at about 30%, but is up to 50% from kale and bok choy and as low as 10% from foods such as spinach.60 In addition, some calcium is lost via secretion into stool. Consequently, the net dietary calcium absorbed may be only 10 to 20% of the ingested amount.61
Requirements
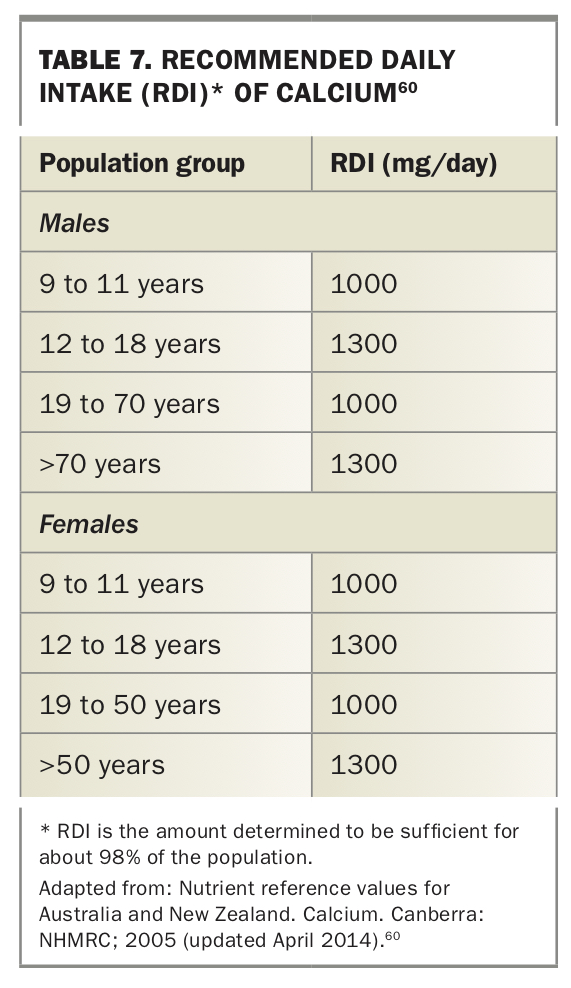
Calcium is predominantly found in dairy-based foods and to a lesser extent in legumes, certain nuts, fortified soy beverages and breakfast cereals. Although plant-based diets may affect calcium needs due to the relatively high oxalate and phytate contents, the recommended daily intakes are sufficient to remain the same regardless of diet (Table 7).60
{kind=link}
Vegetarians generally have relatively similar intakes to omnivores. Vegans tend to have significantly lower intakes due to a lack of dairy; however, chia seeds, soy milk, tofu, kale and bok choy are good vegan sources of calcium.62 Key dietary sources of calcium for vegetarians and vegans are highlighted in Table 3.
Calcium deficiency and bone health
It is important to note that due to the efficiency of calcium regulation, low dietary intakes will not manifest as hypocalcaemia in the absence of another abnormality such as significant vitamin D deficiency, hypoparathyroidism or drug side effects (most commonly with bisphosphonates, denosumab).
Nevertheless, bone health is of significant concern. Both vegetarian and vegan diets have been shown to be associated with reduced bone mineral density (BMD) in those aged over 50 years. Vegans have a more pronounced average reduction in BMD. This reduction was significantly associated with an increased risk of fracture in vegans of about 40% compared with omnivores.63,64 When looking at specific sites of fractures, there was more than double the risk of hip fractures. An earlier study identified that fracture risk was only significant in vegans who had sustained calcium intakes below 525 mg/day;65 however, in a longer term follow up of the same population, fracture risk was significantly increased even when adjusted for calcium and protein intake.64 It is likely that the reduction in BMD and increased fracture risk in vegans is multifactorial. Indeed, studies have shown calcium supplementation to be associated with only a minimal increase in body mass index without significant fracture prevention.66 Vegans tend to have significantly lower vitamin D levels in addition to lower BMI and lean mass than omnivores, which are independently associated with higher risk of osteoporotic fractures.67-70 Low vitamin B12 level has also been implicated as a potential contributor to osteoporosis via its effect on homocysteine. High homocysteine levels seen in vitamin B12 deficiency are associated with bone resorption, decreased bone formation and reduced bone blood flow.
Approach
It would be prudent to check vitamin D levels and replace to normal levels in addition to encouraging dietary calcium ingestion close to the RDI. The use of calcium supplementation for primary prevention in community-dwelling patients is controversial. There is some evidence that calcium supplementation may increase the risk of cardiovascular disease, and there is conflicting evidence regarding the efficacy of calcium supplementation in fracture prevention.71-77 More evidence is required. Additionally, ensuring adequate vitamin B12 and energy intake (and healthy body mass index) and recommending weight-bearing exercise is important to promote bone health.
Iodine
Iodine is an essential trace element that is solely used to form the two thyroid hormones thyroxine and triiodothyronine, which have many physiological roles including control of the basal metabolic rate, multiple cellular processes and normal growth. About 80% of the iodine in the body is stored in the thyroid gland.78 Iodine deficiency is the leading cause of preventable intellectual disability worldwide, and most industrialised countries have mandatory iodine fortification programs that have significantly reduced the frequency of overt iodine deficiency disorders.
Absorption
Iodine is readily absorbed via the stomach and proximal small bowel and stored in the thyroid gland.78 Although its absorption is not influenced by the composition of the diet, utilisation can be affected by goitrogens, which include cyanoglucosides found in sweet potato and maize and sulphur-containing thionamides found in vegetables such as cabbage, broccoli and brussel sprouts.79 Goitrogens in various ways impair the ability of iodine to be utilised, including blocking its uptake into the thyroid gland or impairing binding to thyroglobulin.80 However, the overall clinical significance of goitrogens is unclear.
Requirements
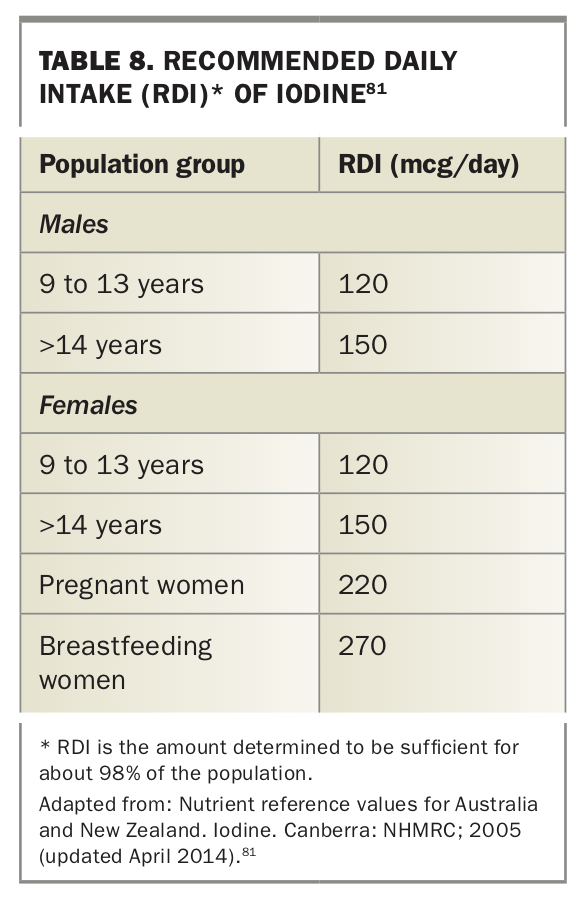
The recommended daily intakes are sufficient to prevent iodine deficiency disorders (Table 8).81 Iodine is naturally found in high quantities in seafood and seaweed (2200 mcg/100 g; one sheet of 3 g has about 66 mcg of iodine), but its quantity in other plant-based foods is largely influenced by the content in soil, irrigation and fertilisers. This is of particular importance in Australia (particularly south-east Australia) and New Zealand, where there is very low concentration of iodine in soil and subsequently minimal amounts of iodine in plant-based foods. Likewise, the concentration of iodine in tap water varies widely and is largely negligible. The maximum acceptable level is 500 mcg/L; most water only contains a fraction of this (e.g. <10 mcg/L in Adelaide, South Australia and 0.38 mcg/L in Gippsland, Victoria82,83).
{kind=link}
Deficiency
Iodine deficiency can result in a variety of conditions broadly termed ‘iodine deficiency disorders’, which vary in severity depending on the degree of iodine deficiency and the age of the person when exposed to deficiency. Severe iodine deficiency occurs with a long-term intake of less than 20 mcg/day. When occurring during pregnancy, severe iodine deficiency can be associated with various manifestations, the most significant of which are miscarriage and permanent intellectual disability in the child. Of note is that the fetus is most susceptible to iodine deficiency during the first trimester into the early second trimester.84 The effects of mild to moderate deficiency during pregnancy can still be pronounced and have been associated with a variety of neuropsychological defects and reduced intelligence into childhood.85-87 Iodine deficiency during childhood can cause further learning impairment, which is reversible. In addition, chronic iodine deficiency is associated with the formation of a goitre.
To increase the intake of iodine in the general population, mandatory iodine fortification, which included mandatory fortification of bread with iodised salt in addition to iodised table salt, was implemented in Australia in 2009. However, the use of iodised salt is not mandatory in commercial products or organic breads. These measures increased iodine intake at the population level, although mild to moderate iodine deficiency, particularly in pregnancy and lactation without adequate supplementation, remains relatively common.88-93 Food Standards Australia New Zealand estimated that 9% of women of child-bearing age were iodine deficient (down from 60% in 2009) and 1% of children aged 2 to 3 years (down from 9%), however did not take into account dietary practices or increased needs during pregnancy and lactation.94
A vegan diet confers a higher risk of iodine deficiency owing to the relatively poor selection of vegan sources of iodine apart from seaweed. Vegans have consistently been shown to have lower urinary iodine concentrations that fall into the mild to moderately deficient range.95-98 Iodine status of vegetarians varies based on location, with some studies showing similar levels to omnivores while others show deficiency.97,98
Approach
Unless regularly consuming a serve of seaweed, those on a vegan diet are likely to be at least mildly iodine deficient, with a high number being moderately deficient. Iodised table salt contains about 45 mcg of iodine per 1 g of salt, and the maximum daily recommended salt intake is 5 g (2000 mg of sodium; 225 mcg iodine). It is possible that the use of iodised salt in home cooking in conjunction with fortified breads may reduce the rates of moderate deficiency and are sufficient to avoid severe deficiency. Although the long-term effects of chronic mild deficiency in adulthood may be unnoticeable, it is important to recommend a pregnancy multivitamin to all women once they are planning pregnancy (or at the earliest possible time after conception), and this is even more important in women with vegetarian and vegan diets. It is recommended that women take a pregnancy multivitamin containing at least 150 mcg of iodine, although this still may not be sufficient, particularly in vegans who do not have commercial breads or use iodised table salt in cooking. It is very important to recommend supplementation is continued during lactation, when requirements are even higher.
Polyunsaturated fatty acids
There are two essential fatty acids that must be ingested. These are linoleic acid (LA) and alpha-linoleic acid (ALA). LA is the primary omega-6 (n-6) fatty acid and precursor to arachidonic acid, and ALA is the primary omega 3 (n-3) fatty acid and precursor to eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA).
These long-chain PUFAs are vital to cell membrane structure, cell signalling and gene expression and are key to the formation of the lipid compounds called eicosanoids (such as prostaglandins, prostacyclins).99 EPA and DHA are cardioprotective.100-103
The ability to convert ALA to EPA and DHA is limited and is suppressed by high intakes of LA.103 This has become a problem with the rise in LA content in diet due to increased use of vegetable oils, resulting in the dietary ratio of n-6:n-3 shifting from 4:1 to about 20:1.104,105 There is increasing evidence to suggest that maintaining a lower n-6:n-3 ratio of 5:1 or less may be beneficial.106,107
Requirements
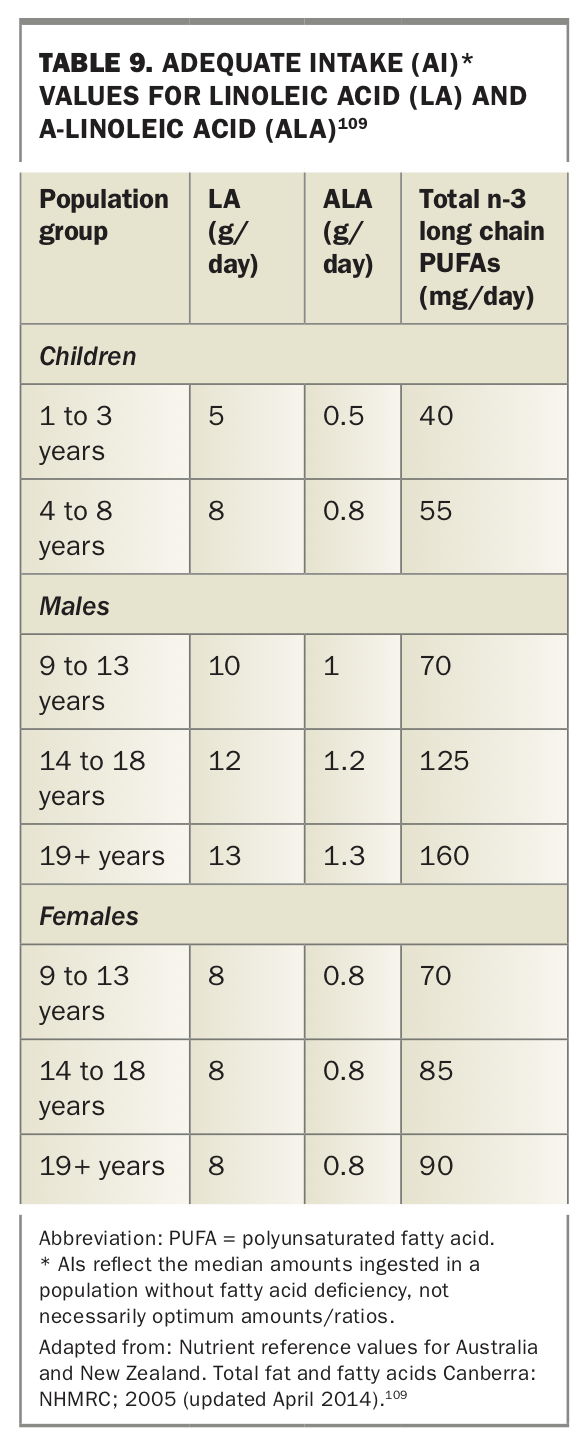
Both LA and ALA are readily available from plant sources, whereas EPA and DHA are most commonly found in fatty fish and thus intake is generally reduced in vegetarians and absent in vegans.108 In addition, although vegetarians and nonvegetarians have similar ALA intakes, the ratio of n-6:n-3 is higher for vegetarians, at about 14:1 compared with 9:1 for nonvegetarians. The current suggested adequate intakes are listed in Table 9 and foods high in ALA are listed in the Table 3.109 Of note is the high content of ALA in chia seeds and flaxseeds/linseeds.
{kind=link}
Approach
Fatty acid deficiency is rare in patients without conditions leading to fat malabsorption. Vegetarians can readily meet the suggested intakes of ALA and improve their LA:ALA ratio with even a small amount of chia seed or flaxseed in their diet, or by incorporating walnuts. In addition, reducing the amount of margarine and vegetable oils used in cooking or switching to extra virgin olive oil will reduce the amount of LA ingested. Supplementation is not commonly needed, but if avoiding high ALA foods, then EPA and DHA supplements are available through either fish oil or a vegan-friendly microalgae supplement.
Possible pitfall: disordered eating
Although most people who adopt a vegetarian or vegan diet do so in a healthy manner, it is important for GPs to assess the thinking of their patients surrounding food and motivations for a change in diet. A history of food restraint, weight loss or a dietary change that is sudden and inconsistent with familial eating patterns, particularly in younger patients, should serve as a red flag to explore further.
Eating disorders and body dysmorphia are relatively common, particularly in adolescents and young adults, with up to 7% having a form of eating disorder and 2% meeting criteria for body dysmorphic disorder, while many more have a strong preoccupation with body image.110-113 A history of discrimination, trauma and abuse has been well established in contributing to eating disorders and body image issues. More recently the rise of social media and ‘influencers’ places more focus on attaining an ‘ideal’ body type.
One condition that can often be missed is orthorexia. Although it is not yet formally recognised, it can be thought of as a type of avoidant/restrictive food intake disorder in its most severe form. Orthorexia is characterised by an obsession with healthy eating that leads to significant emotional distress through nonadherence to self-imposed nutritional limits and subsequent social impacts.114 Of note, it is not associated with a fear of gaining weight or abnormal body perception. Although often starting with the intent to truly eat healthily, patients with orthorexia begin to restrict whole food groups, selecting only foods they deem healthy, demonstrate a fixation on ingredient lists and nutritional labels, limit social interaction surrounding food and experience significant anxiety if their healthy foods are not available.115 Severe dietary restrictions can lead to energy and protein malnutrition and micronutrient deficiencies. Given its sometimes insidious onset, it would be useful to reassess an at-risk patient’s view on foods and body image yearly.
Conclusion
Vegetarian and vegan diets can provide adequate nutrition but may require additional planning, particularly for those transitioning to such diets for the first time. Practical tips directed at the patient level, including a nutritional analysis of select sample meal plans, are available.116,117 This is particularly important for vegans and for patients during pregnancy and while breastfeeding due to increased requirements. It is important to screen for the common nutrient deficiencies highlighted (in particular vitamin B12 deficiency in vegans, given its prevalence) but avoid falling into the trap of attributing all deficiency to diet alone without considering alternative causes or contributors. For those eating a more limited range of foods, a complete multivitamin can help meet daily requirements, but specific supplementation may be required. MT