Beware the cauda equina – not just another low back pain

Low back pain is a common presentation that is often managed conservatively. However, in this patient, severe worsening pain on a background of chronic back pain after injury is a neurosurgical emergency.
As a GP working in your own practice and the local hospital emergency department (ED), you care for many patients with low back pain. Since a close relative underwent spinal surgeries, you have maintained an interest in ‘back pain’ and feel comfortable assessing and managing patients with this complaint.
Case scenario
During a weekend shift in the ED, you see the next patient – a 40-year-old woman who has been assessed as triage category 3, to be seen within 30 minutes. She has low back pain that, although not acute, is severe and worsening.
From the end of the bed, the patient appears to be in considerable pain. You introduce yourself and scan her vital observations, especially her temperature. These are all unremarkable. Her pain score is 8/10 despite the administration of paracetamol 1 g an hour ago.
Sitting next to the patient, you elicit the following history. About a month ago she ‘put her back out’ helping her daughter move into an apartment. The pain resolved with a couple days of rest and paracetamol. Ten days ago, while lifting heavy groceries from the boot of her car, she experienced severe pain in her lower back radiating down her left leg to her calf. It did not improve with rest, analgesia and a hot water bottle. Nor did a visit to a chiropractor help much.
Three days ago, she went to her GP who prescribed oxycodone/naloxone and diazepam, told her to rest and briefed her of possible complications and what to look out for. This included advice to attend the ED if her condition did not improve or worsened.
The patient is apologetic about her husband having to drive her to hospital and about coming to a busy ED on a weekend. She repeatedly says, ‘it is probably nothing … I’m just not fit and I’ve been lifting heavy objects’ and it was ‘just a sprain’.
Assessment
The patient’s past medical history is unremarkable, and she takes no regular medications and has no allergies. Apart from childbirth, she has had no hospital admissions. She is married with one daughter and works in a clothing store.
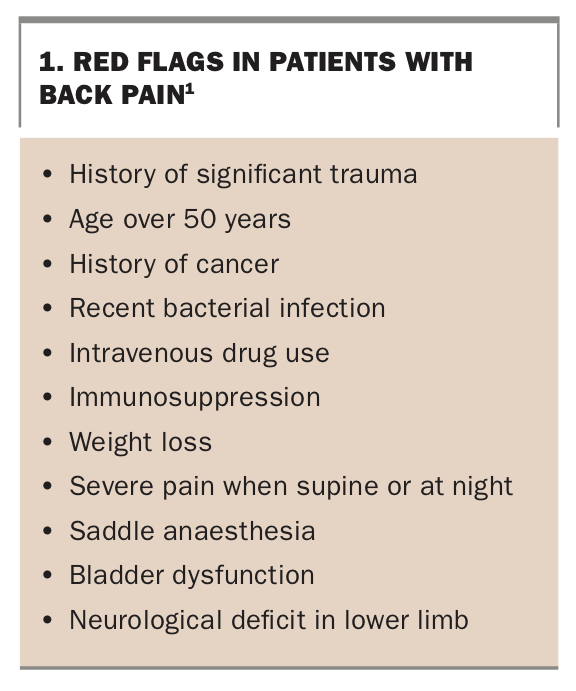
You assess her for ‘red flags’ for back pain (Box 1).1 Quickly, you become much more concerned as she describes difficulty with micturition, difficulty with her gait and pain down both legs.
{kind=link}
You administer intravenous morphine and metoclopramide for the severe pain and spasms, but it remains difficult to perform a thorough neurological examination. However, it is easy to ascertain saddle anaesthesia, decreased anal tone and reflex, as well as abnormal tendon reflexes and decreased sensation at several levels. Left foot drop is also evident. The diagnosis of a cauda equina lesion is strongly suspected.
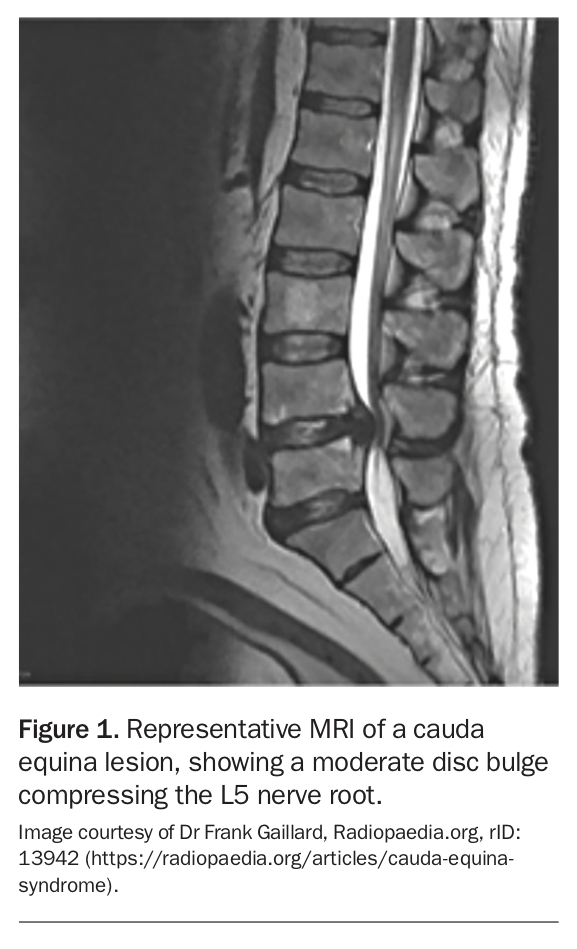
Although it is a weekend, the on-call neurosurgeon and radiologist agree that an urgent MRI is indicated. The MRI shows disc bulges at L3/L4 and L4/L5, with canal stenosis at those levels and severe compression and mass effect on the cauda equina nerve roots. A moderate disc bulge is compressing the left L5 nerve root (Figure 1).
{kind=link}
Management and outcome
The patient reports she has not eaten in the past six hours, and urgent surgery to decompress the cauda equina is organised. This shows a large disc fragment compressing the cauda equina nerve roots. After surgery, the patient recovers well. However, she is left with moderate left foot drop and muscle wasting and numbness of the left lateral lower leg and foot.
Discussion
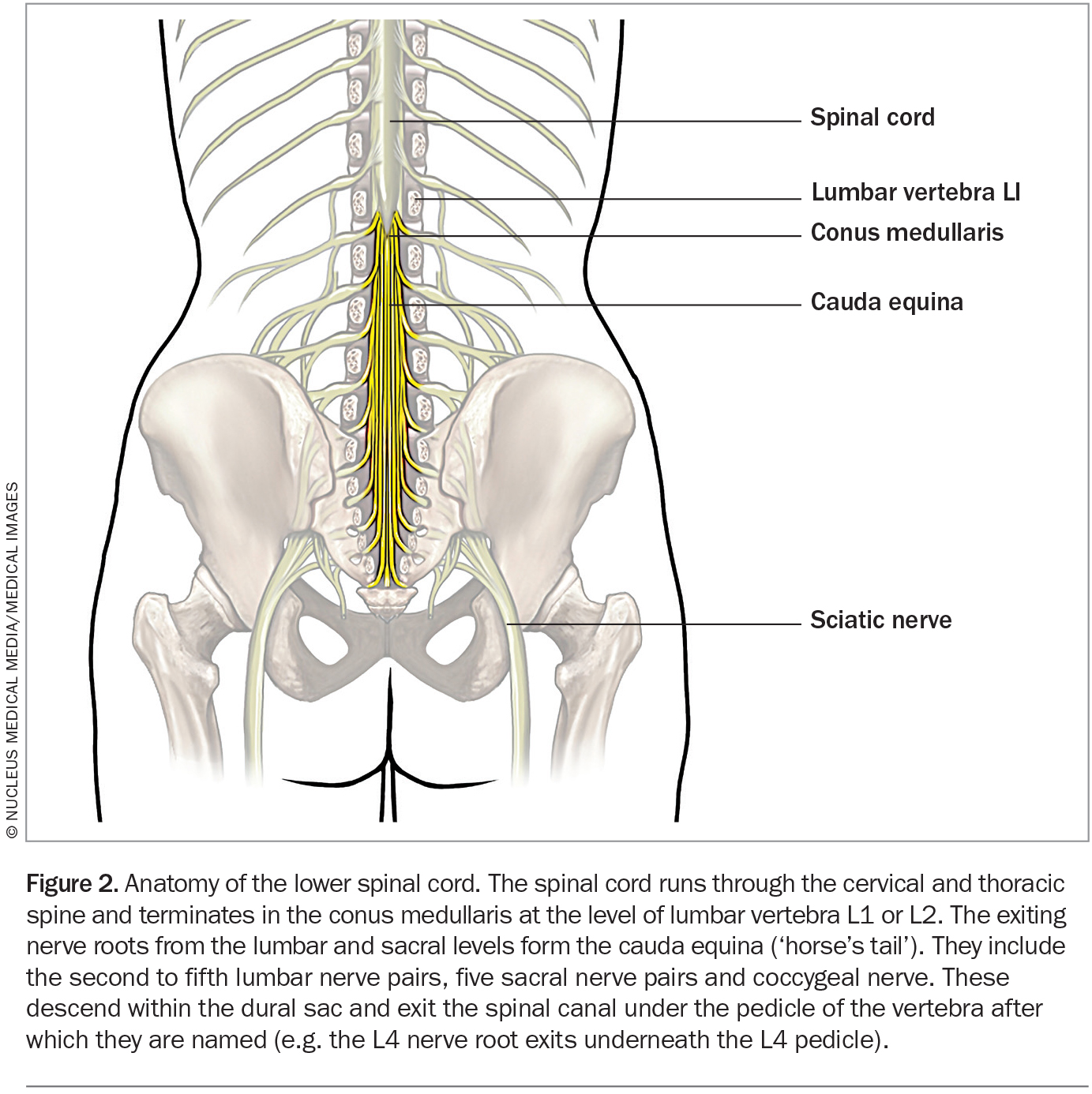
Cauda equina syndrome is a rare but serious condition that occurs when the nerve roots of the cauda equina are compressed, disrupting motor and sensory function to the bladder, bowel and lower limbs (Figure 2). It can lead to urinary or faecal incontinence, sexual dysfunction and even permanent paralysis. The incidence of cauda equina syndrome is about one per 1.8 million population per year, and one per 830 patients with symptomatic disc herniation per year.2 It is more common in men and older age groups.3
{kind=link}
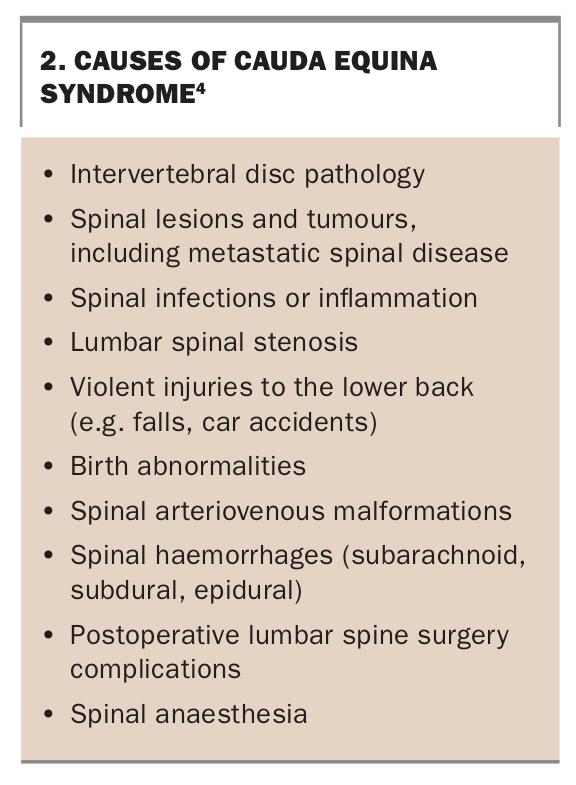
Cauda equina syndrome is caused by involvement of two or more of the cauda equina nerve roots (lumbar 2 to 5 and sacral 1 to 5 nerve roots and the coccygeal nerve) by an intraspinal lesion.3 The most common cause is intervertebral disc pathology, such as a herniated disc or disc fragment, as occurred in this patient. Disc pathology can result from a single excessive strain or injury. However, degeneration of the disc material and surrounding ligaments with ageing can also lead to disc rupture after a relatively minor strain or twisting movement.4 Cauda equina syndrome also commonly results from spinal compression caused by metastatic spinal disease. Other potential causes are shown in Box 2.4
{kind=link}
Despite its rarity, cauda equina syndrome is important to keep in mind in patients with low back pain because of the potentially devastating consequences and the need for urgent (same day) treatment to prevent these. Immediate surgical decompression of the cauda equina is imperative. The longer the delay, the less recovery of bowel, bladder and other function can be expected.
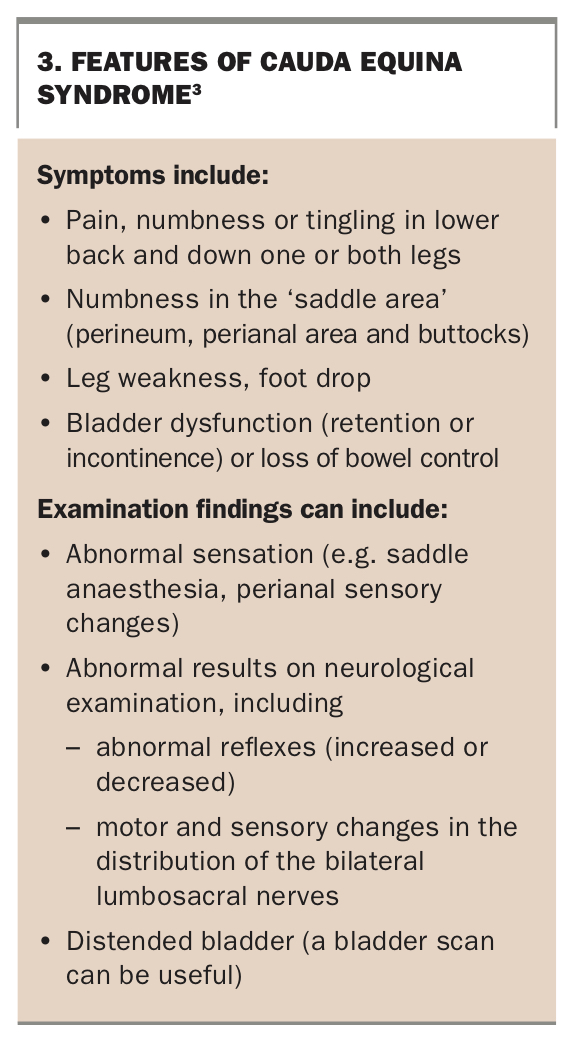
Symptoms and examination findings that suggest cauda equina syndrome are shown in Box 3.3 Cauda equina syndrome can involve frank urinary retention or incomplete retention, including sensory changes, reduced urinary sensation, loss of desire to void or a poor stream. In patients with an insidious onset or pre-existing urinary problems, incomplete retention can be more difficult to recognise. Once urinary retention has occurred, the prognosis is worse.2
{kind=link}
In all patients with low back pain, initial assessment should include an enquiry about bowel and bladder function, as well as a brief screening neurological examination of the lower limbs. Any bowel or bladder dysfunction on history or neurological deficit in the lower limbs raises the possibility of cauda equina. This should lead to testing for perineal sensation, anal wink and anal tone. Regardless of these findings, a low threshold for requesting spinal imaging and urgent specialist review is advisable. CT has a sensitivity of only about 80% in acute cauda equina syndrome, and MRI is the imaging modality of choice.
The diagnosis of even possible cauda equina syndrome is a time-critical neurosurgical emergency to attempt to minimise the potential significant morbidity and disability. This can include loss of bowel, bladder or sexual function or even paraplegia. These outcomes frequently occur if there is any delay and if so, subsequent litigation is not unusual. In the UK, about 10% of cases of cauda equina proceed to litigation.2 Among these cases, the mean delay to treatment was over six days.2
Fortunately, in this patient, suspicion of cauda equina syndrome and urgent investigation led to a timely diagnosis and rapid surgical intervention. Although the patient experienced some residual disability, she avoided serious and debilitating complications such as a need for a colostomy or bladder care, or paralysis. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.