Non-operative treatment of appendicitis. Is this possible?

Appendicitis
Abdominal pain
A fit 30-year-old man with appendicitis is managed conservatively with intravenous antibiotics but develops a pelvic abscess and subsequently undergoes laparoscopic appendicectomy. What is the role of conservative treatment in acute appendicitis?
Case scenario
Harry, a fit and active 30-year-old man, presented to the emergency department with right lower abdominal pain, anorexia and loose stools. He had just returned from two years spent in the USA, where he had recently been managed conservatively for acute appendicitis.
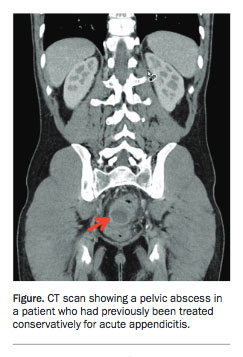
About six weeks before this presentation, Harry had been admitted to hospital with a five-day history of lower abdominal pain and anorexia. Based on the symptoms and ultrasound findings, he was given a provisional diagnosis of acute appendicitis. He was managed conservatively with intravenous antibiotics for one week and then discharged home on oral antibiotics. He re-presented three weeks later with ongoing lower abdominal pain requiring his readmission. Intravenous antibiotics were restarted and a subsequent computerised tomography (CT) scan revealed a pelvic abscess, which was treated by transgluteal percutaneous drainage. Harry’s symptoms settled and he was advised to undergo an interval (i.e. delayed) appendicectomy six weeks later.
Shortly afterwards, Harry returned to Australia, the symptoms recurred and he presented to the emergency department. A CT scan showed a residual pelvic abscess (Figure). He underwent laparoscopic appendicectomy where an acutely inflamed appendix was found complicated by perforation, associated with a free-lying faecolith. A moderately large right-sided pelvic abscess was completely aspirated and a drain left in situ. Postoperatively, Harry remained in hospital on intravenous antibiotics for four days before having the drain removed. He was then was discharged home well.
{kind=link}
Was this patient managed appropriately at the original presentation? Is an operation no longer the preferred option for managing patients with acute appendicitis? What is the role for an interval appendicectomy after conservative treatment of appendicitis? When is it appropriate to offer conservative management for acute appendicitis?
Commentary
Appendicitis is the most common surgical emergency presentation across all age groups. Although there are data to suggest that rates are decreasing in some countries, about 9% of people experience appendicitis in their lifetime and 14 to 20% of patients develop complicated appendicitis.1-3 In Australia alone, around 32,000 patients are admitted with appendicitis annually, and laparoscopic appendicectomy is the most common emergency operation performed.4
Diagnosis
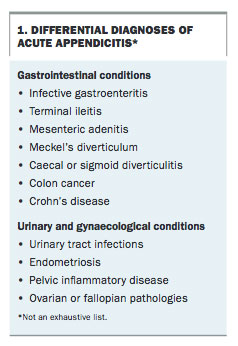
Generalised abdominal pain localising to the right lower quadrant and associated anorexia are cardinal symptoms of appendicitis. A thorough history and clinical examination, including assessing for the presence of urinary or gynaecological conditions, are important in excluding other diagnoses. Differential diagnoses are listed in Box 1.
{kind=link}
Biochemical inflammatory markers are used commonly as adjuncts in the diagnosis of appendicitis. However, these should be interpreted with caution because a normal white cell count or C-reactive protein (CRP) does not exclude early appendicitis. Urine dipstick and microscopy results are also helpful to exclude alternative diagnoses.
In most cases, appendicitis can be diagnosed clinically; however, in specific populations imaging is particularly helpful. For example, in older patients where
other pathologies are prevalent (e.g. newly diagnosed malignancy or right colon diverticulitis) abdominal CT scans may be indicated. Abdominal and pelvic ultrasound is used preferentially to avoid radiation exposure in children and in pregnant women. CT scanning provides a sensitive diagnostic tool and can reliably confirm or exclude appendicitis in most cases. Imaging may also be helpful in differentiating early appendicitis from complicated appendicitis, including cases of appendiceal phlegmon (diffuse inflammatory mass) and abscess formation.5,6
Surgical treatment
The first recorded appendicectomy was performed by Dr Claudius Amyand in 1735 at St George’s Hospital in the UK. The patient was an 11-year-old boy with a fistula in a long-standing right groin hernia. The operation was carried out successfully and without anaesthesia but diacodium (a herbal preparation made mainly from poppies [pre-modern medicine]) was used as a pain killer. The appendix was lying in the hernia sac and had ruptured secondary to a small pin that the boy must have swallowed previously.7 To this day, when the appendix is found within a hernia sac it is known as an Amyand’s hernia.
A surgical intervention has been the mainstay of treating appendicitis for more than a century. In 1886, Fitz described the relationship between appendicitis and pelvic abscesses, and in 1969, McBurney demonstrated that reduced morbidity from pelvic infections is attributable to having had an appendicectomy.8,9
Laparoscopic surgery
In recent decades, the transition from an open to a laparoscopic approach has resulted in shorter hospital stays and earlier returns to normal activity.10-12 Laparoscopic appendicectomy is a relatively safe procedure and most patients with uncomplicated appendicitis are discharged after an overnight stay.11,12 Laparoscopy also enables the surgeon to assess and treat, where necessary, other intra-abdominal pathology.
General perioperative risks include infection and anaesthesia-related complications. Postoperative pain and ileus may occur, particularly if there was significant local sepsis or if dissection of the appendix stump was difficult. Local complications such as bleeding or abscess formation should be suspected if these symptoms do not settle quickly. More serious adverse events such as small bowel perforation during insertion of the laparoscopic ports, and even mortality, are extremely rare but can occur.2
The role of non-operative management in acute appendicitis
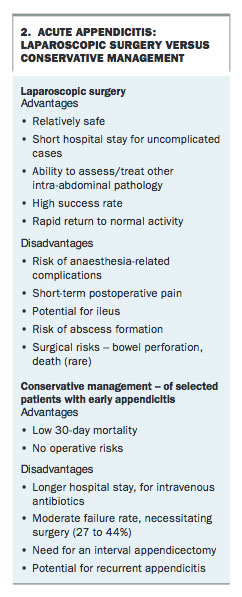
Recently, several randomised controlled trials (RCTs) and meta-analyses have challenged the exclusively surgical approach to the management of appendicitis (Box 2). These studies were undertaken to identify which patients, if any, might be treated conservatively to avoid the associated morbidity and potential complications of an appendicectomy. It appears that in specific patient groups, antibiotic therapy alone is safe and effective in managing uncomplicated appendicitis.2,13-19 Gram-negative and anaerobic organisms are mostly responsible and these can be treated with either single- agent (amoxicillin with clavulanic acid) or dual-agent therapy (a cephalosporin and metronidazole).
{kind=link}
The Appendicitis Acuta (APACC) study is the largest multicentre clinical trial comparing treatments of appendicitis.16 More than 500 patients with a CT diagnosis of uncomplicated appendicitis were randomised to treatment with antibiotics alone or laparoscopic appendicectomy with follow up for 12 months.16 Of patients given antibiotics alone, 73% were successfully treated without an operation. However, 27% failed medical therapy and required operative management during the follow-up period. Medically managed patients had comparatively longer hospital stays, but this may have been partly accounted for by the study protocol. There was a comparable 30-day mortality, which was 0.4% in both groups. No patients in the antibiotic therapy group developed life-threatening infections as a result of delaying appendicectomy.16
A recently published meta-analysis of five major studies comparing antibiotic and surgical treatment of acute appendicitis reported that on average 66% (41.1 to 78.5%) of patients were successfully treated with antibiotics alone, with no recurrence within one year, compared with 85 to 100% of the surgically managed group.17 Another meta-analysis including 1116 patients with nonperforated appendicitis reported fewer major complications (4.9% vs 8.4%) in patients treated with antibiotics alone.18 However 8.2% of 510 patients treated with antibiotic therapy went on to require an operation at a later date and 23% had a recurrence of appendicitis within the first year.18
Are all patients suitable for trial of non-operative management?
There is a wide range of presentations of appendicitis, from uncomplicated cases with or without a faecolith to perforated appendicitis with either a localised abscess or more widespread peritonitis. It is now accepted that some cases of uncomplicated appendicitis can resolve either spontaneously or with antibiotics alone. However, those patients who initially present with complicated appendicitis (i.e. localised peritonitis, an abscess, or the presence of a faecolith) usually follow a different clinical path that most often requires operative intervention.19 It is appropriate in the first instance for all patients with suspected appendicitis to be referred for an early surgical opinion.
Several predictors of successful medical therapy have been identified. RCT data have shown that patients who were successfully treated non-operatively had an average body temperature of 37.2°C compared with 37.5°C in patients who required operative management. Biochemically, a CRP level greater than 50 U/L and a neutrophil to lymphocyte ratio of 5.74 or greater have also been reported to be sensitive predictors of complicated appendicitis with low specificity.20,21 In terms of imaging there is evidence that patients with a faecolith evident on CT scan have a high chance of failing non-operative management, and of subsequently having or developing complicated appendicitis.22,23 As a result these patients were excluded in the APACC study.15 Although routine ultrasound or CT imaging are not necessary or recommended in patients who present with typical symptoms and signs of appendicitis, there may be an argument for greater use to select those most suitable for conservative treatment.
Although high-risk patients (e.g. older adults, immunocompromised patients and patients with medical comorbidities) could also potentially benefit the most from nonoperative treatment of appendicitis, they were excluded from all clinical trials.15,16 Therefore, the efficacy of the antibiotic-first approach in managing appendicitis in this group of patients remains unknown.
Interval appendicectomy
There is ongoing debate about whether after successful medical treatment of appendicitis, patients should proceed to an elective interval appendicectomy. It is surprising how often the appendix in these patients appears normal, with no signs of the previous inflammatory process. In contrast, in those patients with ongoing symptoms despite antibiotics and resolution of changes on imaging, or in those who have a radiologically diagnosed faecolith or previous episodes of appendicitis there is a good case for performing an interval appendicectomy.22-24
Finding a normal appendix at operation
A normal appendix is encountered in 10 to 28% of patients who undergo appendicectomy and is more commonly found in women than in men, as well as in younger adults.2,25,26 The negative appendicectomy rate may be reduced to less than 10% by judicious use of preoperative imaging.26 Although the appendix may look grossly normal at the time of the operation it is usually removed because submural inflammation is often found on subsequent histopathological examination. Furthermore, removal of a normal appendix is helpful to exclude a possible future diagnosis if symptoms recur. In this situation, it is important to search for other causes of the presenting symptoms (Box 1). It could be argued that routine non-operative treatment of all patients with uncomplicated appendicitis especially in females may reduce the rate of negative appendicectomy. However, to date this has not been demonstrated by clinical studies.
Complicated appendicitis: operative and non-operative management
Patients with perforated acute appendicitis presenting within 72 hours of the onset of symptoms should have an operation to avoid further complications. However, those with more than five days of symptoms before presentation, and when imaging confirms an appendiceal abscess or phlegmon have a high risk of complications with immediate operative intervention. They are best treated non-operatively in the first instance. This involves broad-spectrum intravenous antibiotics, bowel rest, rehydration and, if indicated, percutaneous drainage of any associated abscess. The decision not to operate can be difficult and depends on the patient having localised symptoms only and otherwise being well. A key feature of non-operative management in these patients is that they require close and frequent observation particularly early in the course of treatment. After discharge from hospital these patients also need regular review to ensure they remain symptom free. The most appropriate method and timing of repeat imaging during follow up in these patients is not clear.27
A delayed appendicectomy can be arranged six to eight weeks after the symptoms settle. It has been argued that this prevents recurrence and will also exclude a missed neoplasm.2,3,28 However, as indicated above the need for interval appendicectomy has been questioned by numerous studies.29,30
Conclusion
The surgical approach to the management of appendicitis is widely accepted and remains the gold standard of care. However, there are now good data that adults with image-proven uncomplicated appendicitis can be safely and effectively treated with antibiotic therapy alone albeit with close monitoring. This approach is particularly helpful in patients who are high-risk surgical candidates. Immediate benefits include not undergoing an operation with the potential for surgical complications, but this is at the risk of failed medical treatment and recurrence of symptoms.
Patients must be carefully selected for conservative treatment and specifically for prolonged antibiotic therapy so as to reduce the risk of delayed complications as well as potential antibiotic resistance. In the absence of routine imaging, objective confirmation of uncomplicated appendicitis can be difficult. Large multicentre trials are yet to be done to define clinical criteria for subgroups of patients who are likely to fail antibiotic therapy alone.
Perforated appendicitis causing peritonitis or appendicitis associated with a faecolith should always be treated surgically. However, it is reasonable to offer conservative treatment in selected patients with appendicitis as long as they are monitored carefully and on a regular basis. These patients need to be informed that this approach may not work and that they should seek urgent medical attention if their symptoms do not settle. MT
References
an updated meta-analysis of randomised controlled trials. World J Surg 2016; 40: 2305-2318.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.