When helping harms: prescribing pitfalls in chronic noncancer pain

Medicolegal medicine
This series highlights common medicolegal issues in general practice. Written by a team from medical defence organisation Avant, it is based on actual cases with details changed for privacy and some issues summarised for discussion. This case scenario of a woman who died of multiple drug toxicity involving prescription medications highlights the dangers of inappropriate prescribing to treat chronic noncancer pain.
‘His medical practitioners did harm where they had only ever wanted to treat him for his known medical difficulties.'
Western Australian Deputy State Coroner Evelyn Vicker
The role of prescription medication in unintentional deaths has been considered at several recent inquests. The accidental death of any patient is tragic for the individual and their loved ones and distressing for practitioners involved in their care. It may also have medicolegal implications, leading to civil proceedings, a complaint to a professional body or even a criminal investigation. A coronial investigation may require a practitioner to give evidence at a public inquest, an experience that most doctors find confronting.
In deaths attributed to misuse of prescription drugs, the patient has often been prescribed opioids by multiple treating doctors after presenting to each with an episode of acute on chronic pain. However, inquests have highlighted other prescribing issues, including the combined use of opioids, benzodiazepines and psychotropic drugs, the use of injectable medications for pain treatment, as well as the use of benzodiazepines and quetiapine as first-line treatments for mental illness.
The following case scenario of a patient who died of multiple drug toxicity involving prescription medications derives from several cases that have proceeded to coronial inquests. It illustrates the medicolegal implications of inappropriate prescribing. It also highlights the need for clinicians to utilise available supports to help meet the potential challenges of managing patients with chronic noncancer pain.
Case scenario
In February, police contacted three GPs to report that their patient Jane Smith, aged 28 years, had been found dead at her home. An autopsy showed her death was due to multiple drug toxicity; the toxicology report stated that two opioids, three benzodiazepines, two antidepressants and an antipsychotic were present in her body. The three GPs were required to give evidence at a coronial inquest.
Patient history
Dr White had treated Jane for 10 years for multiple conditions, including chronic back pain after a motor vehicle accident, anaemia, endometriosis, migraine and urinary tract infections. Dr White had prescribed oxycodone for back pain and endometriosis (after an unsuccessful trial of ibuprofen) and sumatriptan for migraines. Jane had been in a dispute with her ex-husband over custody of their two small children. Dr White had prescribed diazepam or -temazepam at different times for insomnia and amitriptyline for anxiety and depression.
Jane had declined referrals to a pain management specialist and psychologist, stating she would pursue these when her life was more stable. Jane had never exhibited drug-seeking behaviour, and Dr White was shocked by her death.
Dr Black was a GP registrar practising near Jane’s workplace. Dr Black had treated Jane intermittently for four years for acute exacerbations of back pain and anxiety. At the first consultation, Jane became abusive after Dr Black offered a tramadol injection instead of the requested fentanyl patch. Jane had presented most recently to Dr Black in the previous December with acute pelvic pain, stating her GP was away for the school holidays. Because of her distress, Dr Black eventually gave her a private prescription for immediate-release oxycodone (20 x 5 mg tablets, one to be taken every six hours as needed), with four repeats.
Dr Jones had seen Jane five times in the year before her death. Dr Jones practised some distance away from Jane’s home, in the area where Jane’s new boyfriend lived. Dr Jones had prescribed oxycodone, diazepam, alprazolam and quetiapine for back pain, panic attacks and insomnia. In December, when Jane presented late one afternoon stating she was going away for the holidays and had left her prescription at home, Dr Jones prescribed fentanyl (25 mcg patch).
The inquest
The Coroner noted that in the last month of her life Jane had been prescribed multiple S8 and S4 medications and had also accessed her boyfriend’s sertraline. Individually, the dosage of the drugs was not in the fatal range. The Coroner observed on the one hand that no practitioner had a full understanding of Jane’s health needs, and on the other hand that Jane would not have met the criteria for a doctor-shopper.
The Coroner was not critical of Dr White’s care. Regarding Dr Black, the Coroner noted that, although she initially attempted to manage Jane’s drug-seeking behaviour, she failed to consider whether Jane was drug dependent and prescribed oxycodone on a private prescription, outside the PBS guidelines.
The Coroner was critical of Dr Jones, who had made no attempt to contact Jane’s regular GP or to explore nonpharmacological treatments, despite clear drug--seeking behaviour. His clinical records were scant.
The Coroner referred Dr Black and Dr Jones to the professional standards body.
Discussion
Establishing an effective therapeutic relationship with patients experiencing chronic noncancer pain can be challenging. Often there are not only significant medical factors but also mental illness and social problems. Patients have genuine pain and needs for analgesia, but in some, drug dependence can lead to drug-seeking behaviour. This behaviour can be sophisticated and manipulative, and clinicians may struggle to manage it effectively. Delays in access to specialist services can also complicate care, as can a history of fragmented care, limits to real-time verification of information, time pressures and disruptive behaviour. Prescribing mistakes often occur when clinicians are under pressure, such as at the end of the day or before a long weekend.
Based on experience at Avant, coroners are aware of the complexities of treating patients with chronic noncancer pain. However, coroners are likely to be critical when clinicians have prescribed outside PBS guidelines, have not considered whether patients are displaying drug-seeking or dependency behaviours, or have failed to explore nonpharmacological and non-opioid first-line treatments. Poor record-keeping also attracts criticism.
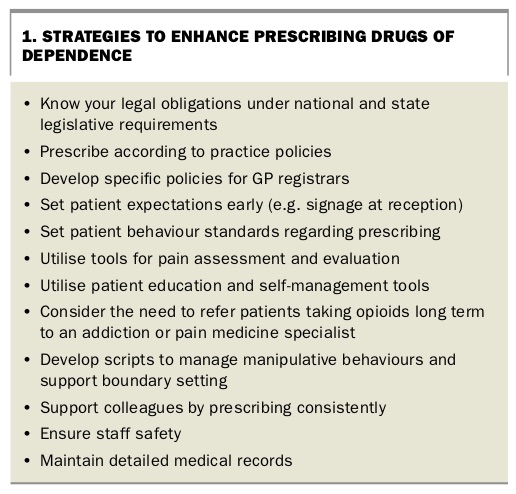
Strategies to enhance prescribing for chronic noncancer pain
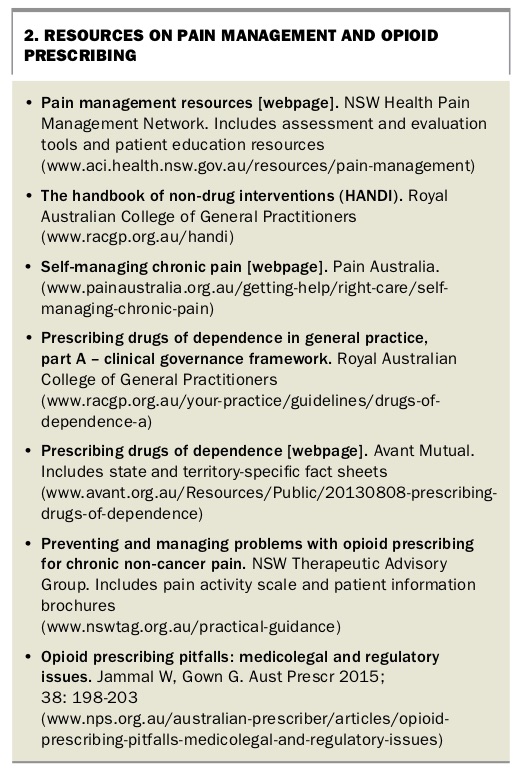
The complexities of managing patients with pain and demanding behaviour make prescribing drugs of dependence an issue that doctors should not manage alone. Strategies to enhance prescribing of drugs of dependence are summarised in Box 1. Some resources on pain management and opioid prescribing are listed in Box 2.
{kind=link}
{kind=link}
Adopt practice policies to support prescribing
Medications should be prescribed only in accordance with the evidence and in line with a clinical governance framework that is also endorsed by your practice colleagues. An example is the framework endorsed by the RACGP.1
Practice policies on criteria for identifying high-risk patients, the approach to urgent requests for high-dose medications, maximum opioid dosages and opioid review can help ensure consistency of prescribing across the practice. Policies such as not prescribing drugs of dependence to new patients and making these policies clear (e.g. through signs at reception) can also help set patient expectations early.
Enforcing prescribing policies across the practice requires accepting that some disruptive behaviour will occur. Reception staff should be trained to manage low-level confrontations and to escalate complaints appropriately.
Asking questions before joining a GP practice, such as whether it is RACGP-accredited and what policies are in place to manage prescribing drugs of dependence, can give doctors some indication of the practice support they can expect. GP registrars should ask what specific policies are in place to support their level of experience.
Comply with legislative requirements
Opioids are heavily regulated drugs. Prescribers must comply with the relevant state or territory legislative requirements in addition to the PBS requirements. Legal obligations for prescribing opioids to patients who are drug dependent or nondrug dependent differ across states and territories. Further, each state and territory has a different definition of dependency. It is important that prescribers understand the prescribing requirements and definitions of drug dependence and substance use disorder for the state(s) where they practise. With states taking different approaches to real-time prescription monitoring, it is also important to be aware of the system in your area.2,3
If you have concerns that a colleague is vulnerable or recognise that you have difficulty managing patient demands, speak up. Discuss your concerns with an experienced colleague, or contact your medical defence organisation (MDO) for advice.
Support the pain management plan
Treatment of patients with chronic noncancer pain should aim to maximise functional outcomes, minimise adverse effects and facilitate self-management of pain. Treatment must be defensible, evidence based and tailored to the patient’s needs. Utilising pain measurement tools and evaluation checklists can support clinical assessment and prescribing decisions and facilitate handover of care.
The source of pain can be difficult to establish with a physical examination. Functional and psychological assessment may provide additional information about the nature and severity of pain and can also elicit beliefs such as catastrophising, which can contribute to the patient’s pain perception. Evaluation tools such as the PEG (Pain Intensity, interference with Enjoyment of Life, interference with General Activity) assessment tool, the 5As of Analgesia, Örebro Musculoskeletal Pain Questionnaire or 8 Quick Steps assessment, provide a framework for discussion.
For long-term patients, self-reports are the most reliable indicators of pain intensity. Pain diaries and single or multidimensional pain measurement tools provide a baseline measure against which to assess presentations of acute pain as well as the patient’s progress towards therapeutic goals.
Use of these tools should be recorded in the patient record to provide evidence of your assessment.
Inform and educate the patient
Patient education should cover:
- the nature and expected duration of chronic pain
- treatment options (emphasising the value of nonpharmacological and self-management strategies)
- the limited role of medications
- specific risks of multiple drug use, opioid tolerance and dependence, the dangers of taking opioids, especially in large quantities or for long periods, and the risks of overdose.
In addition, discussing how to define success in pain management and being open about the unknowns of the patient’s condition can help mitigate unrealistic expectations.
Patient education resources on chronic pain can help reinforce information discussed. Online programs offer patients improved access to self-management strategies. Some examples are shown in Box 2.
Review your treatment plan regularly
Realistic goals should be discussed with the patient, along with how outcomes will be monitored. The patient should be reviewed regularly to monitor compliance with the treatment plan and frequency of prescription requests, including prescriptions provided by colleagues at your practice and others. A prescribing end-point (e.g. maximum dose) should be planned and clear boundaries set about withdrawal or reduction, particularly if you inherit a patient already taking opioids.
Consider regularly whether the patient has developed drug dependency and whether they should be referred to an addiction or pain medicine specialist. If the patient requires specialist review then ensure referrals contain complete clinical and prescribing information.
Conclusion
It is important to avoid the assumption that pain care is about identifying and excluding drug misusers. Patients with chronic noncancer pain have valid treatment needs and are entitled to compassionate and respectful care. They are also entitled to protection from iatrogenic harms. Although patients will make their own behavioural choices, a structured approach to their treatment includes minimising inappropriate prescribing. If things do go wrong, clinicians should be prepared to defend their clinical choices. If an inquest is planned, we recommend seeking assistance from your MDO to ensure you are represented during the coronial process and participating in the process by attending court to give evidence if requested to do so. MT
References
www.avant.org.au/Resources/Public/20130808-prescribing-drugs-of-dependence (accessed October 2018).
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.