Type 2 diabetes in pregnancy. A multidisciplinary approach to improving outcomes

Diabetes type 2
Type 2 diabetes in pregnancy is becoming more common and is associated with poor maternal, fetal and childhood outcomes. Preconception counselling and a multidisciplinary team approach throughout pregnancy are crucial to improving outcomes.
- The prevalence of type 2 diabetes in pregnancy is increasing, and is associated with adverse pregnancy outcomes.
- Uptake of preconception counselling is low, and strategies are needed to ensure all women with type 2 diabetes have access to preconception care, as it is associated with improved outcomes.
- Management of women with type 2 diabetes in pregnancy needs a multidisciplinary approach, including review by a dietitian and diabetes educator.
- All women with type 2 diabetes should be screened for complications of diabetes early in pregnancy, with further review depending on risk.
- High-dose folic acid should be given to all women with type 2 diabetes in pregnancy until 12 weeks’ gestation to decrease the risk of neural tube defects. Low-dose aspirin should also be considered, starting before 16 weeks’ gestation, to decrease the risk of preterm pre-eclampsia.
The prevalence of type 2 diabetes in young women is increasing and, consequently, type 2 diabetes in pregnancy. In Australia, about 1% of all pregnancies are complicated by known pre-existing diabetes, with local variations depending on the ethnicity of the population studied.1 At least half of these women have type 2 diabetes and the prevalence is rising.
Women with type 2 diabetes tend to be older, be overweight and/or obese, have a lower socioeconomic status and be from certain ethnic groups (e.g. Indigenous Australians), therefore cultural or language barriers may need to be overcome.2
This article discusses ways to improve outcomes in pregnant women with type 2 diabetes by increasing uptake of preconception counselling, optimising glycaemic control, screening for diabetes complications, reviewing medication use during pregnancy and using a multidisciplinary team approach.
Definition
Type 2 diabetes in pregnancy may be diagnosed by measurement of glycosylated haemoglobin level ([HbA1c] of ≥6.5% [≥48 mmol/mol] is considered diagnostic) or by an oral glucose tolerance test ([OGTT] a fasting blood glucose level [BGL] of ≥7 mmol/L and/or a two-hour BGL of ≥11.1 mmol/L is considered diagnostic). A random BGL of 11.1 mmol/L or above in the presence of typical diabetes symptoms is also considered diagnostic of type 2 diabetes in pregnancy.3
If atypical features are present, such as low body weight, weight loss at diagnosis or a family history of young-onset diabetes (less than 25 years of age at diagnosis) with an autosomal dominant pattern of inheritance, then alternative diagnoses such as type 1 diabetes, secondary diabetes (related to exocrine pancreatic disease or other endocrine causes such as cortisol or growth hormone excess) or monogenic diabetes (maturity onset diabetes of the young [MODY]) should be considered. Genetic testing for MODY and detailed diabetes-related autoimmune testing should be offered if there is a high clinical suspicion.4 The increasing prevalence of overweight and obesity in type 1 diabetes can make the differentiation from type 2 diabetes more challenging, and testing for type 1 diabetes should be carried out if there is a clinical suspicion regardless of weight.5
Outcomes in pregnancy
Maternal outcomes
Most guidelines for the management of pre-existing diabetes in pregnancy do not differentiate between type 2 diabetes and type 1 diabetes, although the pathophysiology of each is distinct. A retrospective case-control study looked at outcomes in women with type 1 diabetes compared with young-onset type 2 diabetes.6 The findings suggested poorer outcomes in neonates of mothers with type 1 diabetes, with a higher rate of pre-eclampsia, neonatal hypoglycaemia and neonatal intensive care admission. However, poor outcomes in type 2 diabetes occurred despite a lower HbA1c and shorter disease duration compared with type 1 diabetes, suggesting an additional detrimental effect of type 2 diabetes in addition to glycaemia. Compared with matched controls, mothers with type 2 diabetes had a higher rate of gestational hypertension, elective caesarean section, neonatal hypoglycaemia, preterm delivery and neonatal intensive care admission, and a lower live birth rate.6 The strongest predictors of adverse outcomes are poor glycaemic control, high body mass index (BMI) and pre-existing hypertension or nephropathy.7
Fetal outcomes
Risk of congenital malformation increases with consistently increased periconceptual HbA1c. A prospective cohort study of 274 type 2 diabetes pregnancies found the first HbA1c checked in the pregnancy was the only significant risk factor for congenital malformations, with an odds ratio of 1.45 per 1% increase in HbA1c.8 An emerging problem is previously unrecognised type 2 diabetes, which is diagnosed in early pregnancy, with rates of congenital abnormalities similar to that of pre-existing type 2 diabetes.9 Women with type 2 diabetes and comorbidities, such as hypertension or nephropathy, or with poor glycaemic control should deliver in a hospital that has availability for neonatal intensive care admission prior to 36 weeks.
Childhood outcomes
In utero exposure to hyperglycaemia increases childhood overweight, obesity and dysglycaemia, with both genetic predisposition and epigenetic modifications playing a role. There is a direct causal link between maternal diabetes and offspring adiposity, cardiometabolic health and diabetes independent of maternal BMI.10,11
Preconception counselling
Although uptake of preconception counselling is low, it is associated with a lower risk of congenital abnormalities in offspring. Both general advice and more detailed diabetes-specific advice should be provided (Box).12
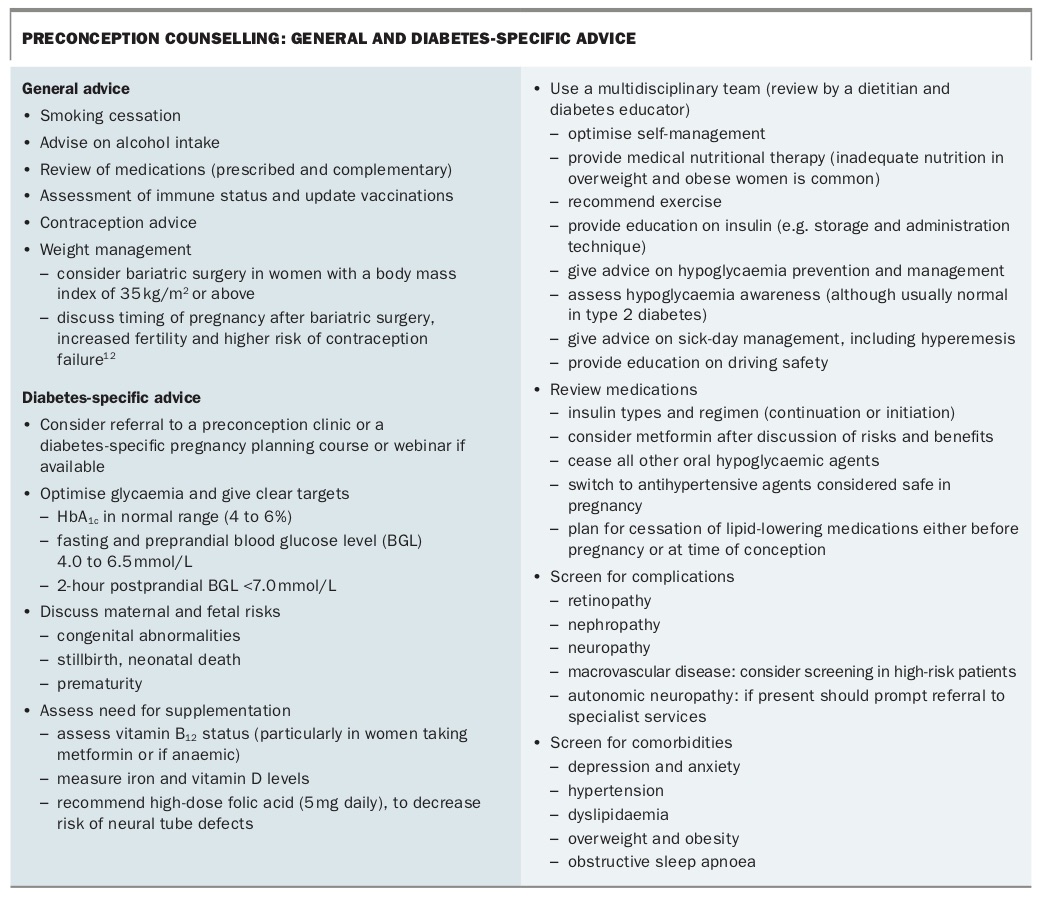{kind=link}
All women of reproductive age with type 2 diabetes should be given advice about appropriate contraception and pregnancy planning. This should be revisited regularly at clinic visits due to the risks of unplanned pregnancy. Discussion about contraceptive options early is imperative, particularly as lifestyle changes and weight loss can lead to regular ovulation in women who were previously anovulatory.
Overweight and obese women with type 2 diabetes should be encouraged to lose weight before pregnancy and be educated on structured diet and exercise programs. Bariatric surgery should be considered in women with a BMI of 35 kg/m2 or above who have not lost weight despite lifestyle interventions, although this needs to be individualised. Women of reproductive age represent the majority of those undergoing bariatric surgery. There have been no randomised controlled studies looking at pregnancy in women with type 2 diabetes after bariatric surgery. The recommended delay in pregnancy after surgery has been empirically set at 12 to 18 months to ensure the fetus is not exposed to rapid maternal weight loss and to decrease surgical complications during pregnancy. Women who have undergone bariatric surgery, particularly malabsorptive procedures, require monitoring for deficiencies of micronutrients and macronutrients and prompt replacement.13
Ideally, pregnancy should be planned for when glycaemia has been optimised. Inpatient management may be advised in women during very early pregnancy to rapidly improve glycaemia, as a swift transition to insulin with rapid and intensive dose titration is often needed. Metformin is often continued in pregnancy, whereas other oral hypoglycaemic agents are generally ceased. Immediate cessation of oral agents must be balanced against the risk of resultant hyperglycaemia and its adverse effects during organogenesis.
Screening for diabetes complications, as well as associated comorbid conditions such as obesity, hypertension and depression, should ideally take place before conception (see below for further details).14 Lipid-lowering agents, ACE inhibitors and angiotensin II receptor blockers should be ceased either before pregnancy or at time of conception. Antihypertensive agents that are considered safe in pregnancy include labetalol, methyldopa and nifedipine.
The reality is that only a small proportion of women plan pregnancy. In patients who present in early pregnancy, without formal preconception care, the same principles are applied. In a significant number of women (who are often asymptomatic) type 2 diabetes is not diagnosed until after pregnancy is confirmed. Strategies are therefore needed to improve screening and diagnosis of type 2 diabetes in young women to allow for optimal maternal and neonatal outcomes.
Management in pregnancy
Screening for complications
Screening for diabetes complications, particularly retinopathy and nephropathy, early in pregnancy is essential. Retinopathy can develop in pregnancy for the first time and can progress rapidly. Eye reviews should be performed at least three monthly (unless otherwise advised by the treating ophthalmologist) if baseline retinopathy is present, if there is a rapid improvement in glycaemic control, or if there has been a long duration of pre-existing diabetes.15
Diabetic nephropathy is less common in women with type 2 diabetes compared with type 1 diabetes in pregnancy. If the urine albumin to creatinine ratio is elevated, the woman requires close monitoring for detection of pre-eclampsia. During pregnancy, proteinuria can progress to the nephrotic range, and in women with pre-existing renal impairment, nephropathy can progress irreversibly in pregnancy and accelerate the need for renal replacement therapy.16 This is not predictable, but the risk is higher in women with elevated baseline creatinine levels and requires close monitoring.
The risk of pre-eclampsia is high in pregnant women with type 2 diabetes and blood pressure should be closely controlled.16 At each antenatal visit, every two to four weeks, blood pressure should be checked with use of the appropriate sized cuff. Urine dipstick testing for proteinuria should also be performed and quantified if appropriate. Symptoms of autonomic neuropathy including gastroparesis, postural hypotension and hypoglycaemia unawareness should be looked for.
Screening for macrovascular complications, including consideration of underlying ischaemic heart disease, should be performed, if not completed preconception. If there is clinical concern, a baseline electrocardiogram and transthoracic echocardiogram or stress echocardiogram should be considered. Risk of venous thromboembolism should be considered in obese women.
Screening for mood disorders is important as there is a strong association between diabetes and depression.17 The GP plays a pivotal role in this, having a therapeutic relationship with the patient before pregnancy, during and after. Early follow up with social workers and/or psychologists is important.
Review of medications and devices
Insulin
A basal-bolus insulin regimen (rapid-acting insulin at each meal and long-acting insulin at bedtime and/or breakfast) is usually required for optimal glycaemic control during pregnancy. The basal insulin often needs to be divided into two injections, especially if using larger doses. However, a single bedtime dose of basal insulin is occasionally sufficient. Premixed insulin (e.g. 30%/70% preparation of short- and long-acting insulin taken before breakfast and the evening meal) may also be effective for some women.
Home blood glucose monitoring is important and should be performed fasting, before meals and one to two hours postprandially. Target BGLs are fasting/preprandially 4.0 to 5.5 mmol/L, one-hour postprandially less than 7.8 mmol/L or two-hour postprandially less than 6.7 mmol/L.3 A glucose meter should be provided that has demonstrated accuracy in pregnancy (e.g. Accu-Chek Active, Freestyle Lite and Accu-Chek Performa meters).18 HbA1c declines in pregnancy due to the relative haemodilution and anaemia. It should be monitored at least once per trimester, with a target in the normal range (4 to 6% or 20 to 42 mmol/mol without hypoglycaemia) or less than 1% above normal (<7% or 53 mmol/mol).
Insulin pharmacokinetics appear to differ in pregnancy, although this has not been shown in all studies.19 The short-acting insulins have longer onset to peak concentration with slower absorption of insulin as pregnancy progresses, particularly with the breakfast meal in which many women are most resistant. To achieve optimal postprandial BGLs, administration of bolus insulin 20 to 30 minutes before eating may be needed in the second half of pregnancy.20 This also helps reduce delayed postprandial hypoglycaemia, which is common in these women who have an absent first-phase insulin response and exaggerated second-phase insulin response. In this setting, the peak endogenous insulin concentration lags the peak glucose concentration, leading to an elevated one- to two-hour postmeal BGL, followed by a later decline in the BGL.21 This can also be reduced by eating lower carbohydrate meals with a lower glycaemic index and proportionally higher fat and protein content delaying glucose absorption, and by ensuring carbohydrates are spread throughout the day with snacks between meals.
Daily insulin requirements generally increase two- to threefold over the course of pregnancy, so frequent clinical reviews are needed. If there is a sudden unexplained reduction in insulin requirement of more than 10% in the third trimester, the woman should present for obstetric review of fetal wellbeing, as this change may be associated with placental insufficiency. However, reduced insulin needs in isolation are not an indication for delivery.15 All women should be encouraged to monitor fetal movements and to present if these decrease.
Metformin
Metformin use in pregnancy is widespread but remains a topic of some contention, with variable use in different countries. Results from the Metformin in Women with Type 2 Diabetes in Pregnancy Trial (MiTy) are eagerly awaited.22
All women should be provided with a summary of the safety data for metformin in pregnancy, with a balanced discussion of risk and benefit, including the lack of long-term studies of possible effects of exposure to metformin on the fetus. In women with longstanding type 2 diabetes and marked insulin resistance, metformin can help decrease the total daily insulin dose and improve glycaemia. Metformin may also decrease treatment cost in some women, who may require over 400 units of insulin per day. In women who have milder insulin resistance and who wish to avoid insulin, metformin alone may be sufficient to maintain satisfactory glycaemia. The possible risks of the medication must be balanced with the risk of poor glycaemic control in these women.23
Sulfonylureas
Use of sulfonylureas in women during pregnancy is rare in Australia, and the Australasian Diabetes in Pregnancy Society consensus guidelines advise against this, due to a lack of safety data.15 However, in some countries, particularly in the US, glibenclamide is often used in pregnant women due to its low cost and oral route of administration.
Other non-insulin agents
Dipeptidyl peptidase-4 inhibitors, sodium-glucose cotransporter-2 inhibitors, thiazolidinediones, acarbose and glucagon-like peptide-1 agonists should be discontinued, as there is a lack of safety data for the use of these medications in pregnancy.
Aspirin
Low-dose aspirin has been shown to reduce the risk of preterm pre-eclampsia (before 34 weeks’ gestation) by up to 70% if initiated at 16 weeks’ gestation or before.24 There is no conclusive benefit of aspirin preventing pre-eclampsia after 34 weeks’ gestation. Women with type 2 diabetes have a 3.5 times higher risk of pre-eclampsia than women without diabetes,25 although the benefit of aspirin in women with pre-existing diabetes has not been specifically evaluated in randomised controlled trials.25 It is reasonable to recommend 150 mg aspirin at night to women with type 2 diabetes, starting before 16 weeks’ gestation, particularly if there are additional risk factors for pre-eclampsia.
Calcium supplementation
The incidence of pre-eclampsia is higher in regions with low calcium intake. Many studies have investigated the role of calcium supplementation (>1 g daily) in decreasing the risk of pre-eclampsia, possibly by decreasing vasoconstriction from parathyroid hormone or renin release, or by directly decreasing uterine smooth muscle contractility.26 The benefit of calcium has not been seen in some larger studies, although this may relate to these studies being carried out in populations with adequate dietary calcium intake. Overall, benefits seem to be greater in women with low calcium levels or at high risk of pre-eclampsia.
A 2014 national nutrition survey showed 90% of women do not meet recommended dietary intake of calcium.26 Further studies are required, but calcium is not associated with harm and it is reasonable to offer calcium supplementation for prevention of pre-eclampsia in women with type 2 diabetes in pregnancy as they are at higher risk of developing pre-eclampsia.
Folic acid supplementation
Women with type 2 diabetes have a higher risk of neural tube defects in offspring. High-dose folic acid (5 mg daily) is recommended from three months before conception until the end of the first trimester, then continuation of 0.4 to 1.0 mg daily until cessation of breastfeeding. Studies of low-dose folic acid supplementation in the general population show an 85% decreased risk of neural tube defects; however, no studies have looked directly into risk reduction in women with type 2 diabetes.27
Continuous glucose monitoring systems
The uptake of continuous glucose monitoring (CGM) systems is much higher in people with type 1 diabetes, but increasingly women with type 2 diabetes are interested in using technology to assist with improving glycaemia. The most common CGM systems in Australia are the Medtronic and Dexcom systems, which use a sensor electrode inserted into subcutaneous tissue, which measures interstitial glucose levels, with accuracy in pregnancy similar to outside of pregnancy.28 This is used together with capillary glucose readings. Use of CGM systems is subsidised by the National Diabetes Supply Scheme for women with type 1 diabetes, but not for women with type 2 diabetes.
Flash glucose monitoring systems measure interstitial glucose levels, which can be viewed via a sensor or mobile telephone interface. Although there are minimal data for use in pregnancy and they are not currently funded for use in pregnancy in Australia, women are increasingly choosing to use these systems in pregnancy. They are cheaper than the Medtronic and Dexcom systems and many women find them more convenient to use compared with other forms of CGM.
Multidisciplinary team review
Diabetes educator
Review by a diabetes educator before and during pregnancy is imperative. Discussion should include lifestyle and exercise recommendations, dietary intervention, insulin education, self-management, and safety around driving and hypoglycaemia management. Other important issues include insulin storage, injection technique, appropriate needle length (4 to 6 mm) and avoidance of lipodystrophy by rotation of injection sites.
Dietitian
Medical nutrition therapy should be provided to all women with type 2 diabetes, and an individualised nutrition plan made, with follow up and support. This should take into account pregnancy-specific nutritional needs, comorbidities, goals for gestational weight gain, the woman’s cultural background, financial impact and health literacy. Studies have shown clear benefit of medical nutrition therapy as part of the overall management of women with type 2 diabetes during pregnancy in decreasing maternal hospitalisation, neonatal death and neonatal intensive care admission.29
Peripartum and immediate postpartum diabetes management
In the late third trimester, a clear plan should be made regarding timing and dosing of insulin the day before induction of labour or planned caesarean, as well as a plan for a spontaneous unplanned labour. Women with type 2 diabetes having an elective caesarean should ideally be scheduled first on the list in the morning to minimise duration of fasting and simplify diabetes management.
Antenatal expression of breast milk may be considered, in the absence of contraindications such as placenta praevia and breech presentation. This may enhance the supply of colostrum for treatment of mild neonatal hypoglycaemia, decreasing need for neonatal intensive care admission and separation of mother and neonate. It may also increase the likelihood of successful initiation of breastfeeding, which is an important goal in the immediate postdelivery period. Safety of this practice has been established in low-risk women with gestational diabetes;30 however, specific evidence of efficacy is lacking in women with type 2 diabetes, particularly those with comorbid diseases or microvascular or macrovascular complications, therefore, it should be avoided in these high-risk groups.
Antenatal corticosteroids are often required in women who are likely to deliver early, to decrease complications of prematurity. The usual regimen is two doses of betamethasone 11.4 mg intramuscularly 24 hours apart.31 This invariably leads to hyperglycaemia; therefore, significant changes in insulin requirements are often required following betamethasone administration. Ideally, these women should be admitted for 48 hours for monitoring of BGLs. Glucose targets are not well defined, but maintenance of near normoglycaemia is important to reduce the risk of neonatal hypoglycaemia and acidosis.
In the presence of optimal glycaemic control, minimal or no insulin dose changes are required before active labour. Short-acting insulin is withheld during periods of fasting. Dose reductions of 10 to 20% of insulin glargine are often advised due to its long duration of action and resultant risk of postpartum hypoglycaemia. Isophane insulin usually does not require dose reductions. Metformin is discontinued at onset of spontaneous or induced labour. Tight glycaemic control during labour is imperative to decrease the risk of neonatal hypoglycaemia with BGL targets of 4.0 to 6.7 mmol/L. Many women with type 2 diabetes maintain this level of glycaemia without additional insulin treatment, but an extra small bolus dose of subcutaneous insulin or intravenous insulin and dextrose infusions may be required. Dextrose containing induction fluids during periods of fasting are important for minimising ketosis, which can develop rapidly during starvation and/or insufficient carbohydrate intake in pregnancy.
Insulin can be discontinued in the immediate postpartum period with monitoring of BGLs and a relaxed BGL target range of 5.0 to 10.0 mmol/L. This is justified due to a time of increased insulin sensitivity, decreased oral intake, sleep deprivation and initiation of breastfeeding, which increase the risk of severe hypoglycaemia.
If BGLs are persistently above target, insulin can be reintroduced judiciously. The insulin requirement is lower than pre-conceptually, but caution is needed because in some women there is an initial persistence of insulin resistance in the immediate postpartum period followed by a delayed improvement in insulin sensitivity and subsequent risk of hypoglycaemia. This risk can be exacerbated by lactation. Education on safety and prevention of hypoglycaemia during lactation, bathing the baby and driving is important. BGLs before these activities should be above 5 mmol/L; if it is in the lower end of the range, the woman should be advised to have a carbohydrate-containing snack.
Blood pressure should be monitored in the peripartum and postpartum period, due to the higher risk of pre-eclampsia. There should be a discussion about contraception before discharge. Metformin may be used during breastfeeding, but other non-insulin agents should be avoided. In women who do not breastfeed, caution is still needed with use of oral hypoglycaemic agents, particularly the sodium-glucose cotransporter-2 inhibitors, due to the risk of genital mycotic infections and euglycaemic diabetic ketoacidosis in the early postpartum period.
Neonatal management is not discussed in this article but careful consideration is needed regarding the most appropriate place for delivery. This is because access to neonatal intensive care facilities is important in cases of preterm delivery, if there has been poor control of diabetes or if comorbidities, such as hypertension or nephropathy, are present.
Conclusion
The prevalence of type 2 diabetes in young women is rising and, consequently, type 2 diabetes in pregnancy, with clear associations with poor maternal, neonatal and childhood outcomes. Preconception counselling is important, with optimisation of glycaemic control, as often consultation with the specialist team is in the late first trimester. Management of women with type 2 diabetes in pregnancy needs to be individualised where possible, using a multidisciplinary approach and with consideration for social and cultural factors. MT