A woman with a scaly inguinal plaque

Test your diagnostic skills in our regular dermatology quiz. What has caused this skin discolouration?
Case presentation
A 55-year-old woman presents with asymptomatic discolouration in her groin that has been present for several months (Figure 1a). She has a history of type 2 diabetes and obesity.
{kind=link}
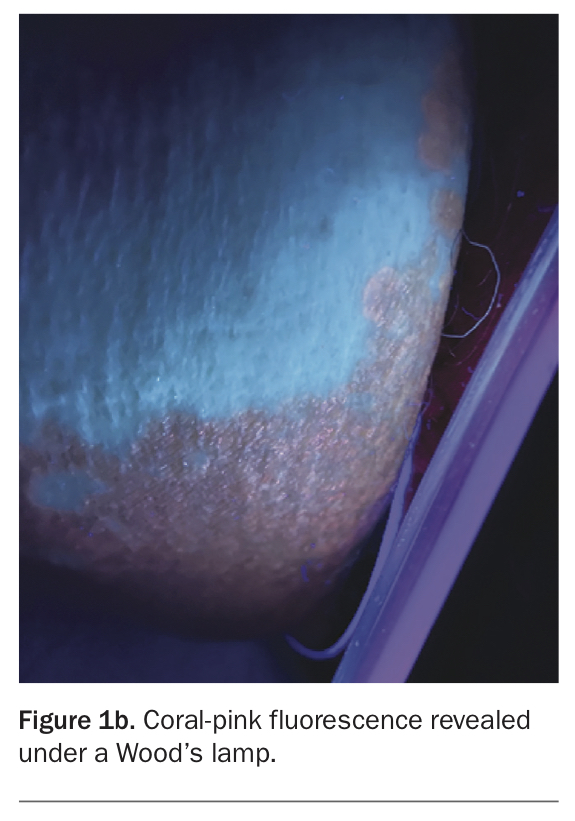
On examination, well-demarcated brown plaques with fine scale are observed in the left and right inguinal folds and extending onto the thighs. Examination under a Wood’s lamp reveals coral-pink fluorescence (Figure 1b).
{kind=link}
Differential diagnoses
Diagnoses to consider in a patient presenting with a well-demarcated scaly plaque in the inguinal fold include the following.
Tinea cruris
Tinea cruris (‘jock itch’) is a dermatophyte infection of the inguinal region (groin, pubic region and adjacent thigh) and occasionally extends to the abdomen and buttocks.1 It typically presents as an erythematous, pruritic and sharply demarcated plaque that has a raised leading edge with scale and central clearing.1
Tinea cruris has a male predominance (males:females 3:1) and is most commonly caused by Trichophyton rubrum. The condition is frequently associated with tinea pedis, which can occur if clothing that is worn against the groin region becomes contaminated by first coming into contact with feet when dressing.1
For the case patient described above, a diagnosis of tinea cruris is less likely because her plaque shows a diffuse distribution of fine scale (seen in Figure 1a) rather than the leading edge of scale with central clearing that is typical of dermatophyte infections. Furthermore, the plaque is brown, which is unlike the typical erythematous appearance of tinea. In addition, tinea cruris does not fluoresce under a Wood’s lamp.
Granular parakeratosis
A benign condition, granular parakeratosis presents at intertriginous sites as pruritic, erythematous or brown, scaly papules or plaques with desquamation and peeling. It has been linked to the use of personal hygiene products and, more recently, to laundry rinse aids containing benzalkonium chloride.2-4 Although it is rare, with an incidence of about 0.004 to 0.005%, clinicians should have a high index of suspicion for granular parakeratosis in patients who present with erythematous flexural eruptions and seek a history of exposure to benzalkonium chloride – especially given the increased use of antiseptic agents secondary to the COVID-19 pandemic.4-6
For the case patient, a diagnosis of granular parakeratosis is less likely because, although this condition can present with brown plaques, there is an absence of erythema and desquamation/peeling. In addition, coral-pink florescence is not observed for granular parakeratosis under a Wood’s lamp.
Pityriasis versicolor
Pityriasis versicolor is a common superficial yeast infection caused by Malassezia furfur that produces only a minimal, if any, inflammatory response.1 It is also known as tinea versicolor but, unlike tinea cruris (or tinea pedis or tinea capitis), it is not caused by a dermatophyte. In tropical locations, this largely asymptomatic condition has a prevalence of up to 50%.7
Pityriasis versicolor typically presents as multiple oval-to-round macules or patches or thin plaques with a fine scale.1 These lesions, which may be hypopigmented, hyperpigmented or erythematous, are often found in seborrhoeic regions such as the upper trunk and shoulders. Less commonly, flexural areas such as the groin can be affected (‘inverse’ pityriasis versicolor).1
Pityriasis versicolor is typically diagnosed clinically. If required, KOH examination of associated scale will reveal both hyphal and yeast forms resembling ‘spaghetti and meatballs’.1 In about 30% of cases, examination under a Wood’s lamp reveals bright yellow florescence.8
For the case patient, pityriasis versicolor is a less likely diagnosis because it usually has less scale and does not fluoresce coral-pink under a Wood’s lamp.
Erythrasma
This is the correct diagnosis. Erythrasma is a superficial and often chronic skin infection caused by Corynebacterium minutissimum most commonly affecting the webbed spaces of the toes and intertriginous areas such as the groin, intergluteal fold, umbilicus, axillae and inframammary region.9 The condition initially presents as well-defined pink to brown patches or plaques with a fine scale and is typically only mildly pruritic or asymptomatic.9
Predisposing factors for erythrasma include poor hygiene, diabetes mellitus, obesity, hyperhidrosis and immunosuppression.9 The incidence of erythrasma worldwide is about 4%, but it is more common in tropical and subtropical areas because of the warm and humid climate.10
The hallmark of erythrasma is coral-pink fluorescence on Wood’s lamp examination, as seen in Figure 1b. This unique colouration is caused by illumination of porphyrin produced by the bacteria.1 Although not usually necessary, C. minutissimum can be cultured and staining reveals Gram-positive filaments and rods in the scale.9
This patient has the typical clinical presentation of erythrasma (well-demarcated brown plaques with fine scale that fluoresce coral-pink under a Wood’s lamp) as well as two known risk factors (obesity and type 2 diabetes).
Management
The treatment of erythrasma depends on the extent of disease. Localised disease can be treated tolerably with topical antibacterial agents. A 2013 double-blind, randomised, placebo-controlled trial showed sodium fusidate 2% ointment (typically twice daily for 14 days) to be significantly more effective for erythrasma than oral erythromycin or clarithromycin.11 Another effective topical treatment option is clindamycin hydrochloride, available at a strength of 1%, applied two or three times daily for seven days.12,13 For widespread or recalcitrant disease, oral antibiotics may be necessary, and there is good data to support use of a single dose of 1 g clarithromycin.11 Antibacterial soaps may help to prevent recurrences.
Type 2 diabetes is a common predisposing factor for erythrasma. In fact, erythrasma outside of the usual intertriginous locations (a ‘disciform’ variant) may be the presenting manifestation of type 2 diabetes.9 A patient who is diagnosed with erythrasma should be examined for systemic sequelae of type 2 diabetes such as acanthosis nigricans and, if relevant, a workup for should be diabetes considered.
Although benign and asymptomatic in the majority of cases, erythrasma has been reported to progress to cellulitis or bacteraemia in immunocompromised patients.9 Therefore, failure to respond to appropriate therapy warrants referral to a dermatologist.
Outcome
The case patient was diagnosed with erythrasma, which was treated with topical clindamycin hydrochloride 1% twice daily for seven days, with resolution. MT