Acute low back pain: avoiding the transition to chronic pain

Back pain
The hallmarks of new evidence-based approaches to assessing and treating acute low back pain are limited use of medical imaging, appropriate use of analgesia and an emphasis on patient education as a means to self-management. Risk stratification enables early identification and appropriate treatment of patients who are most likely to develop chronic pain.
Low back pain (LBP) is pain occurring between the gluteal crease and below the twelfth rib that may or may not be accompanied by features of lumbar radicular involvement. Based on the duration of the episode, patients can be classified as having acute (less than three months’ duration) or chronic (greater than three months’ duration) LBP. Acute LBP is common and has an excellent prognosis, with almost half of affected patients recovering within a few weeks; however, about 15% may have symptoms persisting beyond 12 months.
The most common form of LBP is nonspecific LBP. A diagnosis of nonspecific LBP is made when there are no signs of a serious underlying condition such as a vertebral compression fracture, infection or cancer, and no nerve root involvement is being considered.
This article focuses on the assessment and treatment of the more common primary care presentations of lumbar pain and will not discuss the assessment and treatment of acute LBP with radicular symptoms and chronic LBP. A comprehensive approach to the evidence-based assessment and treatment of all aspects of acute LBP is contained in the NSW Agency for Clinical Innovation model of care for acute LBP.1
The Global Burden of Disease Study has ranked LBP the sixth most burdensome condition globally when both death and disability are considered.2 However, in Australia it ranks second. During any one year, there is a 15 to 20% chance that an adult will experience an episode of back or neck pain. Commonly, episodes of acute LBP resolve within two to three weeks; however, when the pain persists beyond 12 weeks the associated disruption to health has significant personal, social and economic impacts.3 LBP is most prevalent among working-age adults, with profound economic consequences. In Australia each year, over $1 billion is spent on direct healthcare costs associated with LBP.4
Features of acute low back pain
Acute LBP is epidemiologically, psychosocially and therapeutically different from chronic LBP. Treatments for acute pain syndromes mostly do poorly or fail when applied to chronic LBP. The uncritical application of a biomedical model to assess and treat acute LBP has not always resulted in improved patient outcomes, but has led to an escalation in medical imaging, nonevidence-based pharmacotherapies, often inappropriate spinal injections, passive physical therapies and a proliferation of expensive practitioner-dependent niche therapies. The initial patient assessment must consider the possible presence of serious spinal pathology or ‘red flag’ conditions. Considering biopsychosocial aspects of the patient’s pain offers the potential for better patient outcomes for people with acute LBP.
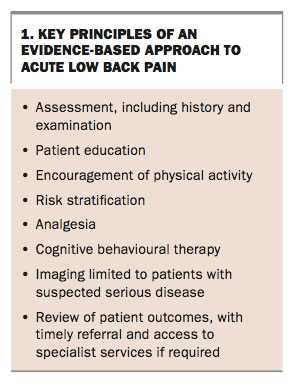
It is not possible, despite appropriate examination and investigations, to allocate a precise anatomical site for the pain source, nor to ascribe an underlying pathological process for a patient with nonspecific LBP. There is a segmental overlapping of sensory supply throughout the spine, making localisation of the pain based on somatic pain referral patterns problematic. As such, the triaging of patients into those with back pain alone and those with back and leg pain creates a more functional approach to organising clinical assessment and treatment. The key principles of an evidence-based approach to acute LBP are presented here and summarised in Box 1.
{kind=link}
Key principles of an evidence-based approach to LBP
Assessment
On initial presentation of a patient with acute LBP in primary care, thorough history-taking and an examination that includes a focused lower limb neurological examination are required. The history and initial clinical assessment are used together to identify patients in whom serious disease is suspected. Red flags assist in identifying these patients and the need for further diagnostic work-up (Box 2). Simplistic application of single red flags in isolation is not informative and should be avoided. A past history of malignancy in any patient and past or current corticosteroid therapy in an older person, which may suggest vertebral fracture, are the most common red flags among primary care patients.5
{kind=link}
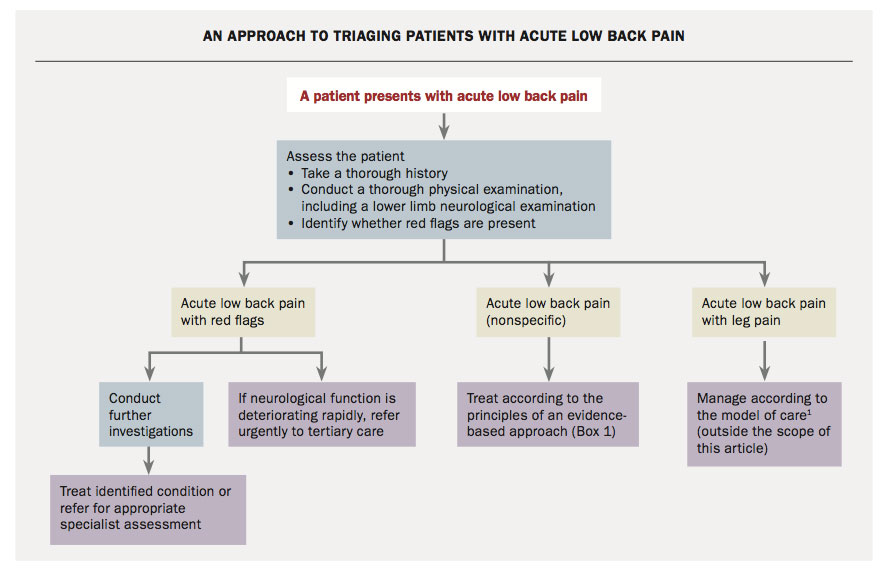
After the initial assessment, which should take into account that patients may have referred pain from other sources such as an aortic aneurysm, renal disease, retroperitoneal disease or organ disease within the pelvis, the GP is able to triage patients with acute LBP into three groups as follow, and as shown in the Flowchart:
{kind=link}
- patients with red flags who require further investigation, specialist assessment or, in the case of rapidly deteriorating neurological function, urgent referral to tertiary care
- patients who have acute LBP alone (nonspecific LBP)
- patients who have back and leg pain, with or without signs of lower limb neurological dysfunction. Patients in this group include those who have a disc herniation with nerve root compression (radiculopathy), spinal canal stenosis with radiculopathy and somatic nondermatomal referred pain from disc degeneration without evidence of radiculopathy.
Patient education
Patient education is the foundation of a self-management approach to acute LBP. This may include giving take-home information or using digital educational resources to inform patients about the overall good prognosis of this condition. Such approaches help to reduce fear and any expectations of catastrophic consequences that patients may hold. Clinicians should be aware that the language and communication style they use may have an impact (either positively or negatively) on the way the patient understands this episode of pain.
Encouragement of active physical therapy
Encouraging physical activity is vital to a patient’s recovery. Only advice to be physically active is needed early in the course of the patient’s pain; there is no need for a supervised specific exercise program at this stage. Encourage the patient to walk regularly, move about their home and maintain their work (with short-term appropriate modification of activities). Once the patient has recovered there is value in considering an exercise program. Trials have shown that exercise programs begun at this point can halve the risk of recurrence.6
Risk stratification
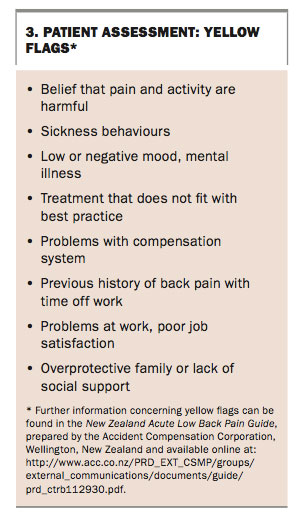
Early appropriate treatment of acute LBP may reduce the risk of developing chronic LBP with its inherent physical, psychological, social and economic costs. Factors associated with the transition from acute to chronic pain include psychosocial issues involving interpersonal and workplace relationships as well as incongruous beliefs and behaviours in response to pain. These psychosocial barriers to recovery are referred to as yellow flags (Box 3). Assessment tools such as STarT Back or Orebro may be used to assess the presence of yellow flags.7,8
{kind=link}
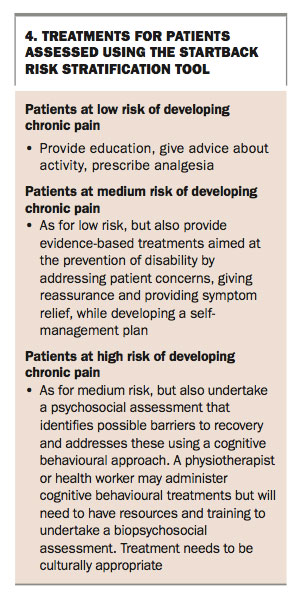
A significant improvement in acute LBP outcomes has been shown to occur when those people identified as having psychosocial barriers to recovery are stratified according to their risk of developing chronic pain by using questionnaires such as Orebro and STarT Back. The stratification approach allows the appropriate allocation of treatment resources based on the assessed implication that yellow flag issues may act as barriers to recovery. By using this approach, therapies can be targeted and then weighted towards the most at-risk group. For example, the STarT Back tool allocates patients to low-, medium- and high-risk groups. The treatment ramifications of this allocation are listed in Box 4.
{kind=link}
The IMPaCT study carried out in primary care showed a large, clinically important outcome difference among patients categorised and treated as high risk using such an approach. Their mean time off work was 50% shorter and the proportion of patients given sickness certifications was 30% lower than among patients given usual care.9
Analgesia
Guidelines recommend NSAIDs for short-term use in patients with acute LBP.10-12 Assessment for contraindications is required before prescribing NSAIDs. These include severe hypertension, renal disease, previous gastrointestinal haemorrhage and current corticosteroid use. The lower incidence of gastrointestinal side effects associated with COX-2 selective NSAIDs needs to be balanced with the increased cardiovascular risk associated with some of this group of drugs. Nonbenzodiazepine muscle relaxants have also been shown to provide pain relief in acute LBP.13
The use of paracetamol in acute LBP has been questioned in a recent study that showed patients treated with regular or as-needed paracetamol had similar recovery times compared with patients who were given a combination of patient education and placebo.3 The use of medications approved for the treatment of neuropathic pain has not been shown to be helpful in patients with nonspecific LBP.
Persisting pain in conjunction with nonrestful sleep may prompt the addition of a tricyclic antidepressant agent as a pain-modifying agent. The judicious short-term use of short-acting, low-dose opioids may also be required. However, in general, opioids are best avoided.
Cognitive behavioural therapy
Identifying problems such as fear avoidance, inappropriate attitudes to activity, low mood and stress allows targeted treatment that will improve pain.14 In both the assessment and treatment phases the careful use of language that informs without fuelling fear is vital.
Cognitive behavioural therapy informs the delivery of physical therapies that create awareness of the links between beliefs and pain behaviours. An example is the encouragement of patients to undertake a controlled quantum of activity, starting from a low base and gradually increasing activity over time (i.e. paced activity). This will lead to realistic goal-setting strategies as part of the overarching strategy of facilitating a self-management approach and helping to restore health autonomy.
No imaging for nonspecific low back pain
There is not always a correlation between radiological features and the cause of LBP. More than 90% of adults older than 65 years have radiological signs of disc degeneration, but less than half of these people have symptoms. The use of imaging for nonspecific LBP (i.e. in the absence of red flags) is not recommended.15 There is no evidence that imaging in these situations leads to improved patient outcomes. Indeed, the language used in radiological reports may, when read by some patients, contribute to fear avoidance activity and thus delay recovery. As such, inappropriate imaging may not only be unnecessary but may, in some cases, be detrimental to improving patient outcomes.
Review
All people with acute LBP should be followed up until their function has improved and pain has resolved. Specific practice points for GPs are given in Box 5. Early access to specialist medical, pain management or psychological care needs to be available if it is clear that LBP is persisting. If there is persisting LBP after three months, then referral to a musculoskeletal specialist
or chronic pain management team is recommended.
{kind=link}
Conclusion
A detailed history and initial examination of patients presenting with LBP allow the primary care practitioner to triage patients into one of three groups with a clear pathway of care for ongoing treatment and investigation. Traditional approaches to assessing and treating LBP have had significant limitations with regard to addressing the transition from acute to chronic low back pain. New approaches provide the opportunity to prevent this transition by allowing early identification of patients who are most at risk of developing chronic pain, as well as providing a more rational approach to medical imaging and an increasing emphasis on patient education as a means to self-management. MT
Acknowledgements
This article is based on the NSW Agency for Clinical Innovation (ACI) Model of Care for the Management of People with Acute Low Back Pain, available online at www.aci.health.nsw.gov.au/__data/assets/pdf_file/0007/336688/acute-low-back-pain-moc.pdf. This document was developed by the ACI Musculoskeletal Network. The lead writers were Professor Chris Maher, Dr Chris Needs, Dr Manuela Ferreira, Dr Niamh Moloney and Robyn Speerin.
References
- NSW Agency for Clinical Innovation (NSW ACI) Musculoskeletal Network. Management of people with acute low back pain. Sydney: NSW Health; 2016. Available online at: https://www.aci.health.nsw.gov.au/__data/assets/pdf_file/0007/336688/acute-low-back-pain-moc.pdf (accessed June 2017).
- Murray CJ, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012; 380: 2197-2223.
- Williams CM, Maher CG, Latimer J, et al. Efficacy of paracetamol for acute low-back pain: a double-blind, randomised controlled trial. Lancet 2014; 384: 1586-1596.
- Walker BF, Muller R, Grant WD. Low back pain in Australian adults: the economic burden. Asia Pac J Public Health 2003; 15: 79-87.
- Downie A, Williams CM, Henschke N, et al. Red flags to screen for malignancy and fracture in patients with low back pain: systematic review. BMJ 2013; 347: f7095.
- Choi BK, Verbeek JH, Tam WW, Jiang JY. Exercises for prevention of recurrences of low-back pain. Occup Environ Med 2010; 67: 795-796.
- Hill JC, Whitehurst DG, Lewis M, et al. Comparison of stratified primary care management for low back pain with current best practice (STarT Back): a randomised controlled trial. Lancet 2011; 378: 1560-1571.
- Linton SJ, Boersma K. Early identification of patients at risk of developing a persistent back problem: the predictive validity of the Örebro Musculoskeletal Pain Questionnaire. Clin J Pain 2003; 19: 80-86.
- Foster NE, Mullis R, Hill JC, et al. Effect of stratified care for low back pain in family practice (IMPaCT Back): a prospective population-based sequential comparison. Ann Fam Med 2014; 12: 102-111.
- Roelofs PD, Deyo RA, Koes BW, Scholten RJ, Van Tulder MW. Nonsteroidal anti-inflammatory drugs for low back pain: an updated Cochrane review. Spine 2008; 33: 1766-1774.
- Bernstein IA, Malik Q, Carville S, Ward S. Low back pain and sciatica: summary of NICE guidance. BMJ 2017; 356: i6748.
- Qaseem A, Wilt TJ, McLean RM, Forciea MA. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med 2017; 166: 514-530.
- Abdel Shaheed C, Maher CG, Williams KA, McLachlan AJ. Efficacy and tolerability of muscle relaxants for low back pain: systematic review and meta-analysis. Eur J Pain 2017; 21: 228-237.
- Nicholas MK, George SZ. Psychologically informed interventions for low back pain: an update for physical therapists. Phys Ther 2011; 91: 765-776.
- Koes BW, van Tulder M, Lin CW, Macedo LG, McAuley J, Maher C. An updated overview of clinical guidelines for the management of non-specific low back pain in primary care. Eur Spine J 2010; 19: 2075-2094.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.