Managing complex and persisting pain in children and adolescents

Children's health
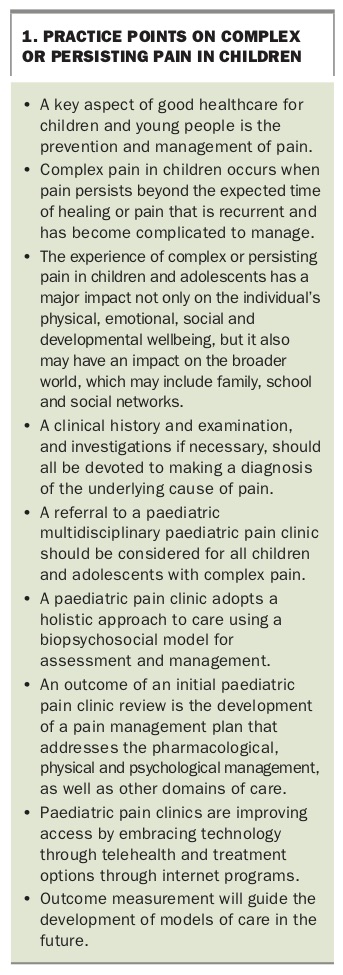
Persisting pain in children and adolescents is prevalent. GPs should consider early referral of young patients with complex or persisting pain to a multidisciplinary paediatric pain clinic that adopts a biopsychosocial approach to assessment and management. This may prevent the possible consequences of long-term pain, including psychological sequelae, school and social disruption and disability.
Pain is experienced as ‘an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage’.1 Pain is a subjective experience modified not only by biological factors, but also by previous painful experiences, the meaning and social context of the pain, fear, anxiety, depression and a range of other issues.
Chronic pain is defined as continuous or recurrent pain that persists past the normal time of healing, most commonly greater than three months’ duration.1 If chronic pain simply refers to any pain with this predetermined duration, then all persistent pain of childhood, such as that related to chronic disease (e.g. cancer, arthritis, sickle cell disease), neuropathic pain (e.g. complex regional pain syndrome, phantom limb pain) and recurrent pain syndromes (e.g. migraine, recurrent abdominal pain), could be classified as causes of chronic pain in children. An emerging term, ‘complex pain’, is increasingly used as an alternative term to describe pain in children which is persisting beyond the expected time of healing or pain which is recurrent and has become complicated to manage and includes medically unexplained pain. This is a new term that is clearer and reduces the stigma of the word ‘chronic’, which for many implies never-ending pain, especially when persisting pain in children can be treated.
To prevent the possible consequences of long-term pain in children, which may include psychological sequelae, school and social disruption and disability, early referral to a paediatric pain clinic should be considered (Box 1).
{kind=link}
Epidemiology of complex pain in children and adolescents
A systematic review has shown that the prevalence rates of chronic pain conditions in children vary substantially.2 Lower socioeconomic status was associated with higher pain prevalence, especially for headache. However, most studies included in the review did not meet high methodological quality criteria. A prospective, descriptive study of the characteristics of 207 children presenting to the chronic pain clinic at Royal Children’s Hospital, Melbourne, over two years reported concomitant medical conditions were present in more than 50% of patients, the most common conditions being cerebral palsy and malignancy.3 The incidences of school absenteeism, sleep disruption and inability to play sport were high (95%, 71%, 90%, respectively). Implied in these data is a significant burden of suffering for the children and families caring for them.
Complex pain in children may be under-recognised by clinicians. Barriers to recognition may include a child’s dependency on caregivers to be advocates and a reduced economic impetus towards a comprehensive approach for children with chronic pain as children do not impose a burden on the insurance and compensation system.4 In addition, children may be met with a dismissive attitude from caregivers, especially if no obvious cause of pain is found (Box 1).
How does a paediatric pain clinic operate?
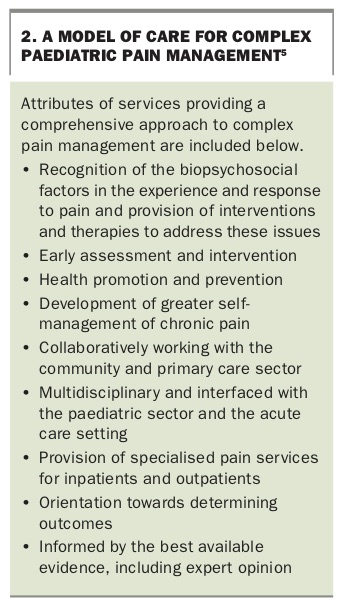
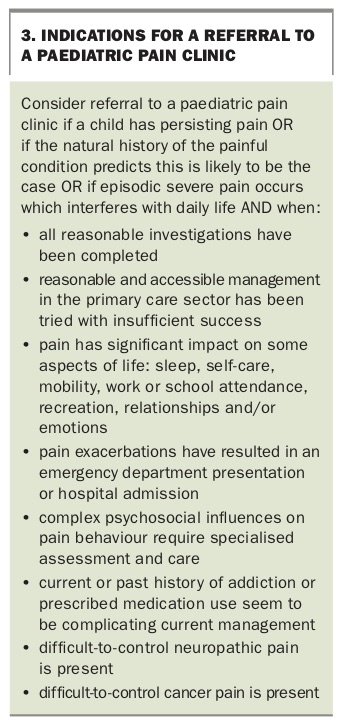
In recent years a multidisciplinary approach to chronic pain in children, through specialised clinics, has evolved in Australian and overseas centres (Box 2).5 There are now seven paediatric multidisciplinary pain clinics in Australia. All clinics have teams consisting of at least medical, physiotherapy and psychology support. For details of paediatric pain clinics in Australia, including contact details for referrals, see www.painaustralia.org.au/getting-help/pain-services-programs/pain-services. Indications for a referral to a paediatric pain clinic are listed in Box 3.
{kind=link}
{kind=link}
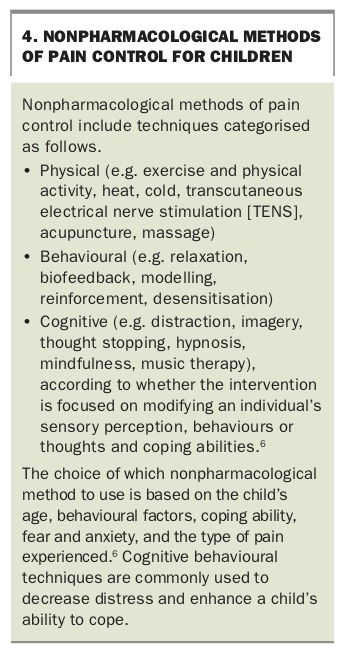
After a triage process ensuring an appropriate diagnostic process has been completed, the initial assessment in the pain clinic begins with a review of the electronic Persistent Pain Outcomes Collaborative (ePPOC) assessment data. A thorough medical history, including psychological and social factors, and a physical examination follow. After formulation of the key pain management issues, a discussion by the multidisciplinary team results in the development of a pain management plan. This plan must consider the nuances of each case and offer a support structure to support adherence. The pain management plan includes pharmacological and nonpharmacological approaches (Box 4) and individual and family therapy as required.6 In the discussion of the plan with the child and family, pain education occurs and arrangements are made to ensure the plan is implemented through referral to, or liaison with, local practitioners as indicated and follow up (telephone, clinic and/or telehealth). Liaison with the school and the implementation of a school pain management plan is often needed.
{kind=link}
What is the success of psychological therapies for complex pain in children and adolescents?
Psychological therapies are broad ranging and target pain-related cognitions and/or behaviours. They range in delivery modes, including face-to-face, internet, phone and, more recently, apps and websites. The effectiveness of psychological therapies across a range of delivery modes for children and adolescents with pain conditions has been evaluated recently by Cochrane and systematic reviews.7-9 These studies concluded that psychological therapies were effective in reducing pain intensity and disability for children with headache and nonheadache pain conditions.7-9
Referrals and categorisation of new presentations to a paediatric complex pain clinic
Referrals to paediatric pain clinics are generally accepted from GPs and medical specialists based in the community and within paediatric hospitals across Australia. From July 2017 to June 2018, the Children’s Hospital at Westmead (CHW) complex pain clinic saw 152 new patients. In keeping with previously published data, 64.1% of new patient referrals were female. Most presentations were for children over 13 years of age, which is also reflected in previously published Australian data.3 Most patients required at least one follow-up review in the clinic and adherence with treatment was generally good, resulting in most having a clinically significant improvement in quality of life and an improvement in functional disability.
Most patients presented to the CHW complex pain clinic with musculoskeletal pain (39%), including limb and joint pains (without hypermobility), back pain and avascular necrosis. Presentations of abdominal pain, complex regional pain syndrome, hypermobility with joint pain and postoperative pain were all similar in number (ranging from 8 to 13%). Persisting postoperative pain was defined as pain occurring beyond the time of tissue healing following a surgical intervention. Generalised body pain with somatising features and headaches was less commonly seen. Several additional presentations to the CHW complex pain clinic could not be categorised, including vaginal pain, ear pain, pain secondary to Fabry’s disease, itch and peripheral neuropathic pain.
New innovations in access to specialist services
Telehealth
In 2015, a six-month pilot study evaluating the use of telehealth as a modality for chronic pain management was conducted by the Agency of Clinical Innovation at two NSW chronic pain clinics: the CHW complex pain clinic and Orange Hospital.10 Healthdirect Australia provided the platform to the two pilot sites. The platform is internet browser based and has no licensing fees, necessity to download software or expensive cameras or screens, enabling direct access into clinician’s rooms and the patient’s home.10 During the six-month pilot phase at the CHW complex pain clinic, there was a total of 14 sessions and 3346km were saved in patient travel. During the trial, 100% of patients and clinicians stated they found it convenient, effective and educational and would recommend its use.10 Patients reported the large benefit was prevention of a flare up of pain which would likely have been the outcome of travel to such appointments. There was an increase in subsequent referrals from professionals who participated in telehealth sessions.10 This successful pilot study provided evidence for the use of telehealth in the management of children with complex pain. Most paediatric pain services have this capability in Australia.
Paediatric day pain program
In response to the need to create a new treatment option for high-school students who were making minimal improvements in the community and did not require inpatient admission and based on growing international evidence, the CHW complex pain clinic conducted its first multidisciplinary moderate-intensity group pain day program in 2013, titled ‘T.A.M.E Your Pain’ (Teaching Adolescents to Manage Pain through Exercise and Empowerment).11 The program runs for five days, split over two weeks, during school holidays.
The program integrates land- and pool-based physiotherapy, supervised practice of nonpharmacological pain management strategies, including deep breathing, mindfulness, relaxation and hypnosis, with education on goal setting, pacing, sleep management and flare-up prevention and management. Validated outcome measures used to evaluate the program demonstrated sustained improvements at 12 months’ follow up. These outcomes potentially support a cost-effective day program as an alternative to a costly hospital admission rehabilitation program.
Paediatric pain clinic outcomes
With the aim of improving pain services and patient outcomes through benchmarking of care and research, a chronic pain treatment outcomes registry, the ePPOC, was established in 2013 (http://ahsri.uow.edu.au/eppoc/index.html).12 In paediatric pain clinics, child self-report measures (for those aged 5 years and above) and parent/carer measures are collected. The paediatric measures selected are banded into age groups ensuring levels of development and language are appropriate. Measures of positive outcomes for a child with persisting pain after attending a complex pain clinic are listed in Box 5. The case study in Box 6 gives an example of a specific pain management plan.
{kind=link}
{kind=link}
A German study has confirmed inpatient and outpatient treatments elicit substantial changes in pain intensity, disability and school attendance in children with chronic pain.13 Of 105 patients who missed five or more days of school because of pain, 93 attended school regularly after treatment.3 Additionally, sleep disturbance improved in 88% of patients and 88% resumed sporting activity after multidisciplinary intervention.3 Outcome was classified as good in 134 patients (65%), moderate in 32 (15%) and poor in 16 (8%).3 Following further collection and analysis of ePPOC data, it is hoped further objective data will be obtained to determine the effectiveness of pain clinic outcomes and allow opportunities for improvement.
Conclusion
Persisting pain in children and young people is prevalent and distressing. It is important to recognise this as an entity and adopt a biopsychosocial approach to assessment and management. The indications for considering referral to a paediatric pain clinic are discussed in this article. Paediatric pain clinics are becoming more accessible to those who need them through use of telehealth, and the measurement of outcomes will guide the development of models of care in the future. MT
References
Chronic_Pain_Telehealth_Pilot_Project_Evaluation_report_2016_v2.pdf (accessed April 2019).
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.