Keratinocyte skin cancers: diagnosis and current management

Keratinocyte cancers, formerly known as nonmelanoma skin cancers, are an important cause of morbidity and mortality in Australia. In 2019, Cancer Council Australia published updated guidelines on diagnosis and management of keratinocyte cancers. This summary for GPs incorporates the latest update.
- Australia has one of the highest rates of skin cancer in the world, with keratinocyte cancer (formerly termed ‘nonmelanoma skin cancer’) the most common type.
- GPs play a crucial role in the detection and early management of keratinocyte cancers.
- Cutaneous squamous cell carcinoma (SCC) can metastasise; for patients with SCC unsuitable for surgery, treatment options include radiation therapy, chemoradiation, epidermal growth factor receptor (EGFR) inhibitors and immunotherapy.
- Basal cell carcinoma (BCC) is the most common keratinocyte cancer in Australia; hedgehog pathway inhibitors are a recent treatment option for patients with advanced metastatic BCC.
- Patients with keratinocyte cancers with poor prognostic features or locoregional spread should be referred to a specialist multidisciplinary team for planning and management.
Australia has one of the highest rates of skin cancer in the world, with keratinocyte cancers being the most common type. Keratinocyte cancers, formerly known as nonmelanoma skin cancers, comprise basal cell carcinoma (BCC) and cutaneous squamous cell carcinoma (SCC). Actinic keratosis is a precancerous lesion that can develop into SCC. Keratinocyte cancers cause about 560 deaths annually in Australia and accounted for over 939,000 treatments in 2015 alone.1,2 Furthermore, keratinocyte cancers are responsible for a disproportionately high financial cost to the healthcare system, representing 8% of healthcare spending on cancer in 2008-09 and over $700 million in reimbursements for diagnosis, investigations and treatment annually.1,2
GPs have an important role in the prevention, early detection and management of keratinocyte cancers in Australia. Skin consultations account for 14.8% of GP consultations, and skin cancers are the second most common reason for specialist referral.3 GPs are also well positioned to educate patients on the importance of sun-safe behaviours and to detect skin cancers at the earliest opportunity through full skin checks and opportunistic skin screening.
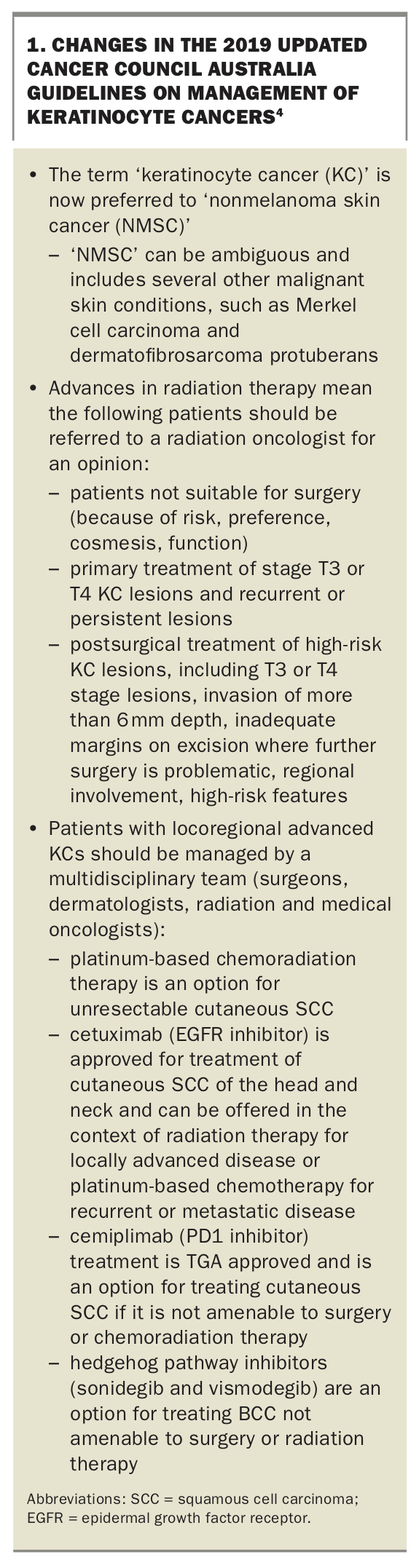
In 2019, Cancer Council Australia published updated guidelines on the diagnosis and management of keratinocyte cancers in the form of a ‘living guideline’.4 This update was a response to significant changes in treatment over the past decade, particularly radiotherapy and immunotherapy of advanced keratinocyte cancers. These changes led the Australian Government Department of Health to commission the Keratinocyte Cancer Guidelines Working Party to revise the 2008 guidelines on diagnosis and management of BCC and SCC.5
Here, we summarise the presentation, diagnosis and latest updated treatment and referral recommendations for keratinocyte cancers as per the updated 2019 guidelines.4 Key changes in the updated guidelines are summarised in Box 1. The important role of GPs in educating patients about sun-safe behaviour to help prevent keratinocyte cancers is discussed elsewhere.6
{kind=link}
Actinic keratosis
Actinic keratoses, also known as solar keratoses, are precancerous lesions commonly found on sun-exposed areas such as the face, scalp, ears and back of the hands (Figures 1a and b). They progress to SCC at the rate of 0.075% to 0.1% per lesion per year, sometimes extrapolated to up to 10% over 10 years.7
{kind=link}
Associated factors
Actinic keratoses are clinically significant not only because they may progress to SCC but also because the presence of multiple actinic keratoses indicates significant ultraviolet (UV) light exposure. It is recommended that patients with multiple actinic keratoses have full skin checks on a regular basis with their GP, who may arrange referral to a specialist dermatologist if appropriate.
Presentation and diagnosis
Actinic keratoses have varied clinical presentations. They are classically described as gritty macules, papules or plaques on an erythematous base, often with rough yellow or white scale. They can also present as hyperkeratotic, pigmented or atrophic lesions. The lesions are typically asymptomatic but may sting or itch.
The diagnosis of actinic keratosis is predominantly clinical. Biopsy should be considered if there is concern that the lesion may be an early SCC. Hallmark signs raising concern include tenderness, bleeding, inflammation and growth in height or thickness.
On biopsy, the distinction between an actinic keratosis and SCC is the extent of keratinocyte atypia:
- in actinic keratosis, keratinocyte atypia is confined to the lower portion of the epidermis
- in SCC, keratinocyte atypia occupies the entire epidermis and may infiltrate deeper into the dermis.
Treatment of actinic keratosis
Localised treatment
The first-line modality for localised treatment of actinic keratosis is liquid nitrogen cryotherapy. This usually causes a blister that heals over seven to 10 days. The duration of therapy varies depending on lesion size and location, but a freeze of about three to five seconds is recommended.
Curettage, electrodessication and shave treatments can also be considered as treatment for actinic keratosis. However, these treatments are often reserved for larger, thicker lesions.
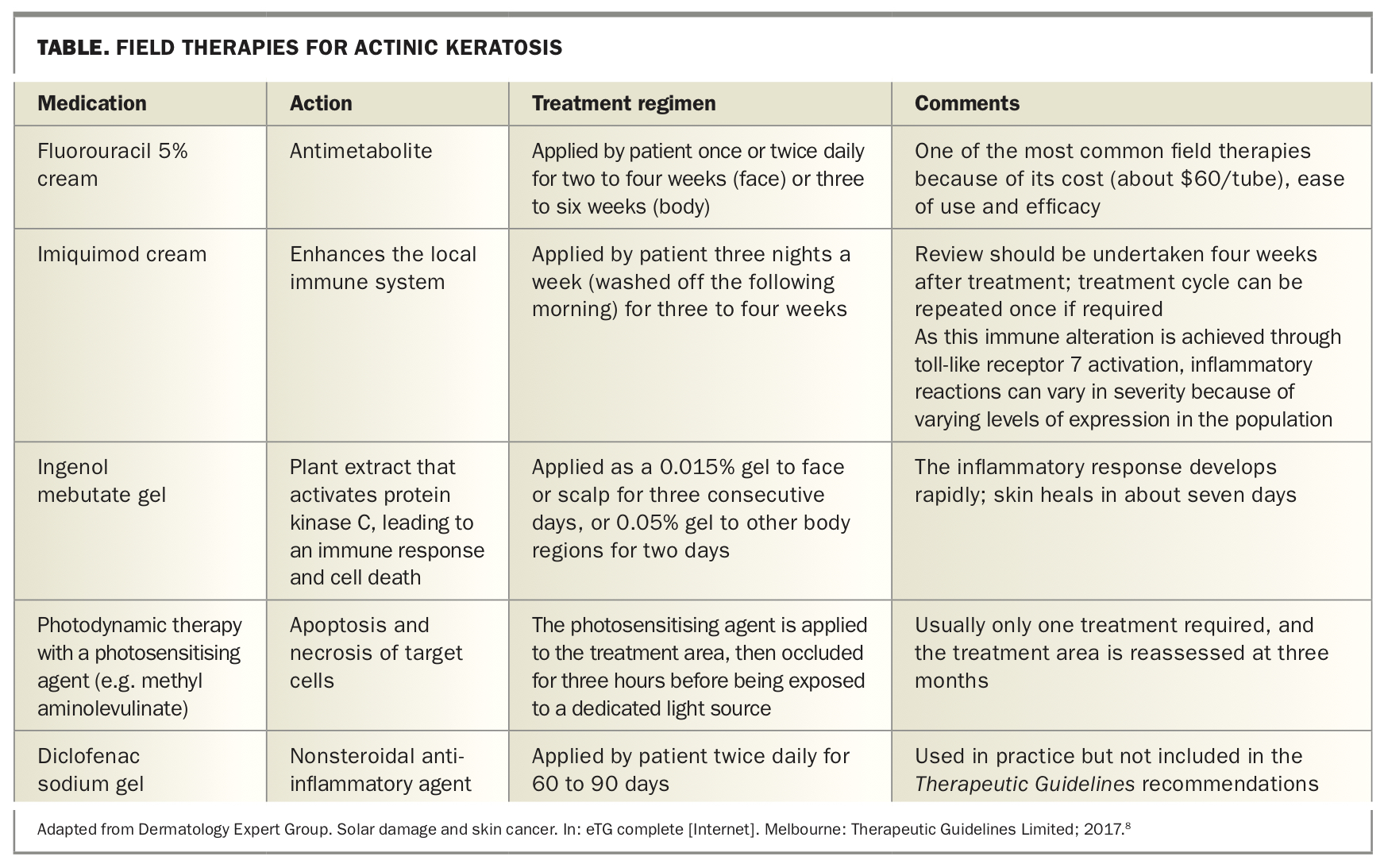
Field therapy
Field therapies should be considered for areas that contain multiple actinic keratoses. Field therapies include:8
- fluorouracil 5% cream
- imiquimod cream
- ingenol mebutate gel
- photodynamic therapy, involving application of a photosensitising chemical to the lesion, followed by irradiation with an appropriate light source (Table).
{kind=link}
Patient education about these therapies is paramount, as they act by inducing an inflammatory reaction, including redness, soreness and crusting. Patients are best counselled about this before therapy, including being shown pictures of expected reactions.
Squamous cell carcinoma
The second most common skin cancer in Australia is cutaneous SCC (Figures 2a and b). The age-standardised incidence rate of cutaneous SCC is about 387 per 100,000 in people aged 14 years and over.9 The incidence increases steeply with age from mid-adulthood and appears higher in men than in women across all age groups.
{kind=link}
The most common sites of cutaneous SCC are the head and neck areas in men, and the upper limbs followed by the head and neck areas in women. After accounting for body surface area, the highest incidence of cutaneous SCC in both men and women is on the face, particularly the lips, ears, nose, cheek and eyelids.
Associated factors
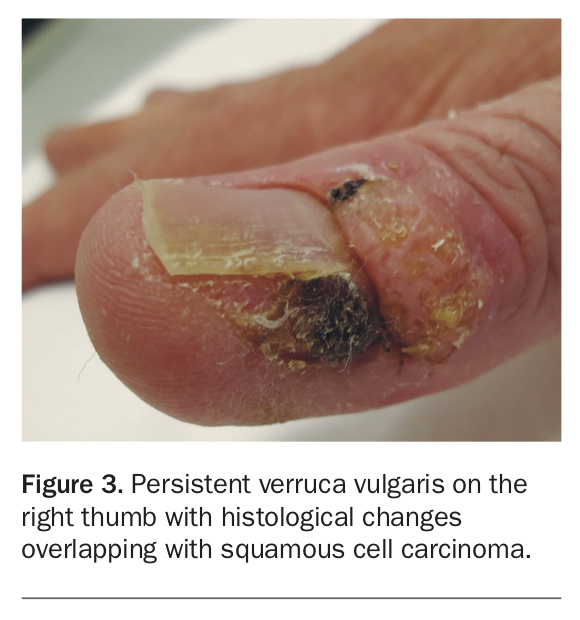
Cutaneous SCC can arise de novo with no risk factors or triggers. However, cutaneous SCC may also develop from actinic keratosis or be associated with the use of immunosuppressive medications, infection (e.g. by oncogenic subtypes of human papillomavirus), chronic inflammation or previous trauma (Figure 3). The two main risk factors for SCC are:
{kind=link}
- cumulative UV exposure, which damages the DNA of keratinocytes and impairs the immune system
- lighter Fitzpatrick skin type, which increases susceptibility to the effects of UV exposure.
The primary concern with SCC is its ability to metastasise, with metastatic SCC accounting for about 20% of skin cancer deaths. A large nationwide study in England found the incidence of metastatic SCC in people with primary cutaneous SCC to be 1.1% in women and 2.5% in men over 36 months.10
Presentation and diagnosis
Cutaneous SCC has a spectrum of presentations. In-situ SCC is termed Bowen’s disease and presents typically as an erythematous patch or plaque with scale and, in rare cases, pigmentation. On histopathological examination, Bowen’s disease shows keratinocyte atypia involving the full thickness of the epidermis. Without treatment, 2 to 5% of cases of Bowen’s disease progress to involve the dermis, defined as invasive SCC.7 SCC presents as an erythematous keratotic papule or nodule, which may be tender on palpation.
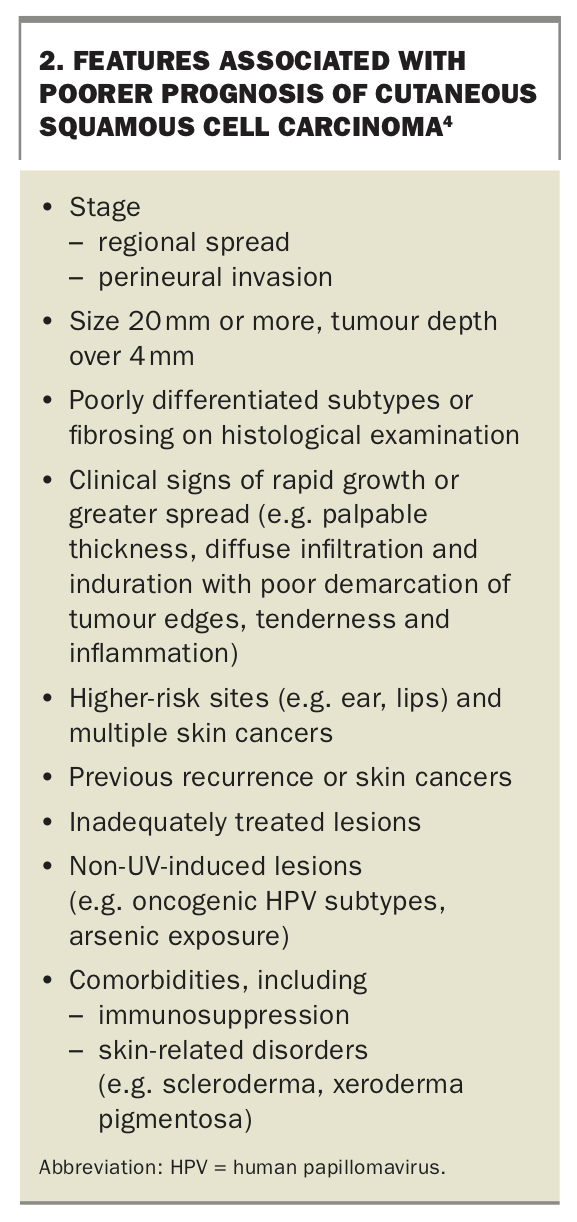
Diagnosis of Bowen’s disease and SCC is via biopsy. If invasive cutaneous SCC is suspected, the biopsy should be deep enough to determine the extent of dermal involvement. Regional lymph nodes should be examined, and suspected metastases should be confirmed with fine needle aspiration. Key factors that indicate a poor prognosis for SCC include regional spread, perineural invasion, poorly differentiated histological appearance, higher-risk sites and comorbidities such as immunosuppression (Box 2).4
{kind=link}
Treatment of SCCs
Surgery
Surgical treatment options for cutaneous SCC include local excision and Mohs micrographic surgery. Low-risk lesions can be treated with surgical excision, curettage and electrodesiccation, or punch excision. Larger lesions up to 20 mm can be removed using a scalpel, ensuring adequate lateral and deep margins. Adequate deep margins are particularly important, as inadequate deep margins significantly increase the risk of recurrence. Fear of damaging underlying anatomy and inexperience may lead to incomplete deep margins in otherwise easily resectable tumours. The orientation of the excision is important; tumours should be excised along relaxed skin tension lines, but in a line that avoids distortion.
For patients with lesions with poor prognostic features, such as size 20 mm or more, or poor differentiation (Box 2), referral to a multidisciplinary team or to a specialist for assessment and treatment should be considered.4 Mohs micrographic surgery is a surgical option for cases where tissue preservation and cosmesis is of paramount importance. The technique involves histopathological examination of frozen sections of almost the entire peripheral and deep margins of the excised tissue, in contrast with standard sectioning, where 0.1 to 1% of the surgical margin is examined.
Surgical treatment of advanced cutaneous SCC with nodal involvement involves lymphadenectomy for disease in the axilla or groin, or selective neck dissection for cervical lymph node involvement. Dermal lymphatic spread (in-transit metastasis) should be managed by wide surgical excision followed by adjuvant radiotherapy.
Radiation therapy
Radiation therapy for SCC has improved significantly in the past few decades. Modified fractionation schedules and more precise fractionation techniques allow an improved balance between killing tumour cells and minimising effects on normal tissue.
There are several indications for radiotherapy of cutaneous SCC. First, it is a therapeutic option when surgery is not feasible because of patient frailty, comorbidities or high surgical or bleeding risk, or when surgery will have a significant effect on cosmesis or functional outcome. Secondly, referral to a radiation oncologist for multidisciplinary care should be considered for patients with T3 or T4 stage primary tumours or persistent or recurrent cutaneous SCC.
Referral for a radiation oncologist opinion about postoperative radiation therapy should also be considered for patients who have had complete excision of high-risk cutaneous SCC, such as T3 or T4 stage tumours, and those with more than 6 mm depth of invasion, inadequate margins on excision when further surgery is problematic, regional involvement or other poor prognostic features (Box 2).
Systemic treatment
Locoregional advanced cutaneous SCC represents an advanced stage of disease that may present de novo or after previous surgery and radiation therapy. The goal of treatment is to clear local disease and prevent further recurrence or regional metastasis. However, options may be limited by the location of the primary tumour and patient comorbidities and whether they are amenable to surgery or radiation therapy. Patients should be assessed on a case-by-case basis in a multidisciplinary setting.
For patients with resectable disease, surgery followed by adjuvant radiation therapy is the preferred treatment. For patients with unresectable disease, platinum-based chemoradiation may be considered.
Cetuximab, an epidermal growth factor receptor (EGFR) inhibitor, is approved for treatment of SCC of the head and neck. It can be used in combination with radiation therapy for locally advanced disease, or in combination with platinum-based chemotherapy for recurrent or metastatic disease.
For patients unsuitable for surgery or radiation therapy, treatment with cemiplimab (a PD-1 inhibitor) may be an option. Cemiplimab has TGA approval in Australia for adults with metastatic or locally advanced cutaneous SCC who are not candidates for curative surgery or radiation therapy.
Basal cell carcinoma
BCC has the highest incidence of all cancers in Australia. The estimated age-standardised annual incidence rate of BCC is 884 per 100,000 overall, and is higher in men than in women (1041 versus 745 per 100,000). The incidence of BCC increases with age, although not linearly. It is higher in men compared with women up to age 50 years but similar at older ages. In both sexes, 50% of BCCs are found on the head and neck, 25% on the trunk and about 10% on each of the upper and lower limbs.9
Associated factors
As with SCC, UV radiation is the greatest risk factor for BCC, but unlike SCC, risk is associated with intense episodes of burning rather than cumulative exposure. BCCs rarely metastasise, and the main clinical concern is local destruction. BCC features associated with a poorer prognosis are listed in Box 3.
{kind=link}
Presentation and diagnosis
The most common BCC presentation is the nodular form, appearing as pearly papules or nodules with evident telangiectasia or umbilication. BCCs may ulcerate and are often found in the head and neck regions, even in areas of little sun exposure such as the inner canthus. Superficial BCCs present as erythematous patches or plaques, often on the trunk or extremities (Figure 4).
{kind=link}
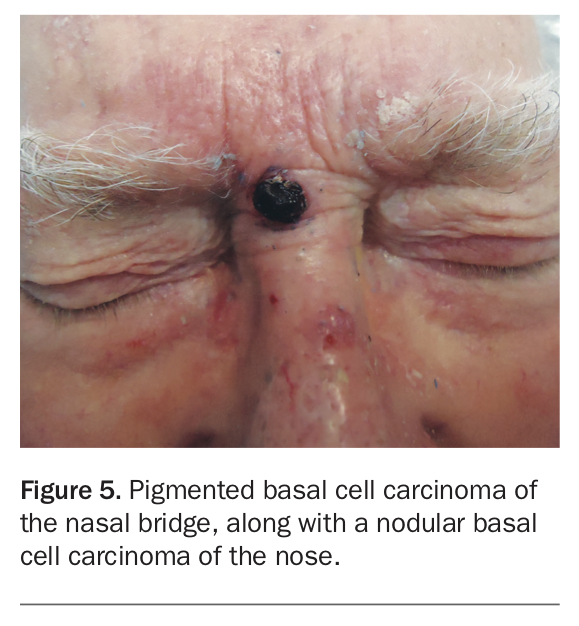
BCCs can also be pigmented, leading to a clinical differential diagnosis of melanoma, but an evident pearly edge and vascularity seen macroscopically or through a dermatoscope can aid in the distinction (Figure 5). Less common BCC variants include sclerosing (morphoeic or scar-like), micronodular and basosquamous BCCs.
{kind=link}
BCCs are often diagnosed by biopsy. The BCC site and histological subtype dictate treatment.
Treatment of BCCs
Topical therapies
Superficial BCCs may be treated with topical therapies, including curettage and electrodesiccation, cryotherapy, imiquimod cream and photodynamic therapy. Cryotherapy is performed with a double freeze-thaw cycle of 20 to 30 seconds. This causes a significant blister that heals in about three to four weeks. It can lead to hypopigmentation, so it is important to counsel patients about this.
Similarly, imiquimod treatment of BCCs is more intensive than for actinic keratoses, with therapy applied by the patient for five nights per week for six weeks. Imiquimod stimulates the immune system and causes local skin inflammation, destroying the lesion. The degree of inflammation is variable and depends partly on the type of skin lesion and genetic factors. If severe inflammation occurs, patients may need to take a break from therapy for a week or two to allow time for the reaction to settle before continuing treatment. There is usually a good cosmetic outcome with little scarring after imiquimod treatment.
Photodynamic therapy can be used for superficial and thin nodular BCCs. It usually requires two treatment sessions, one week apart, with lesions first descaled or debulked, and the sensitising agent applied at a thickness of 1 mm and a margin of 5 mm.
Surgical treatment options
Surgery is usually the first-line therapy for nonsuperficial BCCs such as nodular or nodulocystic BCCs. It often involves excision and direct closure. Options include electrodessication and curettage in anatomically favourable areas.
Micronodular, infiltrating and fibrosing (morphoeic) BCCs are less well defined and need surgical excision with wider margins. For patients with these types of BCC or lesions with poor prognostic features (Box 3), referral to a specialist is appropriate for consideration of options such as Mohs micrographic surgery, postsurgical adjuvant treatments in certain cases and close follow up. The rate of recurrence of this group of tumours is higher if histological margins are close or the BCC is incompletely excised.
Radiation therapy
Radiation therapy using curative doses is an alternative treatment for BCCs if the patient declines surgery or surgery is inappropriate because of patient factors such as frailty, tumour-related factors (e.g. where tissue conservation or cosmesis is a high priority, such as in BCC of the eyelid) or treatment-related factors (e.g. concurrent anticoagulant therapy).
For patients with a T3 or T4 stage primary BCC or persistent or recurrent BCC, referral to a radiation oncologist for an opinion regarding radiation therapy should be considered. Patients with postoperative BCCs with high-risk features may also be referred for an opinion from a radiation oncologist.
Persistent BCCs after a curative dose of radiation therapy should be treated in consultation with a radiation oncologist. Biopsy and salvage excision surgery are often required.
Systemic therapy
Metastatic BCC is rare. If suspected, confirmation is required via biopsy. Patients with complex locally advanced disease are best treated by a multidisciplinary team that includes surgeons, dermatologists, radiation oncologists and medical oncologists.
Locoregional metastases should be treated if possible with surgical excision or radiation therapy. When treatment with curative intent (surgery, radiation therapy or both) is not possible, oral therapy with a hedgehog pathway inhibitor such as sonidegib or vismodegib should be considered. Sonidegib and vismodegib appear to have similar efficacy and have similar side effects, including muscle spasms, hair loss, taste loss and cramps. In some cases, if side effects are not tolerated, intermittent dosing with a hedgehog inhibitor can be used.
When should a GP refer?
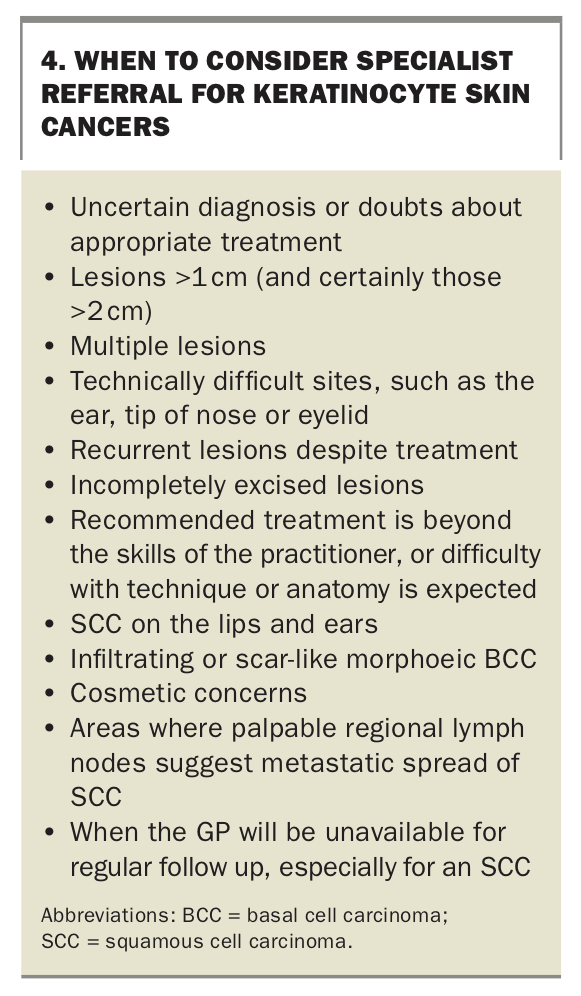
GPs are well positioned to educate patients on the importance of sun-safe behaviours, to detect skin cancers at the earliest opportunity and to provide initial management. Recommendations on when to consider referring patients for specialist care are shown in Box 4.
{kind=link}
Patients with suspicious lesions and those requiring surveillance or surgical management, including Mohs micrographic surgery, may be referred to a dermatologist. Referrals to plastic surgery and surgical oncology specialists are appropriate for lesions that require complex surgical management or have higher risk features. For patients who are unable to undergo surgery because of lesion features or comorbidities, referral for a radiation oncology opinion is appropriate. For complex tumours and metastatic tumours, referral to a multidisciplinary team that includes dermatologists, surgeons and medical and radiation oncologists is recommended for planning and management.
Conclusion
Keratinocyte cancers are the most common skin cancer encountered in Australia, and GPs play a crucial role in their detection and early management. Full-skin examination is recommended for patients at risk of skin cancers, as many areas of the skin cannot be adequately monitored by patients themselves. Prevention through sun-safe education, early detection and appropriate treatment can help reduce the impact these cancers have on patients’ lives and the healthcare system. MT