Priapism related to antipsychotic drug use

Drug reactions
Priapism is a urological emergency. All men who are prescribed a psychotropic medication that has an associated risk of priapism need to be forewarned about this potential side effect. If priapism occurs, urological consultation should be immediately sought.
Case scenario
Recently, Mr PM had seen a psychiatrist and been prescribed olanzapine (10mg daily) to treat his opioid dependence and depression. Two weeks later, he reported a painful erection after taking his regular dose of olanzapine, without any sexual stimulation or trauma. Although he was in acute distress, he did not go to the emergency department because he believed the erection would subside on its own. The painful erection persisted overnight and Mr PM was rushed to hospital.
Initial physical examination suggested ischaemic priapism; this diagnosis was later confirmed by cavernous blood gas testing. Attempts to decompress the priapism through several corporal drainages and irrigation with phenylephrine were unsuccessful. Mr PM was subsequently admitted to the urology unit and emergency corporal shunts were performed with successful detumescence of his penis.
During his hospital admission, Mr PM was referred to consultation-liaison psychiatry services and olanzapine was discontinued. A pain specialist was consulted, and an appropriate pain management protocol was instituted to improve his opioid use and wean him off diazepam. A drug and alcohol rehabilitation specialist also visited Mr PM to treat his alcohol and drug dependence.
Commentary
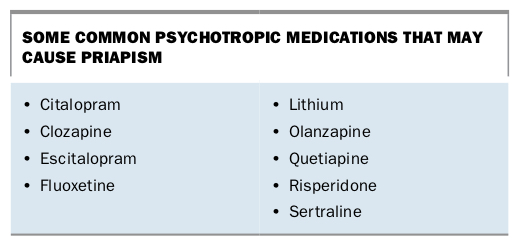
Priapism is a rare disorder characterised by an abnormal, prolonged, persistent, painful erection of the penis that persists more than four hours beyond or is unrelated to sexual stimulation.1 The incidence rate in men 40 years of age and older is 2.9 per 100,000 person years.2 Drug-induced priapism comprises 30% of cases and has been observed with a variety of medications, most commonly antihypertensive drugs. However, many psychotropic medications can also cause priapism, albeit at a lower incidence (Box).3
{kind=link}
The diagnosis of priapism is dependent on history, clinical examination and investigation. There are three subtypes: ischaemic (low-flow) priapism, nonischaemic priapism and stuttering priapism. Medication-induced priapism is likely ischaemic priapism. Psychotropic-induced priapism is almost always associated with ischaemic pathology and is thought to be caused by the alpha-1-adrenergic antagonism of these medications. Key clinical findings in ischaemic priapism are painful and fully rigid erection sparing the glans and corpus spongiosum, presence of venous blood gas parameters on corporal blood gas testing and absence of blood flow on colour duplex ultrasonography.
In Mr PM’s case, it is likely that olanzapine is the main cause for his ischaemic priapism. It is possible that the combination of narcotics, benzodiazepines and alcohol may have posed an additional risk for him. Although it is unknown if these drugs act in an additive or synergistic manner to cause priapism, combining drugs and alcohol with psychotropic medications increases the risk of priapism. There are wide variations in the interval between initiation of psychotropic medication and the onset of priapism, but emerging data suggest that this complication is most likely to occur within the first few weeks of treatment initiation.4
Olanzapine is usually classified as an atypical antipsychotic and is used to treat patients with schizophrenia and bipolar disorders. More recently, olanzapine has been used to treat opioid withdrawal and in other drug addiction treatment regimens due to its dopamine D2 and serotonin 5HT2A receptor activity. Although olanzapine has a relatively low potential for abuse, clinicians need to be aware of the possible additive risk of priapism and should be cautious in prescribing olanzapine in patients with opioid dependence and a history of multidrug use or polysubstance abuse. Prior to initiating therapy, clinicians need to discuss the side effects of olanzapine, including priapism, and documentation of informed consent may be necessary to protect against litigation. They should inform their patients of the potential for corporal ischaemia, fibrosis and subsequent erectile dysfunction from even a single episode of priapism.
Clinicians should always enquire whether a patient has a history of prolonged erections. Such patients need to be aware of their potential for developing priapism, since as many as 50% of patients presenting with priapism during psychotropic treatment have a history of prolonged erections.4 Certain medical conditions, other medications and substance abuse may also increase the risk of priapism.
If a persistent painful erection lasts more than two to three hours, the patient must obtain emergency care because corporal hypoxia and ensuing erectile dysfunction may occur after erections lasting four hours or longer. If priapism occurs, urological consultation should be immediately sought. Management of ischaemic priapism should achieve resolution as promptly as possible.5 Initial treatment is therapeutic aspiration with or without irrigation of the corpora. If this fails, intracavernous injection of sympathomimetic drugs such as phenylephrine is the next step and should be undertaken with cardiac monitoring. Surgical shunts should be performed if nonsurgical treatment has failed.
Patient education is crucial in avoiding olanzapine-related priapism and its potential long-term complications, especially in patients who may abuse multiple substances. Unfortunately, patients with priapism are often embarrassed or hesitant to seek help. It is important that patients who are prescribed olanzapine or other psychotropic drugs that cause priapism are informed of this side effect and of the need for rapid discontinuation of the medication and to seek medical attention if priapism occurs. Patient education about the risk of priapism is essential to avoid long-term complications, including erectile dysfunction, penile fibrosis and possibly penile gangrene.
Conclusion
Priapism is a urological emergency requiring identification of the underlying aetiology because prompt therapy may successfully alleviate the condition and minimise potential morbidities. Psychotropic-induced priapism is not uncommon. It is essential that patients who are to receive psychotropic medications be forewarned about its risk. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.