CrossFit: risk vs reward in the ‘sport of fitness’

Now in its third decade, CrossFit is a ‘sport of fitness’ designed to help participants achieve the physical activity levels recommended by the WHO for optimal health at any age. However, there are some concerns about injuries related to high-intensity conditioning programs such as CrossFit. This article investigates these concerns.
CrossFit began in 1995 when founder and former gymnast Greg Glassman opened the first CrossFit gym in Santa Cruz, California. The first CrossFit affiliate gyms followed in 2003. Seventeen years later, CrossFit is one of the fastest-growing high-intensity functional training models in the world.1 According to Glassman, CrossFit is a ‘sport of fitness’, defined by its ‘constantly varied, high-intensity functional movement’.2 Originating as a core-strength and conditioning program, it was designed to achieve competence in 10 fitness domains: cardiovascular and respiratory endurance, stamina, strength, flexibility, power, speed, co-ordination, agility, balance, and accuracy.2
Sport or training?
By 2020, CrossFit has become both a sport and a training method. Some people’s sole purpose for training is to become better at the sport of CrossFit, while a select few are professional athletes, making their living from the sport. Most ‘CrossFitters’, however, are everyday people who attend CrossFit classes to enhance their fitness and health. Physical inactivity is now identified as the fourth leading risk factor for global mortality.3 In this ‘exercise is medicine’ era, a CrossFit class is considered by many to be an enjoyable option for meeting the WHO global guidelines on the amount of physical activity needed for health and the primary prevention of noncommunicable diseases.3 The recommended amount of moderate intensity exercise of 150 minutes per week can easily be achieved by attending three CrossFit classes, and the two to three days of resistance training advised can be met by an additional one to two classes per week. Thus, CrossFit serves as a one-stop shop for all the cardiovascular, strength, balance and flexibility training suggested by the WHO for optimal health at any age.
To participate in a class at one of the CrossFit affiliates, an individual may be required to combine weightlifting (snatch, clean and jerk, squats, deadlift) and gymnastic movements (on pull-up bars and gymnastic rings) with a form of cardio exercise (running, rowing, riding or skiing). Other common training methods include the integration of dumbbell and kettlebell movements and skipping rope.
However, only the top few per cent of CrossFit participants would be able to perform these movements exactly as prescribed. The rest would scale or modify the movements to achieve suitable functional outcomes at a less technical capacity or lighter load. This is the feature that makes CrossFit suitable for people of all ages and abilities, including those with disabilities or chronic injuries or impairments that might prevent them from participating in other forms of physical activity.
Measurement and accountability
Unique to CrossFit training, compared with other forms of high-intensity interval training, is the scoring system, where participants record on a whiteboard the time taken to complete a workout and how many rounds or repetitions they completed in the specified time. This concept was born from the idea that recording something keeps people accountable and motivated, whether they are ‘competing’ against themselves, the clock or a training partner. It also makes workouts measurable over time, so participants can compare their time when performing the same workout again a year later, to see how much their fitness has improved.
This scoring system is also what has triggered most of the criticism of CrossFit – the perception that participants are trying to move as fast as possible during their training, sometimes at the expense of form and to the detriment of their body. However, this was never the intention of the sport and the Level 1 CrossFit Training Guide (as well as the two-day course that all CrossFit coaches must attended) promotes the message that technique is pivotal to success.2 ‘Technique is an intimate part of safety, efficacy and efficiency,’ is the motto that is drilled into all CrossFit affiliate owners and coaches right from the start.2
Concerns about high-intensity conditioning programs such as CrossFit are highlighted in a consensus paper produced by the Consortium for Health and Military Performance and American College of Sports Medicine, which concluded that although positive influences on body composition and physical fitness were recognised, there was a ‘disproportionate musculoskeletal injury risk from these demanding programs, particularly for novice participants, resulting in lost duty time, medical treatment and extensive rehabilitation’.4
Although there is limited research currently available on CrossFit injury rates, some studies have tried to examine this statistic more objectively. A recent review in the Journal of Sport Rehabilitation looked at whether injuries are more common with CrossFit training than in other forms of exercise.5 From this literature review that initially yielded more than 100 articles, three level 2b retrospective cohort studies were of high enough quality for analysis. ‘In all 3 reviewed studies, the reported incidences of injuries associated with CrossFit training programs were comparable or lower than rates of injury in Olympic weightlifting, distance running, track and field, rugby, or gymnastics,’ the authors concluded.5
Risk of injury
A recent study of injury patterns among Dutch CrossFit athletes – via an online survey distributed to all 130 CrossFit gyms in the Netherlands – found the most common injuries were to the shoulder, lower back and knee.6 The only independent variable associated with an increased risk of injury was the duration of previous CrossFit participation, with those who had been participating for less than six months significantly more likely to sustain an injury than those who had been participating for more than two years. Most of the injuries were caused by overuse. This finding was echoed in a similar study conducted in the US state of Florida, in which the most frequently injured locations were found to be the shoulder, knee and lower back.7
Although acute injuries do occur in CrossFit, as with any other sport, chronic, insidious overuse injuries are far more common. More often than not, chronic activity-related pain stems from a dysfunction within the kinetic chain and management needs to address all possible deficiencies in the chain, not just the area of pain. For example, shoulder pain may be related to scapular dyskinesis or to cervical and thoracic spine dysfunction, while knee pain may stem from overload secondary to restricted hip range of motion, gluteal weakness and poor core stability. Thus, although any CrossFit enthusiasts presenting to primary care with pain during movement need to have their injury assessed and managed, there are still many activities they can continue to do to fulfil their exercise targets.
A common example is a patient presenting with anterior shoulder pain after overhead exercises. A thorough history taking and examination needs to be performed in order to rule in or rule out common causes of shoulder pain such as glenohumeral instability, rotator cuff dysfunction, tendinopathy or tear, acromioclavicular or glenohumeral osteoarthritis and adhesive capsulitis. Referral to a sports physiotherapist or sports and exercise medicine physician may be indicated and there may be a need for further investigations such as x-rays or MRI. Often, there may be no clearly identifiable injured structure. This is when many patients are told to rest until the pain goes away – except that it never really goes away and when they return to the same activity that caused their pain, the pain returns too.
Specific to the shoulder, factors such as altered scapular recruitment patterns and muscle performance as well as flexibility deficits in the surrounding soft tissues may restrict normal scapular movement and lead to shoulder or neck pain with certain overhead exercises. During episodes of pain, there is a redistribution of activity within and between muscles, which may have a short-term benefit of protection from further pain and injury but a long-term potential for adverse mechanical consequences to pain sensitive tissues.8
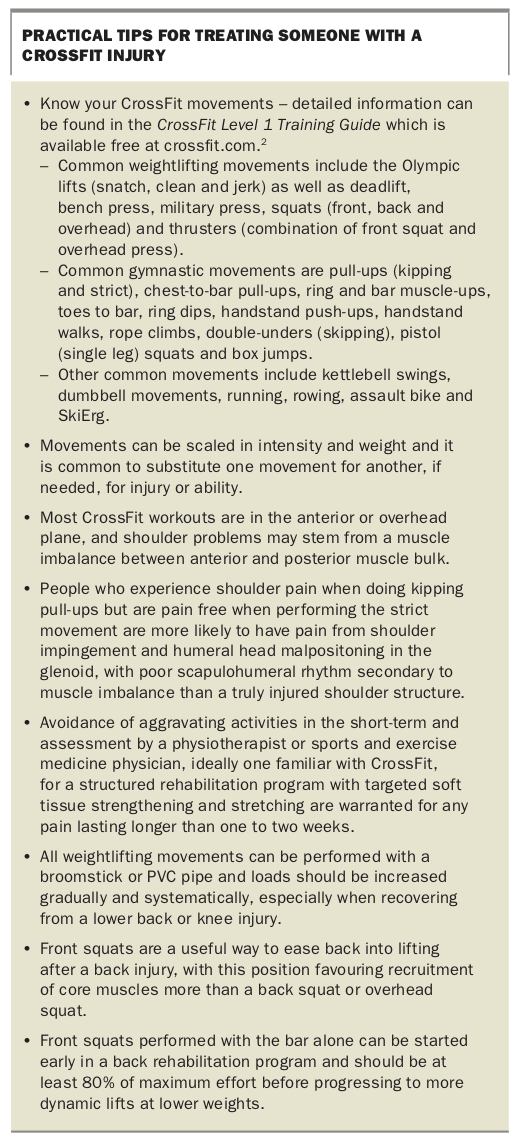
At this stage, the athlete is likely to need to refrain from movements such as snatch, overhead press and jerk movements as well as pull-ups and hanging from the rings, but may easily be able to substitute these with squats, deadlifts, sit-ups and rowing (a suitable movement substitution for most anterior shoulder pain) while their pain is being investigated (Box). This management approach is far more likely to result in patient adherence to treatment than a simple ‘stop all activity or change sport’ approach. Forming a partnership with a local physiotherapist familiar with CrossFit movements (ideally, a CrossFit participant themselves) will help distinguish between patients who need some simple adjustments to strength and flexibility exercises and those who warrant further investigation by a sports and exercise medicine physician.
{kind=link}
Conclusion
On the one hand, CrossFit serves as a one-stop shop for all the cardiovascular, strength, balance and flexibility training necessary for optimal health at any age as recommended by the WHO. On the other, concerns have been raised about injuries related to high-intensity conditioning programs such as CrossFit. A review of the current literature on the risks and rewards associated with this ‘sport of fitness’ shows that although acute injuries do occur in CrossFit, as with any other sport, chronic, insidious overuse injuries are far more common.
Hence, although any CrossFit enthusiasts presenting to primary care with pain during movement need to have their injury assessed and managed, there are still many activities they can continue to do to fulfil their exercise targets; if necessary, with oversight by a physiotherapist or sports and exercise medicine physician. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.