Sudden cardiac death in athletes: what is the role of pre-participation screening?
Sudden cardiac death during exercise, most commonly caused by a lethal arrhythmia, is always a tragic event. There is interest in the role of pre-participation screening to prevent these rare occurrences, but the evidence for its effectiveness is not conclusive.
The health benefits of regular exercise for both physical and mental health are irrefutable. With rare exceptions, the most useful prescription for people with stable cardiovascular disease is exercise. However, the stress of exercise may unmask unrecognised cardiac disease resulting in a cardiac event, with the worst outcome being sudden cardiac death (SCD). SCD during exercise, which is most commonly caused by a lethal arrhythmia, is a rare but always tragic event. In younger individuals (under 35 years of age), inherited conditions such as a cardiomyopathy or channelopathy are the most commonly identified causes, but the events often remain unexplained even after autopsy. In older individuals, atherosclerotic coronary artery disease becomes the most common cause of SCD, and it also accounts for a proportion of deaths in the younger population.
Following an unexpected SCD in an overtly healthy young individual, it is intuitive to ask whether anything could have been done to prevent it. Worldwide, many countries have established protocols and programs to screen athletes in an attempt to identify at-risk individuals before a tragic event occurs. Although the evidence for such approaches is not solid, there has been growing momentum and pressure to adopt these screening strategies more broadly.
What is needed for an effective screening program?
Putting aside the emotional desire to do anything possible to prevent SCD during exercise, it is important to pause and consider whether the current screening approaches are effective in preventing deaths and, if so, whether they are cost-effective. There are published WHO criteria for an effective screening program against which cardiac screening of athletes needs to be considered.1 The principles were originally developed for communicable diseases rather than inherited cardiac disease, but they remain relevant in any screening program. Pre-participation screening of athletes is a form of selective screening.
Screening principle: ‘The condition sought should be an important health problem’
For an affected individual who suffers a cardiac arrest during sport, the condition is obviously important. But how important is this for society as a whole? Estimates of the incidence of exercise-related SCD vary across the globe, depending on case finding strategies and cohorts studied, and vary between 0.76 and 6.8/100,000 athlete-years.2-6 In comparison, the rate of suicide in Australian males aged between 15 and 35 years ranges between 17.3 and 23.2/100,000 persons per year.7 In addition, SCD during or after exercise in young people is actually quite uncommon when compared with the much higher rates of SCD during sleep or at rest.8 Although the ratio of deaths during exercise vs sleep/rest may be underestimated (because exercise time represents a much smaller proportion of one’s day), it is still a very rare occurrence. While rare events still require consideration, this does place this problem into perspective, particularly when the efficacy of screening is still inconclusive.
Screening principle: ‘There should be a suitable test or examination’
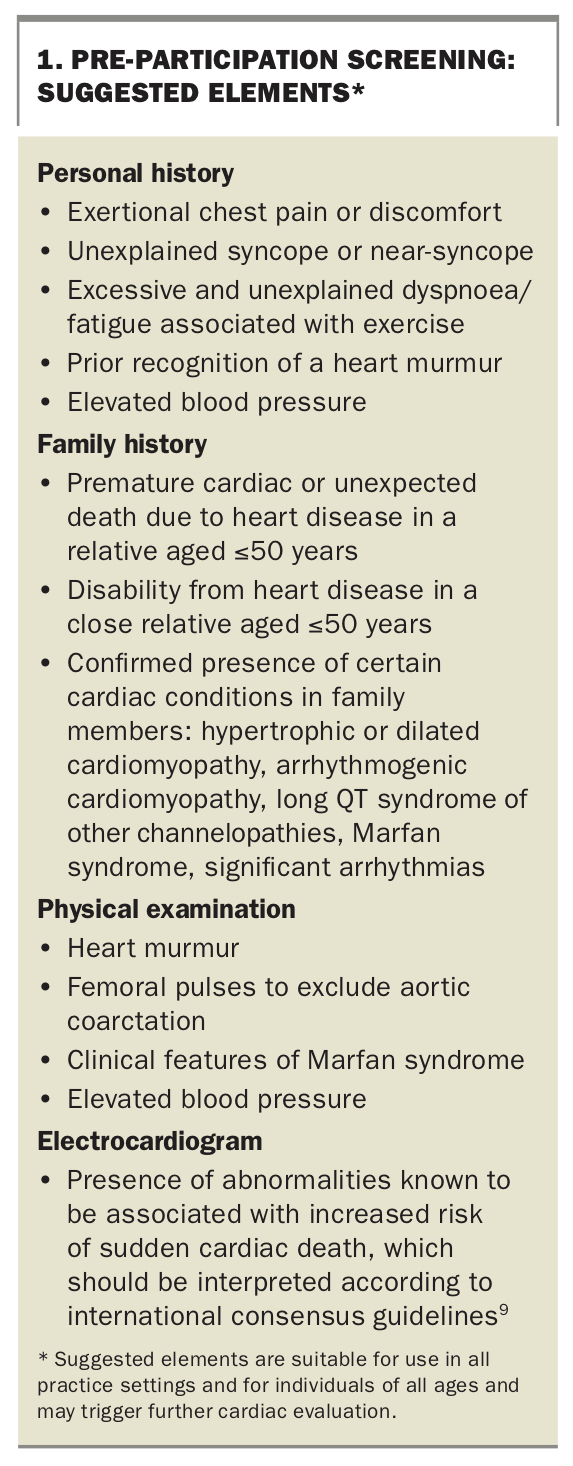
Suggested elements of a pre-participation screening assessment to identify which athletes require further cardiac evaluation are listed in Box 1. Strategies for pre-participation screening of athletes vary across the globe. A clinical history and physical examination are recommended in all guidelines. The inclusion of a resting 12-lead ECG has had a large ground swell despite the limitations, which are addressed in part below. A personal history of symptoms that may reflect occult cardiac disease such as syncope or pre-syncope, chest pain, abnormal dyspnoea or palpitations – particularly in association with exercise – should be included in the assessment. In addition, a family history of known cardiac disease, SCD or unexplained death at a young age (such as drowning or a single motor vehicle accident) should be sought. Examination should focus on valvular disease and characteristics of Marfan syndrome.
{kind=link}
A 12-lead ECG is recommended for screening in some countries. Early attempts at ECG screening were plagued by very high false-positive rates due to misinterpretation of ECG changes, which are now understood to result normally from athletic training as a positive ECG finding, and resulted in excessive downstream testing. There is also significant variability in interpretation despite guidelines – even in relatively expert hands – although refinements in criteria for normality have improved this.10,11 Most recently, use of the international consensus criteria has been shown to result in a false-positive rate of less than 5% without any apparent loss in sensitivity.9 However, this still results in a significant number of secondary tests, most commonly echocardiography, to further evaluate positive test results. Despite improvements in the interpretation of ECGs in athletes over the past two decades, the rate of accurate detection of latent disease in an asymptomatic population with low pre-test probability is, not surprisingly, low (around 0.2%).11
Even with the use of autopsy in cases of SCD, the cause in young people may not be explained in up to 40% of cases.8 Family screening and genetic analysis may increase the number in whom a diagnosis is made, but inability to reach a clear diagnosis in a significant proportion of those who die even with very sophisticated investigations raises questions about our ability to do this in the living through widespread screening.
Screening principle: ‘There should be an accepted treatment for patients with recognised disease’
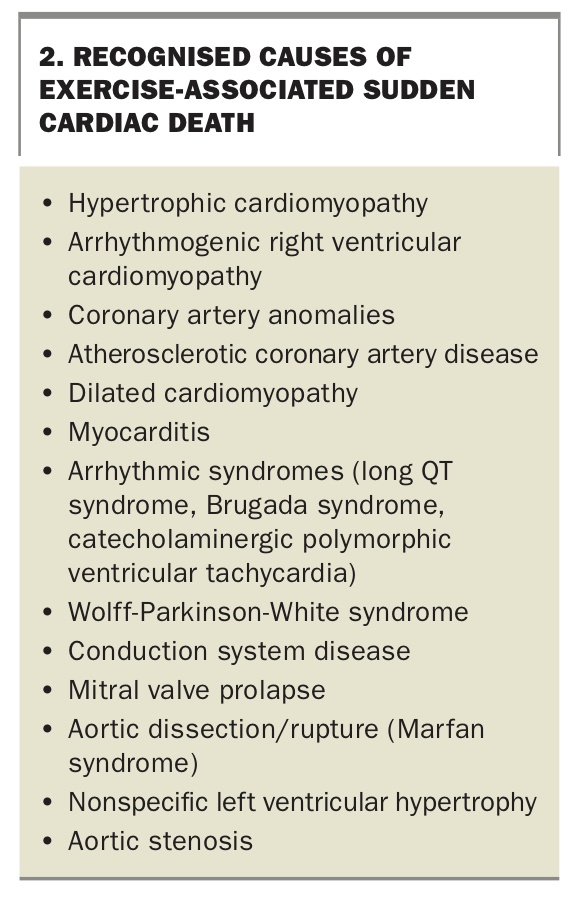
Recognised causes of exercise-associated SCD are presented in Box 2. It is likely that both the genetic characteristics of the population and the expertise and interests of diagnosing pathologists are significant influences on the reported frequency with which particular diseases cause SCD. For example, the reported relative importance of arrhythmogenic right ventricular cardiomyopathy (ARVC) and hypertrophic cardiomyopathy (HCM) vary substantially.12 In Italy, ARVC has been reported to account for 24% and HCM for 2% of exercise-associated SCD, whereas in the USA, HCM has been reported to account for 36% and ARVC only 4%.3,13
{kind=link}
For patients identified as having a cardiac condition with a risk of SCD, the most common intervention is exclusion from competitive sports participation. One example of the utility of this intervention is for ARVC, where exercise not only increases the risk of SCD but also causes more rapid progression of the disease.14,15 For other conditions, diagnosis may result in commencement of medications, cascade screening of other family members and, sometimes, further procedures or device implantation. However, in the context of asymptomatic screening, identified cases of other (more common) conditions fall into a lower risk profile where sports restriction likely offers no benefit and comes with the longer term adverse impacts of a sedentary lifestyle.
What has not been proven in a randomised setting is that routine screening of athletes prevents SCD during sports. Observational studies have had conflicting results. Experience from the Veneto region of Italy, on which the push for pre-participation screening has largely been based, reported a reduction of 89% in the incidence of SCD in athletes after the introduction of screening.2 However, the time period that was considered prior to the initiation of screening was only two years (1980 and 1981), when there were six deaths/year in the athletic population in that region (around 3/100,000 athletes). In subsequent years, the incidence was closer to one death/year (less than 1/100,000), which is very similar to that reported in parts of the world where screening is not undertaken. Thus, the reported 89% drop in incidence may reflect regression to the mean. Indeed, a large observational study in Israel showed no effect of the introduction of compulsory screening on SCD during sport.4 Furthermore, there are many well publicised cases of athletes who have been screened on multiple occasions but suffer SCD during exercise. In the UK, researchers reported eight cases of SCD over a 10-year period in 11,000 young soccer players who had all undergone screening with clinical history and examination, ECG and echocardiography.6 Six of those eight cases (75%) had had normal screening results, which provides further evidence for the limitations of screening.
Screening principle: ‘There should be a recognisable latent or early symptomatic stage’
Unfortunately in many cases, the first symptom of an underlying cardiac problem is SCD without any clear warning. Much of the challenge in pre-participation screening of athletes is that the latent stage, or even manifest disease, may be undetectable by means such as ECG or a concerning finding on clinical history or physical examination. The ECG will be normal in patients with coronary artery disease and no prior infarction and also in up to 10 to 20% of subjects with HCM or ARVC. ECG changes in channelopathies are more subtle and do not always manifest as overtly abnormal ECGs, with diurnal and age/sex related changes occurring in these conditions. Furthermore, the accuracy of testing to identify each abnormality during this stage is critical and very much interpreter dependent.
Who should be screened?
An athlete can be defined in a number of ways. Most working definitions include regular training to improve performance, participation in regular competition against others and a high premium being placed on athletic excellence. Where the line is drawn between ‘athlete’ and ‘exerciser’ and how this interacts with planned screening is a matter of some ongoing debate across the globe. The current Australasian College of Sport and Exercise Physicians’ Position Statement on Pre-Participation Cardiac Evaluation in Young Athletes, which is available online, recommends screening of elite athletes only (see https://www.acsep.org.au/page/resources/position-statements/position-statements).16 One setting in which cost-effectiveness may be less relevant is the world of professional sports, where an employer may have obligations to ensure a safe working environment for the athlete and systematic screening is likely to continue in this setting. For most doctors, particularly those in general practice, it is important to be aware that SCD can occur with exercise and to be alert to patient symptoms that should prompt more detailed evaluation for underlying cardiac disease (Box 1).
Is there an alternative strategy for preventing sudden cardiac death in athletes?
Given that the majority of exercise-associated SCD events involve arrhythmic cardiac arrest, commonly ventricular fibrillation, one alternative to widespread screening is to have defibrillators present with appropriately trained personnel at both training and competition locations to treat people who have arrhythmic episodes. This may be beneficial not only to competitors, but also coaches and spectators alike. This approach is well suited to team sports played on a court or field, but more difficult to implement with some other forms of exercise, such as cycling, long-distance running and rowing. The effectiveness has not been compared with screening, but the economic burden is almost certain to be less than that of widespread screening and may therefore have a positive impact on cost-effectiveness.
Conclusion
SCD in young athletes is a tragic and emotive event. However, conclusive evidence for the effectiveness of selective screening of athletes to prevent these rare occurrences is lacking and does not meet the WHO criteria for an effective screening program. Even after autopsy, the causes of SCD remain unknown in up to 40% of cases, and death may occur in asymptomatic young people with no prior symptoms and no manifest disease on ECG or even echocardiography performed prior to cardiac arrest. Because of the rarity of these events, it is unlikely that any large randomised trial will ever by undertaken to resolve this dilemma, and thus many in the sports cardiology field have adopted the position that screening is necessary on medical, ethical and legal grounds.17 If screening is to be undertaken, however, it is important that doctors involved in evaluating the athletes clinically and in interpreting their investigations have specific training and understand the normal findings seen in trained athletes to avoid unnecessary downstream testing or inappropriate exclusion from competition. More widespread availability of trained first responders and defibrillators may be a more effective and cost-effective approach to the prevention of SCD in athletes. MT
COMPETING INTERESTS: None.
References
http://apps.who.int/iris/bitstream/handle/10665/37650/WHO_PHP_34.pdf (accessed April 2022).