Other vaccine recommendations for older people


Immunisation
Seniors' health
In addition to influenza, pneumococcal and herpes zoster vaccines, older people are recommended to have tetanus and pertussis booster vaccines and vaccines for special risk scenarios. A range of vaccines against other diseases with a high burden in older people are in the pipeline.
- Most tetanus cases and deaths are in older people.
- A tetanus booster vaccine is recommended for all adults at ages 50 years and 65 years if their last dose was more than 10 years previously; unvaccinated adults should receive a primary course plus boosters.
- Most older people are susceptible to pertussis, which can have severe consequences in this age group, as well as potentially infecting infants they contact.
- An opportune time for pertussis vaccination is at the time of tetanus vaccination, using the combined vaccine.
- Older travellers and healthcare workers should follow the same vaccine recommendations as younger people.
Several vaccines are recommended for older people in addition to the influenza, pneumococcal and herpes zoster vaccines already discussed in this Supplement.1-3 For example, boosters of tetanus and pertussis vaccines are important in this age group. Further, older people in specific scenarios are at increased risk of vaccine-preventable diseases, and extra vaccines should be considered. These include older people with reduced immune function and travellers. Recommendations for these extra vaccines and specific risk groups are outlined here. Vaccines for older people in the development pipeline are also described.
Tetanus
In Australia, 80% of tetanus notifications and 90% of tetanus deaths since 1980 have been in adults aged over 50 years.4,5 In the US, 60% of tetanus cases occur in people aged over 60 years.6 Despite tetanus being mainly seen in the older population, the number of deaths from this disease is very low.
Almost all adult cases of tetanus occur in people who never completed a primary childhood immunisation series. A history of immunisation from patients, families or medical charts may be an unreliable indicator of tetanus immunity. Thus, the main thrust of any adult tetanus vaccination policy should be to ensure that everyone receives a primary immunisation series and booster vaccinations.
Seroprevalence studies in the US have shown that more than half of adults lack antibody levels that are considered protective against tetanus and support the need to give primary courses and boosters, especially to those with tetanus-prone wounds.7 Older people have a good response to a single dose of tetanus vaccine.8
The 2018 edition of the Australian Immunisation Handbook recommends a booster dose of tetanus-containing vaccine for all adults at 50 years and 65 years of age if their last dose was more than 10 years ago.9 Unvaccinated adults should receive a primary course of three doses, followed by boosters 10 and 20 years later. Tetanus vaccine is available in combination with diphtheria vaccine (dT) or with diphtheria and pertussis vaccines (dTpa).9 The latter differs from the childhood formulation (DTPa) as it contains smaller amounts of diphtheria and pertussis antigens.
Pertussis
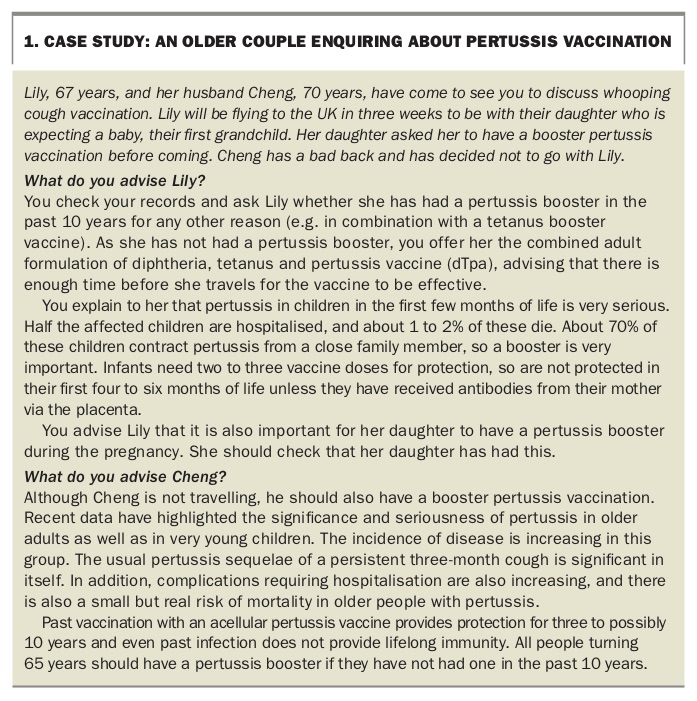
The protection provided by acellular pertussis vaccination wanes rapidly, and full protection lasts on average up to five years. Similarly, pertussis infection does not provide lifelong immunity. Most older people are susceptible to pertussis, and data increasingly show that infection can have severe consequences in this age group.10 Recent evidence shows that pertussis-associated deaths occur in older people as well as the very young.10 Because of the increase in morbidity associated with pertussis in older people, they are recommended to have a single booster dose of dTpa, which is the only adult pertussis vaccine available, if they have not received this vaccine in the past 10 years.11-13
Vaccination is also supported for older people who intend to have close contact with infants (younger than 6 months), to prevent pertussis transmission in the period before the infants are fully protected by direct immunisation (see the case study in Box 1 and Special risk scenarios, below). However, increasing vaccination of pregnant women may soon reduce this need.
{kind=link}
An opportune time for pertussis vaccination is at the time of tetanus vaccination, using dTpa. Reviewing the pertussis vaccination status of all people when they turn 65 years of age will protect them and reduce circulation in the community.
Meningococcus
Meningococcus (Neisseria meningitidis) strain W has emerged as the predominant meningococcus strain in Australia, surpassing strain B in 2016.14,15 Strain W is a hypervirulent strain associated with a higher risk of invasive disease and mortality. In 2017, adults aged over 65 years accounted for 25% (24/94) of the total cases reported in Australia. Two meningococcal vaccines, a quadrivalent meningococcal conjugate vaccine covering strains A, C, W and Y and a meningococcal B vaccine, are available for adults through private prescription.
Meningococcal vaccination is recommended for adults with immunodeficiency, including those who have had a splenectomy and those with HIV infection, if they are a close contact of a person with meningococcal infection, and those taking the medication eculizumab.16 It is not known whether patients taking other types of monoclonal antibodies are at increased risk of meningococcal disease. In 2017, the state of Victoria funded meningococcal vaccine for all gay and bisexual men and men who have sex with men, at any age.17 In areas with regional outbreaks in any age group, vaccination against the prevalent strains should be offered to older people irrespective of additional risk factors.
Haemophilus influenzae
Vaccination against Haemophilus influenzae type b (Hib) is recommended for infants, children and some people who are immunocompromised. This includes patients who have undergone splenectomy and were not vaccinated in infancy or were incompletely vaccinated, functional and autologous haematopoietic stem cell transplant recipients and all solid organ transplant recipients.18
Special risk scenarios
People with reduced immune function
Although older age itself is associated with a reduction in most immune functions, in some people other conditions further reduce immune competency. In people who are immunocompromised, vaccination with a live vaccine (e.g. the live attenuated herpes zoster vaccine) is less safe, and response to vaccination with most other vaccines is reduced.
The live attenuated herpes zoster vaccine can be safely given to about 97% of older people. This includes those using corticosteroids in the following categories: those taking oral prednisolone at a dose less than 20 mg for less than two weeks; those using inhaled or topical corticosteroids; and those taking corticosteroids as replacement therapy. More detailed recommendations on whether a person is immunocompromised to the extent that they should not receive this vaccine have been recently published.19
Recommendations on vaccination for people about to become immunocompromised (e.g. by elective splenectomy or by taking higher-dose immunosuppressants) can be broadly summarised as: check current vaccination status and give any outstanding vaccines. More detailed advice for people about to undergo splenectomy are available from Spleen Australia (https://spleen.org.au).20
Grandparents and other older people exposed to children
Infants younger than 6 months, who are too young to have received a full course of pertussis vaccine, are at risk of being infected with pertussis, typically by an older relative such as a grandparent or great-grandparent. Pertussis vaccination should be offered to older people before contact with infants younger than 6 months. Increasing immunisation of pregnant women to protect their infants through passive immunity via the placenta may affect this recommendation.
No other additional vaccinations are recommended for older people in contact with younger people. Indeed, it is likely that protection works the other way – vaccination of younger people with conjugated pneumococcal vaccine and influenza vaccine protects older people through herd immunity.
Older travellers
Older people should be offered the same travel vaccinations as those recommended for younger people for the countries they are to visit. This is particularly important as travel becomes easier and safer, and thus more often undertaken by older people. Individualised advice according to older people’s medical conditions and degree of immunosuppression is recommended; more details are available in the Australian Immunisation Handbook.21
Older healthcare workers
Increasingly, older people continue to work into their 60s and 70s, including in health care. Older healthcare workers should follow the same vaccination recommendations as their younger counterparts. This includes annual influenza vaccination. Influenza vaccine coverage of GPs is more than 70%, whereas coverage in hospital staff is less than 50%.22,23
Regional issues
Healthcare practitioners should remain aware of regional outbreaks, and adjust vaccination recommendations accordingly. Similarly, in some tropical regions the usual seasonal variations in influenza are less apparent, and vaccination at other times may need to be considered, subject to vaccine availability.
Vaccines in the development pipeline
Over the next few years, new vaccines for older people are likely to become available. These include more effective vaccines than those currently available (e.g. both a 15-serotype and a 20-serotype conjugate pneumococcal vaccine) and vaccines for infections not currently covered by vaccines (e.g. Clostridium difficile, Pseudomonas aeruginosa and Staphylococcus aureus infections and possibly even malaria).
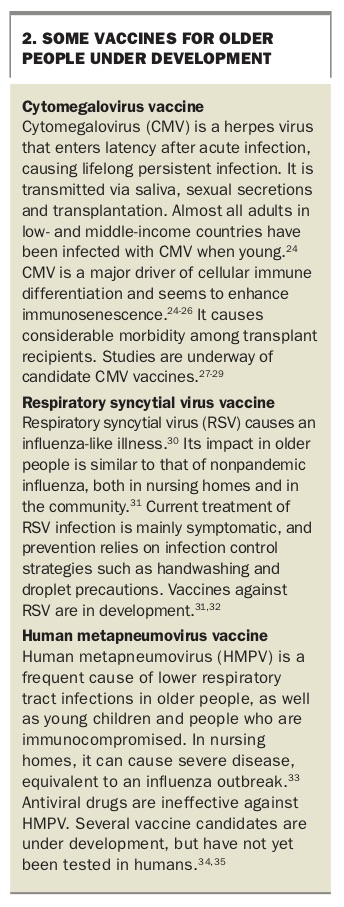
In addition, a range of vaccines are in the development pipeline against viruses responsible for considerable morbidity and mortality among older people. These include cytomegalovirus and respiratory pathogens such as respiratory syncytial virus and human metapneumovirus (Box 2).24-35
{kind=link}
Vaccines against noninfectious diseases may also become available in the future. For example, research is underway on antiamyloid vaccines to prevent or modify Alzheimer’s disease.36
Conclusion
Immunosenescence is a significant problem in older people that mandates offering them vaccines against a range of vaccine-preventable diseases. As well as influenza, pneumococcal and herpes zoster vaccines, booster vaccines against tetanus and pertussis are important in this age group.
A booster dose of tetanus-containing vaccine should be offered to all adults at age 65 years if their last dose was more than 10 years ago. Reviewing pertussis vaccination status is also recommended for all people when they turn 65 years of age, as pertussis causes considerable morbidity and even mortality in older people. Those about to become grandparents should also be vaccinated. Older travellers and older people who are employed should follow the same vaccine recommendations as their younger counterparts. MT