Mild cognitive impairment and mild dementia: recognition, diagnosis and management

Mild cognitive impairment and mild dementia are common presentations in general practice. Early recognition of symptoms, screening and assessment for a diagnosis, and implementation of lifestyle approaches to target dementia risk reduction can help reduce the rate of cognitive decline. Specialist referral should be sought for further evaluation to confirm the diagnosis. For people with mild to moderate Alzheimer’s disease, treatment with acetylcholinesterase inhibitors is warranted, and novel disease-modifying therapies using monoclonal antibodies may soon be available.
Dementia is the second highest cause of death in Australia, and the lead cause of death in women.1,2 It is a feared diagnosis with high direct and indirect health and personal costs for patients, their family and society. Consequently, there is an increasing focus on risk reduction and more comprehensive management of people in the early stages of dementia. Recently, a clinical quality registry for dementia has been established, with increasing efforts being made to bring high quality assessment, support and opportunities to be involved in research to all Australians with dementia and its prodromal stage, mild cognitive impairment.
In 2021, the first disease-modifying therapy for mild Alzheimer’s disease was approved in the US but is not yet approved in Australia and, recently, promising results have been shown with another therapy in the same class.3,4 Blood-based biomarkers to facilitate the detection and diagnosis of Alzheimer’s disease may also soon be available. It is therefore timely to review the common cognitive disorders, how to best detect them and the current and future management approaches.
What are mild cognitive impairment, early Alzheimer's disease and 'mild dementia'?
The term ‘mild cognitive impairment’ (MCI) has had numerous connotations over the years and, along with ‘mild dementia’, is increasingly used to describe the early clinical stages of a neurodegenerative cognitive disorder, rather than the underlying pathology itself. MCI is not used universally in this context, and indeed is still rarely used in Europe (where ‘prodromal’ is the preferred term); however, it is commonly used in Australia. Thus, Alzheimer’s disease can be preclinical (asymptomatic) or it can cause MCI, where cognition – usually memory – is impaired but function is preserved. This impairment can progress to the stages of dementia – mild, moderate or severe – with increasing impairment of day-to-day function. Early, or mild, Alzheimer’s disease includes MCI and mild dementia due to Alzheimer’s, and targeting these early stages of the process is the focus of most of the recent research into new therapies. Other neurocognitive diseases, including Lewy body disease (LBD) and frontotemporal dementia (FTD), also likely have preclinical, MCI and dementia stages.
The diseases themselves are associated with an accumulation of toxic (and usually misfolded or aggregated) proteins in the brain, including amyloid-beta and tau (Alzheimer’s disease), tau, and/or TDP43 (FTD) and alpha-synuclein (LBD), although the role of these proteins in causing the clinical manifestations of these diseases is subject to intense scrutiny. This accumulation usually progresses over decades, and treatment with disease-modifying therapies and risk reduction strategies in the early stages of cognitive decline can improve outcomes. It is difficult to restore or even slow down deterioration in a brain that has suffered extensive damage from these toxic proteins and no current therapies have been shown to achieve this.
Normal ageing versus MCI and mild dementia
All too often, older people feel or are told it is ‘normal’ to become forgetful as we age. Although minor changes in attention and memory do occur with age, the changes associated with MCI and mild dementia are far more profound and impacting. GPs are well positioned to reassure the patient who is aware that memory disorders can occur with ageing and is concerned about their occasional lapses, and to further assess the patient who is constantly misplacing objects, repeating themselves and leaving heaters, stove or taps on.
How common are MCI and mild dementia?
About 500,000 people in Australia have dementia, of which 60% have Alzheimer’s disease. What is less clear is the prevalence of MCI; however, the number is likely close to one million. In the Sydney Memory and Ageing Study, the incidence of MCI in those aged 70 to 90 years was just over 100 per 1000, or about 10% per year, and prevalence studies have shown 5 to 37% of people over the age of 60 years have MCI.5,6 People with MCI progress to dementia about three times faster than those without MCI.7 Not all people who develop MCI progress to dementia; some revert to normal cognition, and a few who have dementia have bypassed the MCI stage, therefore, it is likely that the prevalence of MCI is much higher than that of dementia.7,8
How to detect MCI and mild dementia
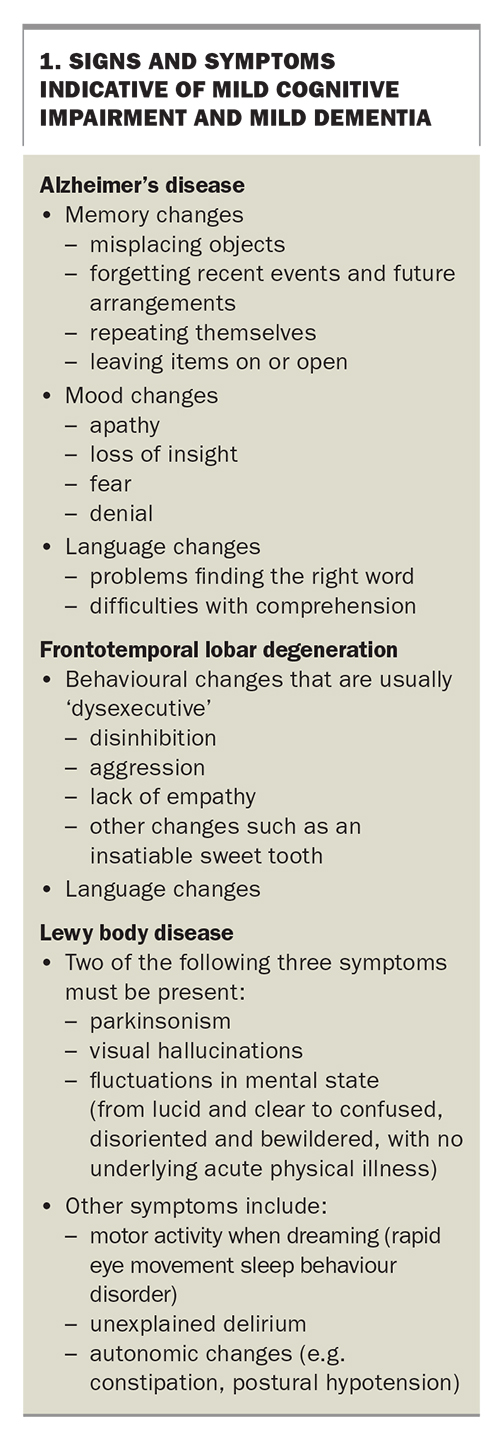
It is important to differentiate mild changes of ‘normal ageing’ from these first signs of a neurodegenerative disease. Typical signs and symptoms of MCI and mild dementia are summarised in Box 1.
{kind=link}
Alzheimer’s disease is the most common neurological disorder; patients usually present with concerns about memory, such as misplacing objects, forgetting recent events and future arrangements, repeating themselves and leaving items on or open. They may experience changes in their ability to plan and organise, as well as subtle changes in mood, for example, they may become increasingly apathetic. Patients may have lack of insight into, or may be in fear or denial of, changes in their behaviour, and may be brought to their GP by a concerned relative.
Patients with FTD can present with behavioural and ‘dysexecutive’ changes, including disinhibition, aggression and a lack of empathy, and other changes, such as an insatiable sweet tooth. Language changes, including comprehension difficulties or problems finding the right word, are an early feature of FTD and can also occur with Alzheimer’s disease.
Patients with LBD usually present with a combination of parkinsonism, motor activity when dreaming (rapid eye movement sleep behaviour disorder), visual hallucinations, fluctuations in mental state, unexplained delirium and autonomic changes (e.g. constipation, postural hypotension). LBD can be difficult to distinguish from Parkinson’s disease and people with Parkinson’s disease often develop dementia that is similar to LBD.
Recognising signs of a neurodegenerative decline in younger patients is equally important but often challenging, as healthcare professionals are less attuned to the likelihood of a young onset neurodegenerative disease. Patients younger than 60 years are often misdiagnosed as depressed or suffering from a completely different disease, and may take longer to be accurately diagnosed.
What tests are available to assist diagnosis?
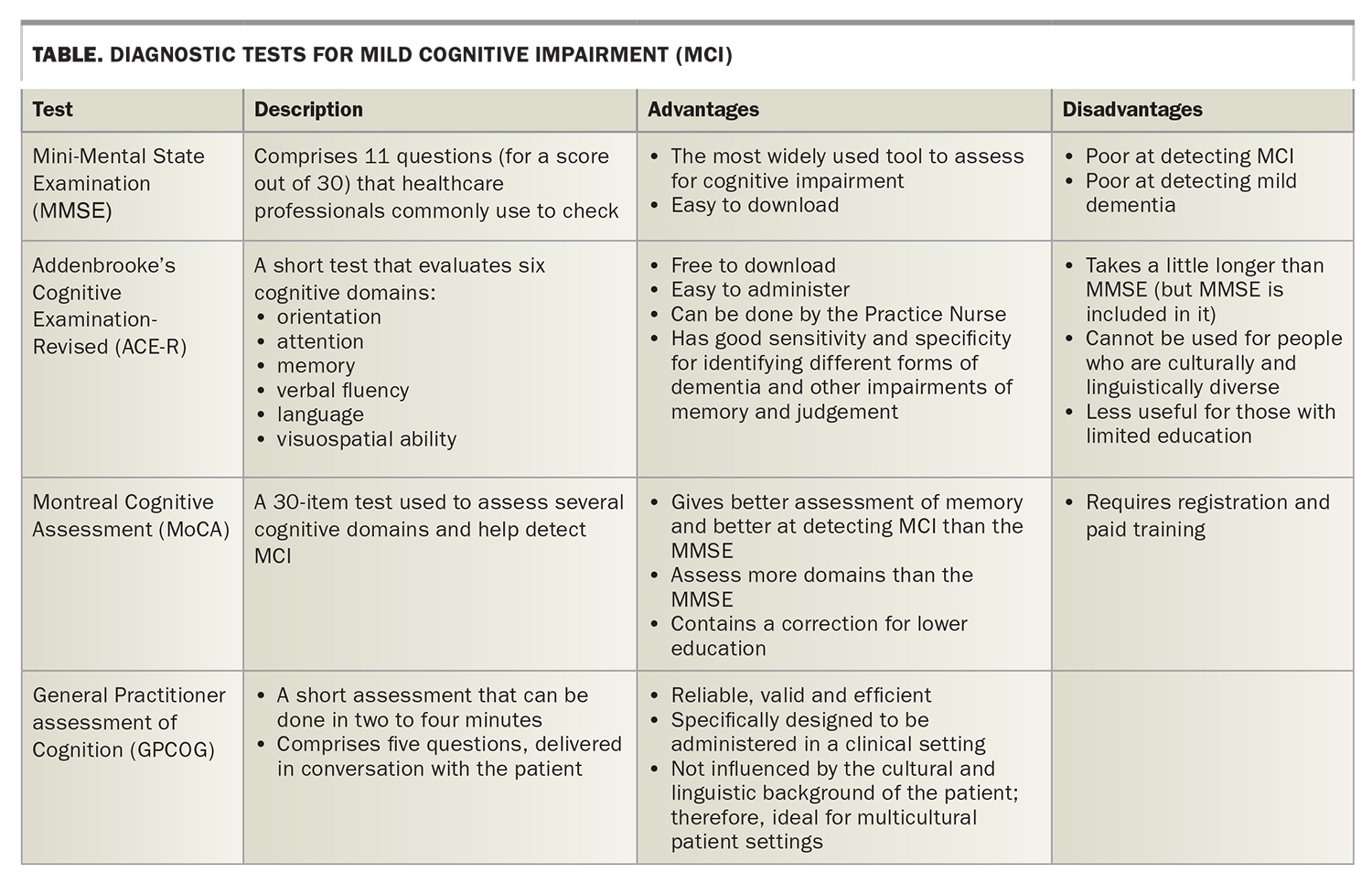
A cognitive test should be used for any patient with a suspected neurodegenerative disease (Table). The Mini Mental State Examination (MMSE) is the most widely used tool and, although it tests several cognitive domains, it is poor at detecting MCI or mild dementia. More sensitive tests include the Montreal Cognitive Assessment (MoCA), which requires registration and paid training, and the Addenbrooke’s Cognitive Examination-Revised (ACE-R).9 The ACE-R is easy to administer and can be done by the Practice Nurse, and has good sensitivity and specificity for identifying different forms of dementia and other impairments of memory and judgement. It is also available online at no cost (www.sydney.edu.au/brain-mind/resources-for-clinicians/dementia-test.html). The General Practitioner assessment of Cognition (GPCOG) is a quick screening tool for cognitive impairment designed to screen for dementia in a primary care setting. Like the ACE-R, it is easy to administer and available online at no cost (http://gpcog.com.au).
{kind=link}
A CT brain is often ordered in a clinical setting; however, an MRI is more useful and CT is typically only used for patients who cannot have an MRI brain. Patients referred to a specialist are likely to undergo additional testing, including detailed neuropsychological evaluation, a positron emission tomography (PET) scan (either fluorodeoxyglucose or amyloid) and an MRI. Patients with more complex symptoms may require cerebrospinal fluid analysis and other evaluations.
What tests may be freely available soon?
A test for blood-based biomarkers may soon be available to detect specific markers of neurodegeneration and diagnose Alzheimer’s disease. The biomarkers that show the greatest correlation with cerebrospinal fluid analysis and PET scans, and therefore the most promise for detecting neurogenerative diseased, are the amyloid and phosphorylated tau proteins.10 Although it seems likely that these tests will assist detection and diagnosis, they have not yet been studied as a screening tool that could be used in general practice.
When should I refer to a specialist?
Specialist referral should be made for a patient with objective impairment of cognition (e.g. on the ACE-R tool) or when the patient or their family are sure of a decline in cognitive function. GPs are then well placed to clarify or further discuss a diagnosis and establish individualised management and support, and are encouraged to work within a team care arrangement that includes either memory clinics, research screening sites (such as the Australian Dementia Network) or geriatricians, psychogeriatricians and neurologists for optimal patient management. As GPs in Australia become more extensively trained in the diagnosis and management of cognitive disorders, the need for specialist confirmation of a diagnosis of MCI may change.11
What is the natural course of MCI and mild dementia?
Most people with MCI progress to dementia and are eventually diagnosable as suffering dementia, usually due to Alzheimer’s disease. However, not all people with MCI progress to dementia; some improve and no longer have a cognitive disorder. This highlights the ‘instability’ of a clinical diagnosis of MCI without a confirmatory test, such as an amyloid PET. Some people die with an MCI diagnosis and, in many cases, this is simply because they have had ‘insufficient time’ to progress to dementia. Once dementia has been diagnosed, whatever the cause, it is very rare to see clinical improvement; however, decline may be attenuated by the approaches outlined below.
What therapies are currently available?
Four medications are approved for the treatment of Alzheimer's disease in Australia: three acetylcholinesterase inhibitors (donepezil, rivastigmine and galantamine) and memantine. They have limited proven benefit in dementia and no proven benefit in MCI. They have modest benefits on cognition, and may have other noncognitive benefits, including improved behaviour, mood, function and, with memantine, functional communication. Indirect benefits include reduced caregiver burden and delay to needing residential care.
The three acetylcholinesterase inhibitors are functionally similar and are used to treat mild to moderate Alzheimer’s disease. Rivastigmine confers additional butyrylcholinesterase inhibition, which results in an improved response in some patients, and is often delivered as a patch for convenience.12 Memantine is given to patients in later stages of Alzheimer’s disease (usually to those with an MMSE score below 20). All four medications are available on the PBS for those with a diagnosis confirmed by a specialist (which can be by telephone discussion with the GP) but only one can be subsidised – either an acetylcholinesterase inhibitor or memantine. None are approved for initiation on the PBS for an MMSE score below 10, unless there is a noncognitive reason for this, such as if the patient is from a culturally and linguistically diverse community or has aphasia. GPs can initiate and provide repeat perscriptions for these medications once the initial diagnosis has been confirmed by a specialist.
These agents have considerable side-effect profiles. The three acetylcholinesterase inhibitors can adversely affect the gastrointestinal tract and bladder and cause bradycardia, whereas memantine can cause anxiety and agitation. This risk is reduced by up-titrating to the recommended (most effective) dose gradually and, in the case of donepezil, taking it on a full stomach.
If the medication is causing severe adverse effects or if, after three months, it is clearly not impacting on the patient’s decline, it should be ceased, and a different cholinesterase may be trialled. One study showed 56% of those who did not respond to, or could not tolerate, donepezil responded to rivastigmine.13
In those with LBD, a trial of a cholinesterase inhibitor is warranted; however, it is not PBS approved for this condition. Fortunately, most people with LBD also have Alzheimer’s pathology and may be subsidised accordingly. A ‘lazaroid’ (potent antioxidant) response can occur with these agents in LBD as the acetylcholine deficiency is sometimes greater than in Alzheimer’s disease.
In a small randomised controlled trial in people with MCI due to Alzheimer’s disease, the nutritional supplement Souvenaid showed modest benefits on cognition, function and brain atrophy compared with placebo.14 It is reasonable to consider Souvenaid for patients with MCI, although more evidence is needed for a consensus recommendation.
Are there other management approaches?
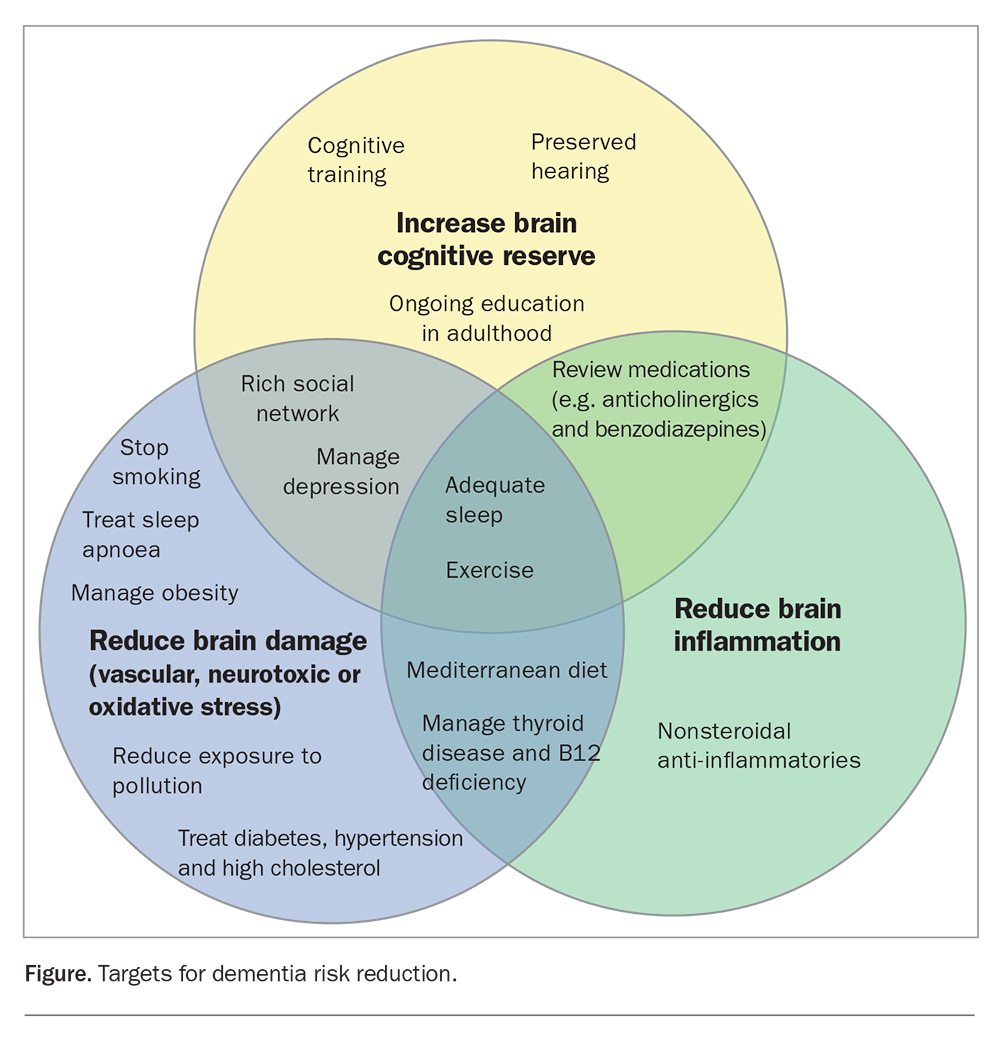
Lifestyle approaches to target dementia risk reduction are warranted for all people with MCI and may reduce the rate of decline in those with dementia. The value of the GP–patient relationship, including an individualised management plan, ongoing support in the context of multidisciplinary care and enhanced primary care options, is pivotal to achieving effective uptake of strategies that may reduce the risk of cognitive decline and support mental and physical health more broadly (Figure). Strategies include reaching or exceeding minimal recommendations for physical exercise, eating a Mediterranean diet, performing mental activities (including cognitive training) and ensuring social interaction.
{kind=link}
Other risk factors for dementia that should be managed to help improve cognition and delay cognitive decline include:15
- diabetes
- depression
- sleep apnoea, an important emerging risk factor for dementia
- medications that may contribute to cognitive decline (e.g. anticholinergics and benzodiazepines)
- thyroid disease
- B12 deficiency
- obesity or overweight, particularly in later life
- smoking
- heavy alcohol consumption
- hearing loss, especially at midlife
- air pollution, although this is often a function of where a person lives and difficult to avoid.
An aged care assessment and support services are usually required as the disease progresses and the need for these should be reviewed at follow up appointments. Caregiver burden should be monitored and addressed. Patients should be offered access to resources and support services, such as those offered by Dementia Australia (www.dementia.org.au) and Forward with Dementia (https://forwardwithdementia.au). Resources for patients living with dementia and their carers are listed in Box 2.
{kind=link}
What therapies are on the horizon?
The first disease modifying therapy for mild Alzheimer’s disease, the monoclonal antibody aducanumab, was granted accelerated approval by the US Food and Drug Administration in late 2021. It has been shown in two Phase 3 studies to remove brain amyloid and, when administered at the recommended highest dose, to reduce the rate of cognitive and overall decline by about 22% compared with placebo.3 However, aducanumab has several potentially severe side effects, including cerebral oedema and haemorrhage, and is not yet approved for use in Australia. Aducanumab is administered intravenously every four weeks and patients are monitored closely for adverse effects, including having regular MRIs to assess for cerebral oedema.
At least three other monoclonal antibodies against amyloid-beta and amyloid plaques (donanemab, lecanemab and solanezumab) have been studied for the treatment of mild Alzheimer’s disease. Donanemab showed promising results in a Phase 2 clinical trial of patients with early Alzheimer’s disease and is now in Phase 3 trials.16 Lecanemab slowed cognitive decline in people with early Alzheimer’s disease by 27% and is currently under review by the US Food and Drug Administration.4 Phase 3 trials with solanezumab showed no improvement in cognition or functional ability in people with mild-to-moderate Alzheimer’s disease.17 Other potentially disease modifying therapies targeting many components of the pathology associated with Alzheimer’s disease are also undergoing advanced stage clinical trials.
A new therapeutic era for Alzheimer’s disease treatment could move away from symptom management and towards effective disease modification. In the future, those at higher risk of cognitive decline (family history, age above 70 years, memory symptoms) may undergo an amyloid PET scan or a blood-based biomarker test to assess for amyloid accumulation and, if found, could be treated with a combination of disease modifying drug therapies and risk reduction strategies to delay, or even avoid, the onset of symptoms or decline. However, more data is needed before we embrace this approach.
Conclusion
MCI and mild dementia are common conditions. Health professionals need to be aware of the signs and symptoms of cognitive decline and be able to differentiate them from normal ageing to reach a timely diagnosis. Effective testing tools are available to help diagnose cognitive decline and should be used for assessment. Early referral to a specialist is recommended to provide further assessment, access to biomarker tests such as PET scans, and assistance in managing this chronic disease over time. Lifestyle changes and, when the dementia stage is reached, cholinesterase inhibitors and memantine, are pivotal to management. Caregiver support and providing access to resources and education is also encouraged. MT
COMPETING INTERESTS: Associate Professor Woodward has been on the Advisory Boards of, and received consultation and speaker fees from, Nutricia, Biogen, Roche and Eisai.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.