Gastro-oesophageal reflux disease in infancy. A practical primer for the busy GP

Gastro-oesophageal reflux (GOR) is a challenging yet common clinical situation faced in primary care that requires a judicious practical approach. The assessment of infants presenting with regurgitation and vomiting should be directed towards distinguishing infants with physiological GOR from those with pathological gastro-oesophageal reflux disease (GORD). In most situations, an empathetic approach to manage expectations and provide reassurances where necessary is key.
Gastro-oesophageal reflux (GOR) is defined as the retrograde passage of stomach contents into the oesophagus. Its occurrence in infancy is a common reason for presentation to general practice.1 GOR may be associated with regurgitation (i.e. the expulsion of oesophageal contents proximal to the oesophagus) and/or vomiting. Gastro-oesophageal reflux disease (GORD) denotes presentations where GOR is complicated by organic pathology, which may include oesophageal inflammation, respiratory tract infections, aspiration episodes or troublesome symptomatology.2
Recognition of GORD in infancy is compounded by overlap in its clinical presentation with normal infant behaviour, including excessive crying, irritability, poor sleep and effortless regurgitation. Furthermore, the label of GORD based on troublesome symptomatology is particularly difficult in the assessment of nonverbal infants.
Available treatments for GORD, although effective, require judicious use to avoid potentially adverse side effects.3
Epidemiology and pathophysiology of GOR in infants
The incidence of GOR peaks at 3 months of age and tapers over the subsequent 12 months of life. At peak incidence, 60% of infants regurgitate once a day, with 25% having up to four episodes daily.4 Due to maturation of the lower oesophageal sphincter, physiological GOR, which seldom presents before 1 week or after 6 months of age, improves over time.5 Most infants will outgrow their symptoms by 12 months of age.5
Clinical presentation
Although many infants with GOR present with effortless regurgitation or vomiting, others may do so with various signs and symptoms. Excessive crying and infant ‘colic’ may be attributed to GOR, although this can be difficult to quantify objectively and an appreciation of normal variation is important.6
GORD is sometimes attributed as the cause of infants presenting with brief unresponsive episodes (BRUE); however, there is little prospective evidence linking the two.7 Therefore, apnoeas in infants should not be ascribed to GORD without further investigation. GORD may present with back-arching and posturing. Sandifer syndrome describes infants who present with neck extensor posturing and distress in the context of GOR.8 Infants presenting with feeding difficulty or those with recurrent otitis media should also have GORD considered as part of the differential diagnosis.
Clinical assessment
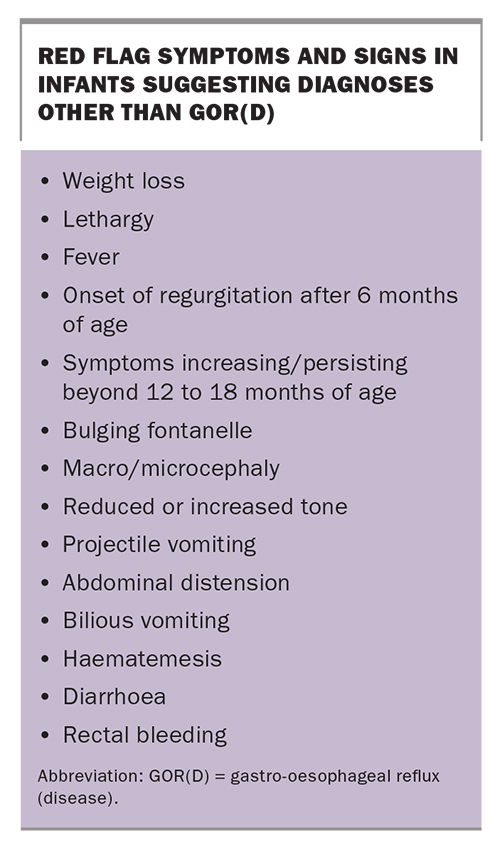
Clinical assessment of infants presenting with regurgitation and vomiting should be directed towards distinguishing infants with physiological GOR from those with pathological GORD or red flags (Box). A particular focus of clinical assessment should include feeding patterns that may suggest overfeeding or underfeeding.
{kind=link}
History should be obtained on the age of onset of symptoms, type of formula used for non-breast-fed infants and pattern of regurgitation in association with feeding. Further questioning should elicit risk factors for atopy and prior dietary or pharmacological interventions, as well as an understanding of complementary and alternative health beliefs in the family.
Physical examination must encompass the infant’s growth trajectory, nutrition and tone. Careful examination of the infant’s abdomen should be carried out for masses and distension. If there is clinical suspicion of serious pathology, specialist referral, often to a general paediatrician in the first instance, should be considered.
Investigations
The role of investigations in infant GORD is primarily to exclude alternative diagnoses and should be directed by clinical suspicion.
Infants with green bilious vomiting, projectile vomiting or abdominal distension should be referred urgently to a paediatric centre for investigation of possible mechanical obstruction.
Upper gastrointestinal contrast studies (barium, most often) may be obtained to rule out structural anomalies – e.g. malrotation. A videofluoroscopic swallow study should be considered in the setting of recurrent aspiration and chronic cough.9 GOR episodes seen on a barium study is of low clinical significance.
A midstream urine specimen to rule out urinary tract infection (UTI) should be considered in infants with irritability and frequent regurgitation of acute onset, even in the absence of fever. This specimen may be collected by clean catch or urinary bag, and a negative dipstick result for leucocyte esterase and nitrite is validated for ruling out UTI.10
Serological screening for coeliac disease with IgA tissue transglutaminase titres and total IgA level is reasonable for GORD in late infancy that occurs after gluten exposure.
Multichannel intraluminal impedance (MII) and pH studies are specialised tests that can detect acid and nonacid reflux episodes at different levels of the oesophagus; however, their value in diagnosing GORD is limited due to the lack of true normal reference ranges.11 These tests may be considered by a paediatric gastroenterologist in cases where recurrent aspiration pneumonia, otitis media, unexplained apnoeas or epileptiform paroxysmal behaviours, including back-arching, are otherwise unexplained.
Endoscopic investigations have a limited role in the diagnosis of GORD. Erosive oesophagitis is uncommon in infants.12 Equally, the presence of a normal appearing oesophagus endoscopically does not rule out GORD.13 Gastroscopy does, however, have a role in identifying conditions that mimic GORD, particularly eosinophilic oesophagitis (EoE). EoE is a chronic inflammatory disorder of the oesophagus characterised by eosinophilic infiltrate and consequent oesophageal dysmotility.14 Although rare, this can present in infants with symptoms akin to GORD. Due to the higher incidence of EoE in infants with atopy and IgE-mediated food allergies, a lower threshold for referral should be considered for this group.15
Management
Management of GOR and GORD requires an empathetic approach that often includes reassurance to parents and carers of normal infant behaviour. However, in cases where clinical judgement indicates a need for treatment, a stepwise approach, which may include nonpharmacological therapies, pharmacological therapies or both, is useful. This is summarised in the Flowchart.
Nonpharmacological therapies
Nonpharmacological therapies include positioning, feed thickeners and cow’s milk protein exclusion. Evidence for smaller, more frequent feeds, as opposed to overfeeding, is limited, although this intervention is cost-free and anecdotally effective in many infants.16 Any modification to a feeding regimen, however, needs to prioritise the adequate intake of volume and calories for age.
Upright positioning, although often believed to be helpful, has not been shown to reduce acid reflux in infants.17 Although reduced reflux events have been seen in clinical studies on premature infants with prone and left lateral positioning, supine positioning during sleep must be emphasised to mitigate the risk of sudden unexplained death in infancy.18
Starch or carob-gum based feed thickeners are useful, particularly for bottle-fed infants with visible and troublesome regurgitation. These have been shown to reduce the frequency of regurgitation and height of nonacid GOR on pH-MII studies.19 However, feed thickening does not reduce acid GOR or apnoea episodes in infants.20
The role of non-IgE-mediated cow’s milk protein intolerance (CMPI) in GOR is complex.21 However, several studies have shown improvement, on both pH investigation and clinical symptom measures, in some infants trialled on hydrolysed formula.22-24 In keeping with this, international guidelines recommend that a two- to four-week trial of dairy exclusion be considered for infants presenting with GOR.11 A recurrence of symptoms with reintroduction of cow’s milk protein confirms the diagnosis of CMPI. Resumption of an unrestricted diet should occur if dairy exclusion made no difference to GOR symptoms.
For bottle-fed infants being trialled on a cow’s milk protein exclusion diet, extensively hydrolysed formulas are first-line in infants under 6 months of age, whereas soy formulas can be considered in infants over 6 months of age. Reintroduction of cow’s milk protein at 12 to 18 months of age is usually successful.25
Pharmacological therapies
Alginates are designed to neutralise acid and often also act as feed thickeners. They should not be used in infants at risk of dehydration (e.g. those with acute vomiting or diarrhoea) or intestinal blockage due to reports of constipation. Although alginates have not reduced GOR symptoms based on symptom questionnaires, they do reduce visible regurgitation and vomiting.19,26 A one- to two-week trial of alginates is safe to consider but particular attention should be paid to appropriate dosing.27 For example, Gaviscon Infant powder, which contains sodium alginate and magnesium alginate, is available in sachets. For infants weighing less than 4.5kg, one sachet should be mixed into each feed, and two sachets for infants weighing 4.5kg and above. If this results in symptomatic improvement, alginates can continue to be used on a discretionary basis until the infant is weaned onto solids.
Studies assessing proton pump inhibitors (PPIs) have shown no improvement with regards to crying, cough, back-arching or regurgitation.28 H2-receptor antagonists fare no better in this regard.29 In addition, there is emerging evidence that early exposure to acid suppression therapy may even be harmful and increase the risk of childhood fractures.3 Acid suppression can be considered as a therapeutic trial in children aged over 12 months who persist with troublesome symptoms for presumptive reflux oesophagitis. However, early referral to secondary care should be considered for these children.
Promotility agents such as domperidone and erythromycin can improve gastric emptying. However, infants with GORD have not been shown to have delayed gastric emptying times.30 There is some anecdotal evidence for the role of these agents in infants with impaired antroduodenal motility. However, the use of these drugs in the paediatric age group is off-label and, coupled with their side effect profile, necessitates specialist guidance.16
GORD and maternal mental health
GORD negatively impacts infant–maternal bonding and may lead to dysfunctional feeding and sleep routines.31 A pre-existing history of maternal mental health issues, particularly maternal anxiety, also predisposes to more frequent visits to primary care and hospitalisation of infants with GOR.32 It is appropriate to consider maternal mental health issues and provide adequate support when required.
Conclusion
Feeding routines form the basis of healthy infant–parent interactions. GOR(D) may have a significant negative impact on this. A systematic approach that allows for identification of infants at risk of other diagnoses who require further investigation and a stepwise approach to management is advisable. MT
COMPETING INTERESTS: None.