Axial spondyloarthritis: what is it and how is it diagnosed and managed?

Back pain is very common in the community, and therefore an evidence-based referral strategy is valuable to guide GPs in referring patients with inflammatory back pain when axial spondyloarthritis is suspected.
Ankylosing spondylitis (AS) is the recognisable name that has been used to describe inflammatory arthritis of the spine and sacroiliac joints (SIJs) for decades, although the naming of this group of conditions has evolved. To be classified as having AS a patient has to have erosive damage in their SIJs detected on plain radiograph; however, we know that the inflammatory arthritis starts long before erosions are detected in the SIJs with plain radiographs. Patients who present earlier can have inflammation detected on MRI that has not caused erosions in the SIJs. This condition in these patients has now been given the name nonradiographic axial spondyloarthritis (nr-axSpA).1 Therefore, to bring together these two concepts, the umbrella term ‘axial spondyloarthritis’ (axSpA) has been introduced. AxSpA encompasses both nr-axSpA (which can be considered an early form of AS) and AS.
Epidemiology and clinical features
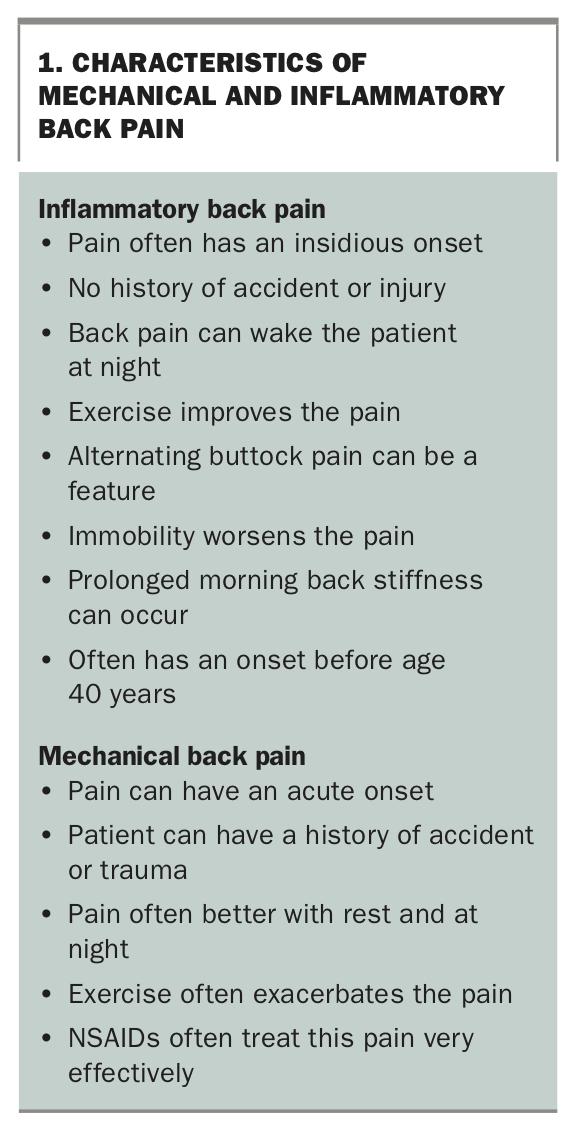
AxSpA has a prevalence of 0.3 to 1.4%.2 It can present in both men and women; the AS entity (as defined by the presence of erosions on plain film) is more common in men, but research has identified a higher prevalence of women in the nr-axSpA cohorts. Patients with axSpA can present with chronic back pain that can have ‘inflammatory’ characteristics. Inflammatory back pain differs from mechanical back pain, as shown in Box 1. Inflammatory back pain has high sensitivity (81 to 90%) for diagnosing axSpA but not high specificity (44 to 59%).3 Therefore, this type of back pain is useful in screening for axSpA but less useful for diagnosis.
{kind=link}
As well as inflammatory spinal arthritis, axSpA can be associated with enthesitis and peripheral arthritis, being characteristically a lower-limb inflammatory oligoarthritis. Patients with axSpA also have higher rates of anterior uveitis (iritis), skin psoriasis and inflammatory bowel disease.
Imaging
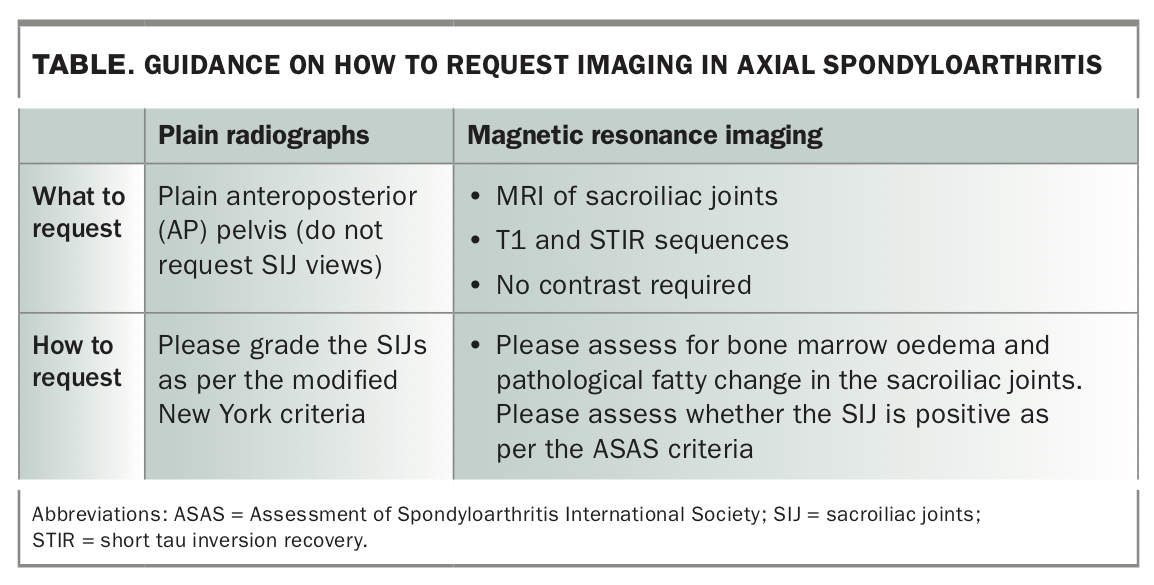
Imaging is important for the diagnosis of axSpA; however, it should be used in the context of an evidence-based screening strategy and in the right patient population (see section ‘Practical strategies for general practice’).4 Plain radiographs can show changes in the SIJs, but these can take five to 10 years to become evident. Plain anteroposterior pelvis views should be requested. Dedicated SIJ views should not be requested because of high inter-reader variation and these views not being used for making a diagnosis.
A more recent development in the diagnosis of axSpA is the use of MRI, which is sensitive for detection of inflammation in the SIJs. SIJ MRI does not require gadolinium contrast to make the diagnosis. Requestors should ask their radiology providers to assess whether the SIJ meets the Assessment of Spondyloarthritis International Society (ASAS) definition of a positive SIJ MRI scan, which is primarily based on the presence of bone marrow oedema in the SIJ.5 However, it is important to note that there is an appreciable false-positive rate. Studies have shown that athletes, runners, hockey players, military personnel undertaking basic training and women in the postpartum period can have false-positive SIJ MRI scans.6-9 Completing the MRI scan with the correct sequences (T1 and short tau inversion recovery [STIR], or other fat-suppressed sequence) is important to making a correct diagnosis, as is using the imaging results together with symptoms and laboratory tests. Guidance on what specific imaging to ask for and how to request it is provided in the Table.
{kind=link}
Laboratory tests
Assessment of C-reactive protein (CRP) level, erythrocyte sedimentation rate (ESR) and the presence of the HLA-B27 allele are the only laboratory tests of value when considering the diagnosis of axSpA. HLA-B27 is an ideal screening test but is unsuitable as a diagnostic test (see later section for further guidance on its use) as, despite being sensitive, it lacks specificity. This is because 50 to 80% of patients with axSpA are HLA-B27 positive, compared with around 7 to 9 % in healthy Caucasian populations. The HLA-B27 allele is also common in other ethnic groups but generally at slightly lower rates. Inflammatory markers such as ESR and CRP can be raised but are more commonly normal early in the course of axSpA, and even late in the disease course can be normal. Therefore, a finding of normal ESR and/or CRP level in no way reduces the probability of axSpA being present.
Practical strategies for general practice
Because the inflammatory arthritis is present five to 10 years before any abnormality shows on plain radiographs and inflammatory markers commonly remain normal, diagnosis of axSpA without MRI can be very challenging. The MRI scan can also be a challenge to interpret correctly, owing to the appreciable false-positive rate. Biologic treatments can only be prescribed by rheumatologists, so referral is often required for the diagnosis and management of axSpA.
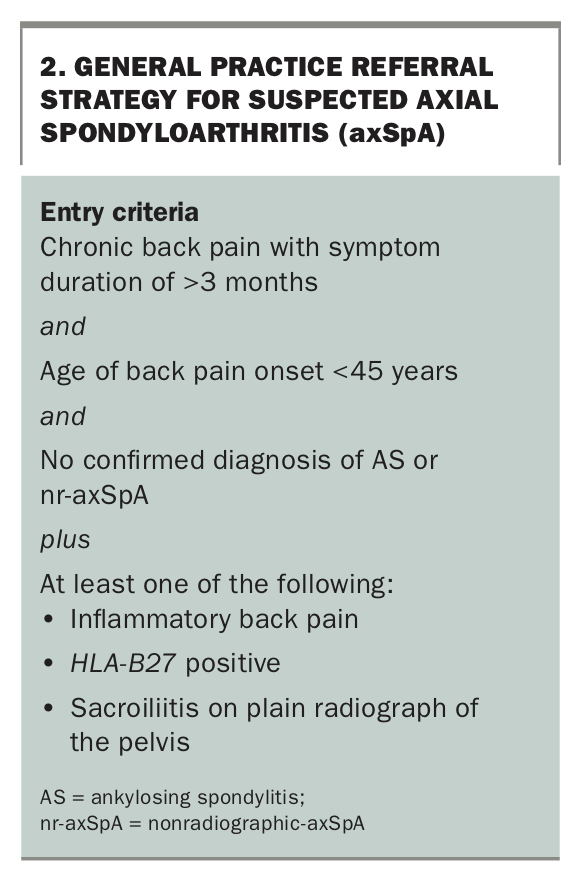
The challenge is that back pain is very common in the community, and therefore an evidence-based referral strategy is valuable to guide GPs in whom to refer. Such a referral strategy is shown in Box 2. Research has demonstrated that of patients selected based on a simple general practice screening strategy, 42% are diagnosed with axSpA in secondary care.10
{kind=link}
Diagnosis
AS is diagnosed when patients have symptoms of inflammatory spinal arthritis-like spinal pain in the presence of erosive damage evident on plain radiographs. This must be either bilateral grade 2 sacroiliitis or a unilateral grade 3 sacroiliitis based on the modified New York criteria.11
The diagnosis of nr-axSpA can be made when evidence of inflammation (bone marrow oedema) is present on MRI with a consistent clinical picture of inflammatory pain or other features of SpA. There is some controversy in the field about whether the diagnosis can be made in the absence of MRI evidence of inflammation, and such patients are currently included in the ASAS axSpA classification criteria. However, these criteria may well be revised in future.12-14 Pragmatically, patients with nr-axSpA who have an elevated CRP level or inflammation shown on an MRI scan respond to biologic treatment, whereas those patients without these features do not respond at a rate greater than that with placebo.15,16
Treatment
The initial treatment of axSpA (both AS and nr-axSpA) is with NSAIDs and physiotherapy. Physiotherapy should focus on maintaining flexibility throughout the cervical, thoracic and lumbar spine. There is good evidence for reduction in pain, improvement in physical function and spinal mobility and improvements in patient global assessment.17 There is no good evidence about superiority of different NSAIDs over each other. Naproxen, celecoxib, meloxicam or indometacin are commonly used.18 If patients have peripheral inflammatory arthritis, traditional oral disease-modifying drugs such as methotrexate, sulfasalazine or leflunomide can be used. However, these traditional oral agents are ineffective for treatment of the inflammatory spinal arthritis.
If patients have an inadequate response to the combination of physiotherapy and NSAID treatment, then moving to the use of biologics is often required if patients meet the PBS criteria. Biologic treatments currently reimbursed for axSpA are adalimumab (subcutaneous every two weeks), certolizumab (subcutaneous every two weeks or every four weeks), etanercept (subcutaneous weekly), golimumab (subcutaneous every four weeks), infliximab (intravenous every six weeks) and secukinumab (subcutaneous every four weeks).
There is no evidence for the use of osteopathy, chiropractic treatment, different diets, supplements or alternative medicines. Glucocorticoids are seldom used because they have to be used at very high doses (namely, 50 mg of prednisone) to achieve only a short-term response.19
Conclusion
AxSpA is not uncommon in the community. However, degenerative back problems are much more common. Selecting patients for further investigation is helped by an evidence-based referral strategy and the recognition that inflammatory markers and plain radiographs are often normal. AxSpA is a condition that has highly effective treatments available for patients, so awareness and recognising when to refer is paramount. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.