Dementia: how to reduce the risk and impact

Dementia
Seniors' health
This pragmatic update on prevention, diagnosis and management of Alzheimer’s disease and other types of dementia focuses on the crucial role of GPs in each phase of patient care. Minimising risk factors for dementia across the lifespan has the potential to reduce dementia incidence. Although disease-modifying therapies remain elusive for most types of dementia, current interventions can materially improve the lives of people with dementia and their families.
- Addressing risk factor modification for dementia should be considered in all patients, particularly those at higher risk.
- Memory concerns raised by patients or families should be explored rather than dismissed as an expected part of ageing.
- Early diagnosis of dementia provides benefits to patients and their families.
- A person- and family-centred approach and effective communication are key to accurate assessment and management of patients with dementia.
- Management should consider cognitive and neuropsychiatric symptoms, function, comorbidities, future planning and the needs of carers; patient preferences should be followed as far as possible.
The prevalence of dementia is increasing globally. In 2015, 47 million people were living with dementia (including 343,000 in Australia), and this number is estimated to rise to 131 million globally (900,000 in Australia) by 2050. The global cost of dementia in 2015 was estimated to be US$818 billion.1 The most common cause of dementia is Alzheimer’s disease, with other common causes being vascular dementia and dementia with Lewy bodies (DLB).
Preventing dementia
Symptomatic treatments are available for dementia. However, there are still no approved disease-modifying treatments for neuro-degenerative disorders, despite more than 200 drugs having entered at least phase II trials between 1984 and 2014.2 Consequently, focus is increasing on the possibility of preventing or delaying the onset of dementia.3
Up to 35% of an individual’s risk of dementia is potentially modifiable.4 In Australia, the most significant modifiable risk factors, in decreasing order of contribution to total cases, are:5
- physical inactivity
- midlife obesity
- midlife hypertension
- low educational attainment
- smoking
- depression
- diabetes mellitus.
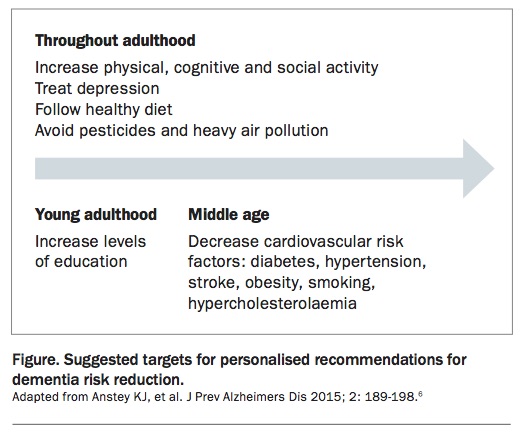
Whether dementia can be prevented still needs to be proven; however, evidence is now sufficient for us to promote protective factors for dementia risk reduction and for delaying the onset of significant cognitive decline. A review of research into risk factors concluded that ‘the evidence is now strong enough to support personalized recommendations for risk reduction by increasing levels of education in young adulthood, increasing physical, cognitive and social activity throughout adulthood, reducing cardiovascular risk factors including diabetes in middle-age, through lifestyle and medication, treating depression, adopting a healthy diet and physical activity, avoiding pesticides and heavy air pollution and teaching avoidance of all potential dangers to brain health while enhancing potential protective factors’.6 Suggested targets for dementia risk reduction across the lifespan are shown in the Figure.6 General practice and public health initiatives have a pivotal role in addressing all of these modifiable risk factors except for low educational attainment.
{kind=link}
Patients and families often ask about their risk of dementia and how they can reduce their risk. For general information on this topic, we suggest the Dementia Australia website as an informative resource (www.dementia.org.au). To assess individual risk of dementia, we direct people to the Australian National University Alzheimer’s Disease Risk Index (http://anuadri.anu.edu.au), which calculates risk and provides suggestions on risk reduction based on research.
Diagnosis of dementia
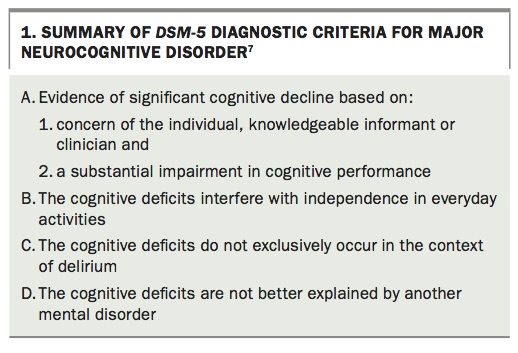
In the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), dementia is categorised as ‘major neurocognitive disorder’.7 However, most patients, families, clinicians and organisations in Australia, including Dementia Australia, continue to refer to the condition as ‘dementia’. Box 1 summarises the DSM-5 diagnostic criteria for major neurocognitive disorder.7 There is to date no definitive diagnostic test for dementia, and the diagnosis relies on clinical assessment with the aid of some investigations.
{kind=link}
Mild cognitive impairment (MCI) is considered an intermediate state between healthy ageing and early dementia, characterised by mild objective cognitive impairment without impairment of function.4 Individuals with MCI have an increased risk of developing dementia compared with those without MCI, but some individuals with MCI remain stable or revert to healthy cognition.
History taking and examination
Given the increasing prevalence of dementia with age, it is important that memory concerns are explored rather than being dismissed as an expected part of the ageing process. Early diagnosis of dementia can provide benefits to the patient and their family through use of treatments to slow cognitive decline and the ability to plan for the future, including important tasks such as organising support services, a will and enduring power of attorney, as well as consideration of driving safety.
The NHMRC guidelines for dementia recommend that patients with a possible diagnosis of dementia be referred to a memory assessment specialist or service, if available.8 Some regions have free or Medicare-funded memory clinics, with the Cognitive Dementia Assessment and Management Services (CDAMS) throughout Victoria being a good example. Many geriatricians, neurologists and old age psychiatrists offer such assessments in the private sector.
Initial assessment of patients with possible dementia in general practice should include:
- taking a history from the patient and an informant
- use of a screening tool for cognition
- physical examination
- investigations to exclude reversible causes of cognitive impairment.
These steps can be challenging given the time constraints of general practice and may require an extended consultation or a number of consultations.
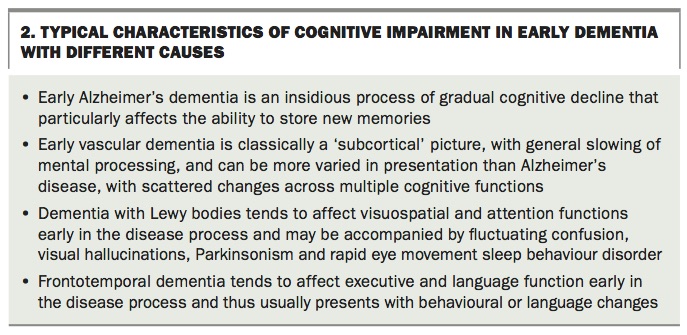
The nature and extent of cognitive impairment (whether it affects memory, orientation, language, visuospatial or executive function) should be ascertained, as this may help determine the underlying cause (Box 2). As dementia progresses, cognitive impairment becomes more generalised, and the cause becomes more difficult to differentiate. The time course of change is also important, as dementia is usually more gradual and insidious in onset than delirium, which is an acute confusional state.
{kind=link}
A history from an informant is important, as there may be aspects of cognitive impairment that patients themselves do not recognise, and some patients do not identify any problems at all. It is important to take this history sensitively. Informants should be seen separately as they may not feel comfortable discussing the symptoms in front of the patient, especially when the patient does not identify any problems.
A thorough medical history and physical examination help to exclude reversible causes of cognitive impairment. For example, there may be signs of hypothyroidism, markers of vascular risk or signs of alcoholic liver disease in a patient who has consumed excess alcohol long term. Reviewing current medications, including over-the-counter or complementary medicines, is useful to exclude medications that can contribute to cognitive impairment, such as anticholinergic medications or benzodiazepines.
A psychiatric history is also important as psychiatric conditions often impact on cognition. For example, severe depression can cause ‘pseudodementia’; in this situation, the cognitive impairment sometimes resolves with recovery from depression. Finally, family history provides valuable information, as some types of dementia have a genetic component.
Cognitive assessment
Cognitive assessment, like physical examination, begins as soon as one meets the patient. Information about a patient’s cognitive function can be obtained through general conversation and history taking. Patients may demonstrate disorientation during the interview or difficulty in recalling facts (e.g. names and numbers of grandchildren) or events or problems with retaining information.
During the formal cognitive assessment, we recommend use of a reliable validated cognitive screening tool. The results of the test should be interpreted in light of the patient’s cultural and language background, level of education, medical comorbidities, sensory impairment and presence of aphasia, which may all affect performance.
The Mini-Mental State Examination (MMSE) is one of the most commonly used tools and screens most cognitive domains apart from executive function. Asking a patient to construct a clock face and indicate a time is a relatively time-efficient way of grossly screening executive and visuospatial function. The General Practitioner Assessment of Cognition (GPCOG) is a shorter tool than the MMSE and was designed specifically for the general practice setting. An alternative tool for culturally and linguistically diverse populations is the Rowland Universal Dementia Assessment Scale (RUDAS).
Assessment of neuropsychiatric symptoms
Neuropsychiatric symptoms, also termed noncognitive symptoms of dementia, behavioural and psychological symptoms of dementia (BPSD) or behavioural symptoms, are common in people with dementia. They can occur at any time and affect up to 90% of people with dementia at some point in the course of their illness. Some symptoms are particularly associated with specific types of dementia (e.g. visual hallucinations in DLB). They tend to persist for some time but change qualitatively as dementia progresses and may remit as dementia advances.
The European Alzheimer’s Disease Consortium divides neuropsychiatric symptoms into four classes:9
- psychotic symptoms (delusions, hallucinations and rapid eye movement [REM] sleep disorder)
- affective symptoms (depression and anxiety)
- hyperactivity (motor restlessness, agitation, aggression, disruptive vocalisation)
- apathy.
Neuropsychiatric symptoms are often associated with greater functional disability, earlier move to residential care and distress for both individuals and carers.10 As such, and as recommended by Australian guidelines, specific review of these symptoms is an important component of any comprehensive dementia assessment.11
The ABC (antecedent, behaviour, consequences) model is a recommended approach to assessment. It prompts consideration of the antecedents of behaviour, the behaviour itself and its consequences.12 This model helps healthcare professionals identify targets for prevention or management.
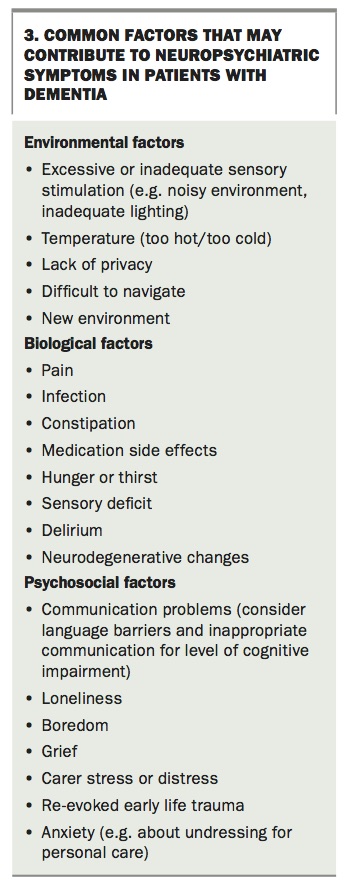
Assessment should produce an individualised understanding of specific contributing factors. This includes consideration of pain, other medical issues and other unmet needs, such as hunger, thirst, cold, sensory deprivation and inadequate social stimulation. Where symptoms are of acute or subacute onset, the medical review must rule out delirium and other medical conditions. Common environmental, biological and psychosocial factors that may contribute to neuropsychiatric symptoms in dementia are summarised in Box 3.
{kind=link}
Finally, assessing the consequences of behaviour is important but frequently missed. It is relatively common to find that the response of family, care staff or others inadvertently reinforces the behaviours that they are trying to manage.
If symptoms cause significant risks or are difficult to analyse then referral to specialist services such as Dementia Support Australia or local mental health services for assessment is recommended.
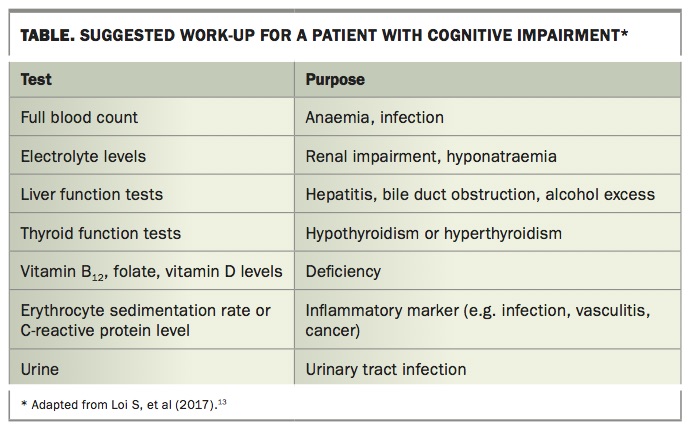
Investigations
It is important to assess for reversible causes of cognitive impairment. Suggested investigations that should be considered in the work-up of a patient with possible dementia are shown in the Table.13
{kind=link}
Brain imaging is another important part of the work-up of patients with cognitive impairment. Ideally, this is with MRI, including coronal views to visualise the hippocampus, but CT can be used where MRI is not an option. Where there is diagnostic uncertainty, functional imaging such as single photon emission CT (SPECT) or positron-emission tomography (PET) may be considered. Amyloid scans are not commonly available in Australia outside research settings.
Management
Effective and future-focused management for people with dementia and their families can significantly reduce the impact of the syndrome on quality of life. Comprehensive management should address cognitive and neuropsychiatric symptoms, physical comorbidities and the functional, psychological and social consequences of symptoms. Further, regular review is crucial to adapt strategies and address new issues as dementia evolves.
The guiding principle for dementia management is person-centred and family-centred care. This means engaging individuals with dementia and, where appropriate, their families in tailoring interventions to their individual needs and priorities and in promoting continued independence. It requires sufficient time and dementia-specific communication skills to be properly implemented.
Optimal care for people with dementia is usually a partnership between GPs, medical specialists and other health professionals involved in psychosocial support services. Specialist memory services in Australia usually refer individuals back to GPs for ongoing management after making a diagnosis.
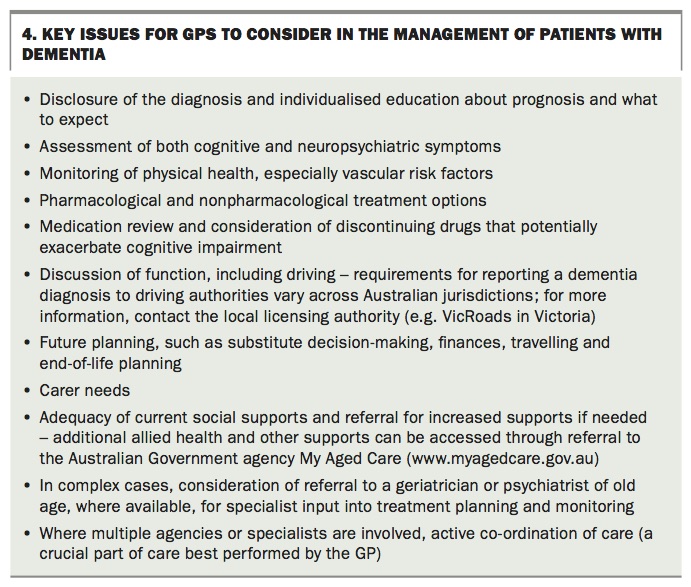
Key issues for GPs to consider when managing a patient with dementia are listed in Box 4. We will discuss some aspects of management in more detail. Dementia Australia provides extensive information to support health professionals working with people with dementia (www.dementia.org.au).
{kind=link}
Cognitive symptoms and functional decline
Pharmacological interventions
Two classes of medication are currently available that may at least temporarily improve cognition and function for some individuals with dementia.
Cholinesterase inhibitors
Cholinesterase inhibitors may benefit cognition and function in patients with mild-to-moderate dementia due to Alzheimer’s disease.4 Evidence also suggests beneficial effects in patients with DLB, Parkinson’s disease dementia, more severe Alzheimer’s disease and, to a limited degree, vascular dementia, although these indications are not covered by the PBS.14-16
Cholinesterase inhibitors approved for patients with Alzheimer’s disease include donepezil, rivastigmine and galantamine. These three agents show similar efficacy and side effects but differ in presentation (pills, patches, liquid or capsules), which may impact on side effects. Common or significant side effects include nausea, vomiting, diarrhoea, dizziness and falls, urinary frequency and incontinence, muscle cramps, weight loss, anorexia, headache, vivid dreams, drooling and excessive sweating. They may also cause bradycardia, occasionally precipitating heart block. About one in eight treated patients are unable to tolerate a cholinesterase inhibitor because of adverse effects.17
A review of physical health that includes body weight, a falls risk assessment and an ECG should be completed before commencing a cholinesterase inhibitor. An opinion from a cardiologist is recommended if there is significant pre-existing cardiovascular disease. Regular review to monitor for side effects and effectiveness is also imperative, particularly as improvement in cognition, neuropsychiatric symptoms and/or quality of life must be demonstrated by six months for PBS-subsidised treatment to continue. As most side effects occur early after drug commencement or at dose increase, education for families and instructions for them to follow in the event of symptoms developing is also prudent. Finally, these medications may diminish the effectiveness of some muscle relaxants used during surgery and may need to be stopped preoperatively Anaesthetic consultation is recommended.
Memantine
In Australia, memantine is available on the PBS only for patients with moderately severe Alzheimer’s disease. However, there is some evidence of benefit to cognition in those with mild-to-moderate dementia, and it is often prescribed for this off label, either in combination with a cholinesterase inhibitor or as an alternative agent when cholinesterase inhibitors are not tolerated.4 Memantine is generally well tolerated, although it can cause sedation (usually accommodated by evening administration), headache and gastrointestinal adverse effects. It may also lower the seizure threshold, and a history of epilepsy or seizures should prompt discussion with the patient’s treating neurologist before commencement.
Prescribing details
Both cholinesterase inhibitors and memantine are commenced at a low introductory dose. The dose is gradually increased if tolerated, usually after a month for a cholinesterase inhibitor and over three weeks for memantine.
Decisions about stopping therapy may be influenced by PBS restrictions on dual therapy. As the PBS does not subsidise concurrent treatment with a cholinesterase inhibitor and memantine, the cholinesterase inhibitor must be stopped to obtain a PBS subsidy for memantine. However, a well-conducted study found convincing evidence that cessation of cholinesterase inhibitors in patients with moderate-to-advanced dementia may be associated with accelerated cognitive, functional and behavioural decline.16 Concurrent cholinesterase inhibitor and memantine therapy is safe and may offer some additional benefits for cognition.18
Evidence does not support the use of either cholinesterase inhibitors or memantine in patients with MCI.19
Nonpharmacological interventions
Numerous nonpharmacological interventions to improve cognition and function, particularly in patients with mild dementia, have been investigated or marketed. The evidence base supporting these is often limited.4 However, interventions with promising results include:
- occupational therapy programs
- group-based cognitive stimulation incorporating both cognitive activities and social interaction
- cognitive rehabilitation, with the setting of specific functional goals and support for individuals to develop strategies to achieve these
- some forms of cognitive training.4
Some of the principles underlying these interventions have been incorporated into Australian Government home care support packages and into the activities scheduled in some residential aged care facilities.8
Physical activity has broad health and functional benefits. Despite limited evidence of cognitive benefits in dementia, it should be recommended.20,21
Similarly, several vitamins, nutritional drinks (e.g. Souvenaid) and other dietary supplements have been postulated as of potential benefit. Again, more evidence is needed to establish a clearer picture of their role within a management plan.22,23 If individuals are considering using supplements or other complementary therapies then healthcare professionals should ensure consideration of potential side effects and drug interactions, as for other pharmacological agents.
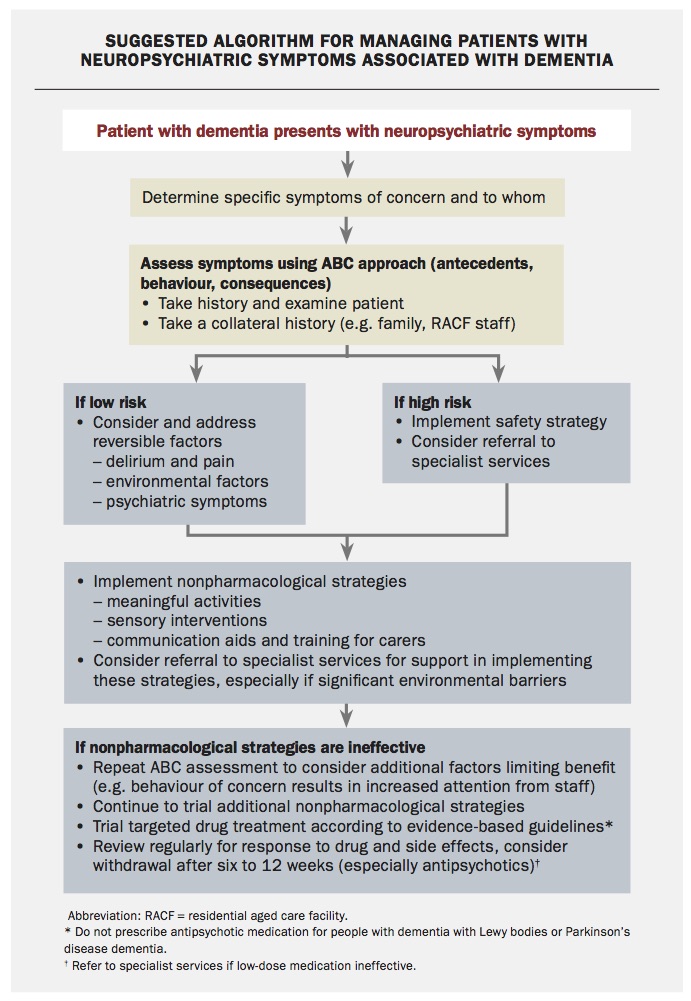
Neuropsychiatric symptoms
As noted, thorough assessment using the ABC model, effective communication and individualised treatment plans are key to successful management of patients with neuropsychiatric symptoms. A suggested algorithm to assist in management is shown in the Flowchart.
{kind=link}
Usually nonpharmacological strategies should be first-line interventions, and medication should be reserved for situations in which neuropsychiatric symptoms are severe or associated with significant risks. Specialist support is often required for patients with moderate-to-severe neuropsychiatric symptoms. As noted above, Dementia Support Australia can provide specialist assessment and treatment recommendations, including telephone and face-to-face consultations, including for crisis situations (Box 5).
{kind=link}
Nonpharmacological interventions
Where possible, any environmental, biological or psychosocial factors identified as contributing to neuropsychiatric symptoms should be addressed or eliminated (Box 3).
Nonpharmacological interventions are most effective when they are personalised and multicomponent, such as engaging the individual in multiple meaningful activities that reflect the leisure or recreational activities they enjoyed earlier in life.11 The best supported individual interventions are:
- engagement in meaningful activities
- sensory interventions (e.g. hand massage, multisensory rooms)
- communication training for family and care staff.4,11
Individual interventions should be implemented only as a trial, with a review of their effectiveness and adaptation as dementia progresses.
Other interventions with some supporting evidence include:
- doll, robotic animal or pet therapy
- reminiscence therapy
- music and dancing
- exercise
- simulated family presence (using recordings)
- some psychotherapeutic approaches for depressive symptoms.11
Choice of strategies should be guided by applicability to the individual (e.g. doll therapy for a person who strongly identified with a parental role in earlier life). Input from specialist dementia services or specifically trained residential aged care facility staff may aid implementation trials.
Pharmacological interventions
Pharmacological interventions for neuro-psychiatric symptoms should be reserved for patients with symptoms that are distressing for them or associated with significant risks. A prior discussion should be held if possible with the patient or family, in which target symptoms are identified and risks of medication are discussed. In particular, this discussion must include the side effects and risks of antipsychotics in people with dementia, including increased risk of death and stroke, especially during the early stages of treatment, worsening of cognitive impairment, sedation, parkinsonism and falls.
All medications should be introduced on a trial basis. Antipsychotic medication in particular should be commenced at a low dose and slowly increased, with review within a week for tolerability, a month for effectiveness and three months to determine whether ongoing treatment is necessary.
Specific pharmacological interventions for neuropsychiatric symptoms include the following.
Cholinesterase inhibitors
Cholinesterase inhibitors may be of benefit for psychotic symptoms (particularly hallucinations) in DLB and potentially for apathy in dementia generally, although evidence for the latter is limited.4,24
Risperidone
Risperidone 0.5 to 1 mg may be of benefit in patients with severe psychotic symptoms and aggression.11 In addition, risperidone is the only antipsychotic medication that is PBS listed for psychosis in dementia. Importantly, antipsychotic medication should not be prescribed to patients with DLB without specialist input.
Antidepressants
Some antidepressants may be indicated for anxiety and agitation. Australian guidelines recommend a trial of a selective serotonin reuptake inhibitor (SSRI) such as escitalopram if agitation is severe or does not respond to nonpharmacological interventions.12 Mirtazapine is also supported as potentially providing benefits for anxiety and agitation in dementia.25 Side effects to consider for both escitalopram and mirtazapine include exacerbating cognitive impairment, falls and hyponatraemia.11
Although depression is common in people with dementia, it is likely heterogeneous, and antidepressant medication may be ineffective for depression in many people.25,26 Antidepressants to treat depression should be reserved for patients with severe depression or where there is a pre-dementia history of depression (especially if it was severe or responded well to antidepressant treatment).
Melatonin
Melatonin may be of benefit for sleep and is safer than benzodiazepine-related hypnotics. However, more evidence is needed, and it is not subsidised by the PBS.27
Ginkgo biloba extract
There is some evidence, albeit preliminary, that Ginkgo biloba extract EGb 761 (daily dose 240 mg) may be of benefit for some neuropsychiatric symptoms in patients with mild-to-moderate dementia, including depression, anxiety and irritability.28 The clinical relevance of the improvements remains uncertain. As noted above for use of complementary therapies to treat cognitive symptoms, health professionals must consider potential side effects and drug interactions and provide an individualised risk-benefit assessment before any trial of complementary supplements such as G. biloba.
Support for carers
The challenges in caring for any individual with dementia are significant and can adversely affect carer mental and physical health. Carers are at increased risk of distress, depression and anxiety, physical health problems and diminished quality of life.29,30 These symptoms, in turn, may be associated with adverse outcomes for the person with dementia, including early move to residential aged care and risk of elder abuse.31,32
Regular checks with carers about how they are coping are crucial to ensure access to appropriate supports. There are many levels of support available, including peer support networks, educational interventions, telephone crisis supports and psychotherapy. Dementia Australia, Carers Australia and local councils are good places to connect to. Carers with more significant depression or anxiety may require referral to a psychiatrist. If elder abuse is suspected then this must be reported. The Australian Government’s My Aged Care website lists appropriate organisations to contact in each Australian jurisdiction (www.myagedcare.gov.au).
End-of-life care
A palliative approach to dementia care is recommended, acknowledging that dementia does shorten life.4,11 Ideally, an individual’s wishes for end-stage dementia care should be established early in the course of the illness through advance care planning. Early identification of end-stage dementia then allows advance care directives to be followed or, if advance care planning has not occurred, it allows family and health professionals to establish common goals for end-of-life care.
End-stage dementia should be managed according to usual palliative care and good nursing principles, accommodating the specific challenges that arise because of cognitive impairment. In particular, communication difficulties mean that individuals with dementia may not be able to communicate their needs. Again, good person-centred care and effective communication are key to good palliative care in dementia. It is often of benefit to involve a community palliative care service.
The UK Gold Standards Framework in End of Life Care has produced simple and useful clinical practice tools to help health professionals identify patients who are nearing the end of life in the setting of various conditions including dementia, and to anticipate their likely future needs.33 These are available from the Gold Standards Framework website (www.goldstandardsframework.org.uk).
Conclusion
Dementia is a common, complex syndrome with significant consequences for individuals, families, healthcare services and societies. It is, however, not an inevitable outcome of ageing. Primary care, in partnership with specialist services and supports across health and community care, has a crucial role in the prevention, diagnosis and management of dementia that can materially reduce the impact of this syndrome. MT
Acknowledgements
The authors would like to thank Emeritus Professor David Ames, University of Melbourne, for advice in the preparation of this article. The authors also acknowledge funding received by the Academic Unit for Psychiatry of Old Age from the NHMRC Centre for Research Excellence in Cognitive Health.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.