Treating acne – how to minimise physical and emotional scarring

Dr See is a Dermatologist in private practice at Central Sydney Dermatology, Sydney; and is Co-Chair of the All About Acne group.
Dr Tong is a Dermatologist in private practice at Central Sydney Dermatology and Visiting Medical Officer at St Vincent’s Hospital, Sydney, NSW. He is a member of the All About Acne group (www.acne.org.au).
Acne
Skin conditions

Acne is a common skin condition associated with significant physical and psychological morbidity that affects people from prepubescence to middle age. Treatment should be individualised according to the patient’s history, severity of disease and contraindications. The psychological impact of acne should be acknowledged and considered when developing a treatment plan.
- Acne is not just an adolescent condition; it is also common in prepubertal children and middle-aged adults.
- There is psychological harm associated with having acne and this may not correlate with disease severity.
- GPs play an important role in helping to dispel common myths surrounding the causes of acne.
- Taking an accurate history, identifying patient concerns and evaluating psychological impact are key to successful acne management.
- GPs should set guidelines for treatment, have a plan to review treatment outcomes and establish realistic expectations with their patients.
- Treatments should be individualised according to the patient's history, acne severity and contraindications, and patients referred when necessary.
- Acne scarring can be avoided through early intervention.
GPs are at the frontline for managing acne in patients from prepubescence to middle age. Year by year, there are more acne treatments available and the minefield of information, especially on the internet and social media, can make management confusing. This article guides the reader to consider treatment options for acne to help address patients’ needs and concerns.
Since the last published article on acne in Medicine Today in 2015,1 there have been many developments in acne treatment – new products, new procedures and promising new medications currently on trial. There is even a new name for Propionibacterium acnes, the bacterium linked to acne, which is now called Cutibacterium acnes.
Epidemiology: is acne really that common?
Acne is a common skin condition that is associated with significant physical and psychological morbidity. International studies have shown about 85% of people between the ages of 12 and 24 years experience at least minor acne.2 It is particularly commonplace in teenagers in Australia, with a prevalence of 93.3% among those aged 16 to 18 years.3 Although commonly thought of as a teenage disease, acne can start in prepubertal children and may coincide with an earlier onset of puberty.4 Acne can also be considered a chronic disease.5,6 It may extend from adolescence, through the 20s, and even to middle age. The prevalence has been noted to be 64% in those aged 20 to 29 years and 43% in the 30- to 39-year age group.3
Patient concerns
Acne can cause significant psychological harm and can affect quality of life.7,8 Many studies link patients who have more severe acne and acne of a longer duration with a greater likelihood of low self-esteem and quality of life.9 People with acne can also experience lack of self-confidence, anxiety and depression. In the Global Skin Disease Study, acne ranked highly as a skin disease associated with significant disease burden.10,11 A recent Delphi survey showed that patients with acne reported:
- being self-conscious
- feeling unattractive to themselves and others
- feeling uncomfortable in their own skin
- not wanting pictures taken
- feeling envious of people with clear skin
- that time and effort was spent concealing scarring.12
Although previously considered a teenage concern, a recent meta-analysis found the prevalence of depression was higher among adults with acne (aged 20 years) compared with their adolescent counterparts (aged 12 to 19 years).13
Due to the chronicity of the condition, many patients can become disheartened and disillusioned with treatments offered to them. They often seek alternative measures, some of which have very little scientific basis. Many patients are now consulting social media platforms such as YouTube and Instagram, and social media influencers for advice – the advice given is not always in keeping with recommended acne guidelines.14
Patient concerns should be identified and addressed so that an individual management plan can be tailored to each patient. Patients with acne often question and are concerned about the possible side effects of acne medications such as oral antibiotics and oral isotretinoin. There is also increasing global concern about the use of antibiotics and increasing antibiotic resistance of bacteria. This may lead to patients not wanting to adopt antibiotic treatment strategies. It is recommended that antibiotic courses be limited to three to six months, and that topical and oral antibiotics are not prescribed simultaneously. Patients are also concerned about the possibility of acne scarring and it is important for the clinician to realise that early effective management can lessen the risk of this.15
The GP consultation
The GP is at the forefront of acne management, with presentations of chronic acne seen by Australian GPs at a frequency of 0.4 of every 100 consultations.16 Acne is diagnosed clinically by patient history and physical examination, which evaluates the type and severity of the acne and if there is any psychological impact. Laboratory investigations may be considered if there is a possibility of underlying hormonal factors, such as polycystic ovary syndrome, as a baseline for oral medications such as isotretinoin, or monitoring in the setting of spironolactone. Key questions to ask patients presenting with acne can be found in the Box.
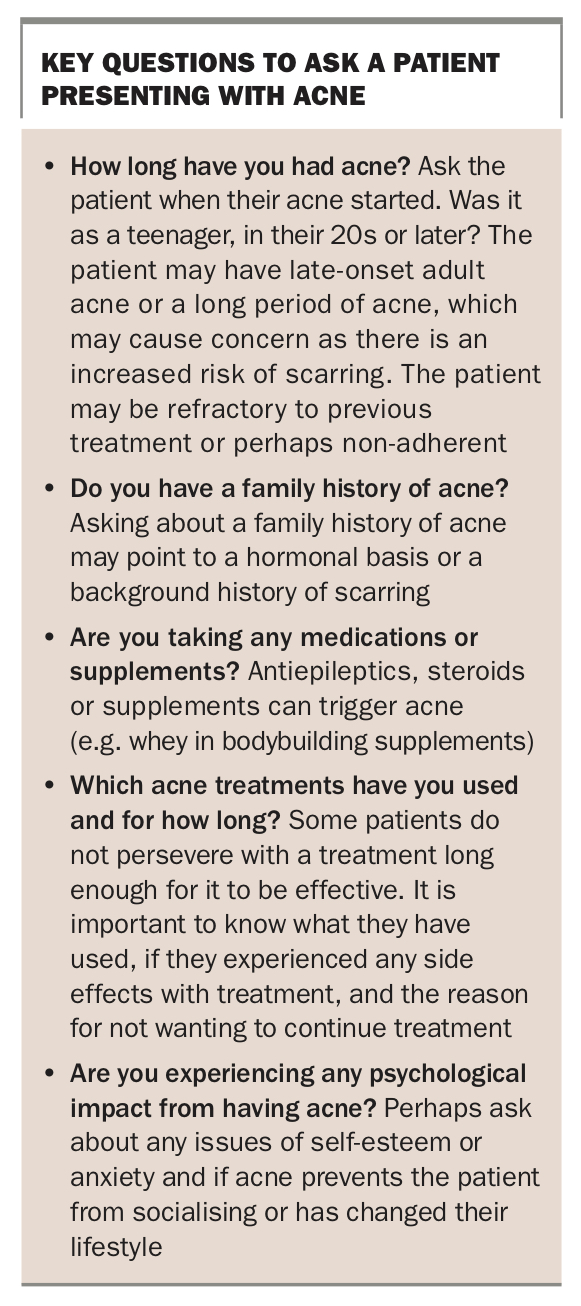{kind=link}
Although consultation time may be limited, it can be worthwhile asking patients what they think the cause of their acne is. The four main factors contributing to acne are:
- increased sebum
- hyperkeratinisation of the pilosebaceous duct
- colonisation by C. acnes (formerly known as P. acnes)
- immune activation and release of inflammatory mediators.
There are many myths around the factors that influence acne that should be dispelled. These include:
- acne is caused by poor hygiene
- only teenagers get acne
- popping pimples makes them go away faster
- acne scarring can be easily fixed
- acne always goes away on its own - it may eventually burn out after days, weeks, months, or years but, unfortunately, the longer a patient has acne, the greater the risk for permanent scarring.
Diet is a controversial triggering factor, with the common misconception that an unhealthy diet is always the cause of acne in every person. Recent evidence suggests that in a select group of patients, high sugar intake, high dairy intake and a high glycaemic index diet may contribute to the development of acne, thought to be mediated by mammalian target of rapamycin complex 1 (mTORC1) signalling (Figure 1).17
It is important to set realistic expectations for treatment success and to offer patients a review to see if management needs to be altered.
The physical examination
Acne severity can be quickly assessed by looking at the patient’s face and torso. There is no standard method of acne grading, it can be simply classified as:
- mild – noninflammatory or inflammatory comedones (blackheads or whiteheads; Figure 2a)
- moderate – with inflammatory papules and pustules (Figure 2b)
- severe – with deeper inflammatory nodules and cysts (Figure 2c).
{kind=link}
Many patients, especially those with darker skin (Fitzpatrick III or higher), may have postinflammatory redness or hyperpigmentation as inflammatory lesions resolve, which are often mistaken as active acne lesions or scarring.
Patients with severe acne with deep nodules and cysts that has not responded to treatment, and those with uncommon forms of acne such as acne conglobata and acne fulminans, may require urgent referral to a dermatologist for prescription of oral or intralesional corticosteroids or oral isotretinoin. Patients who have a psychological impact may require counselling with a psychologist or psychiatrist as well as referral for consideration of oral isotretinoin therapy.
Acne in adults can look the same as teenage acne. Both rosacea and perioral dermatitis can occur at the same time as adult acne but the clinical hallmark of acne is the comedone.
Investigations
Most patients with acne do not need laboratory investigations. Consider hormonal acne in patients who have symptoms of hyperandrogenism in the context of polycystic ovary syndrome; a hormonal assay should be performed in the luteal phase of the menstrual cycle after the patient has stopped taking the oral contraceptive pill for at least one month. Tests for women with suspected hormonal acne include measurement of serum dehydroepiandrosterone sulfate, total testosterone, free testosterone and sex hormone binding globulin levels and the luteinising hormone/follicle stimulating hormone ratio.8 Patients with hormonal acne who are also insulin resistant may be at risk of developing diabetes and cardiovascular disease later in life.
If patients are having baseline investigations for oral isotretinoin, it may be helpful to order the following tests: liver function tests, creatine kinase (in athletic patients) and fasting lipids. Beta human chorionic gonadotropin should be added as a pregnancy screen in female patients. In healthy individuals, less frequent ongoing monitoring may be safe for those who are receiving typical doses of isotretinoin.18
Treatment options
Acne treatments are tailored to each patient according to severity, as shown in the Table. Clinicians must always bear in mind that acne can fluctuate from time to time; therefore, taking an accurate patient history and developing a flexible treatment plan that accommodates fluctuations in acne severity are an important part of management.
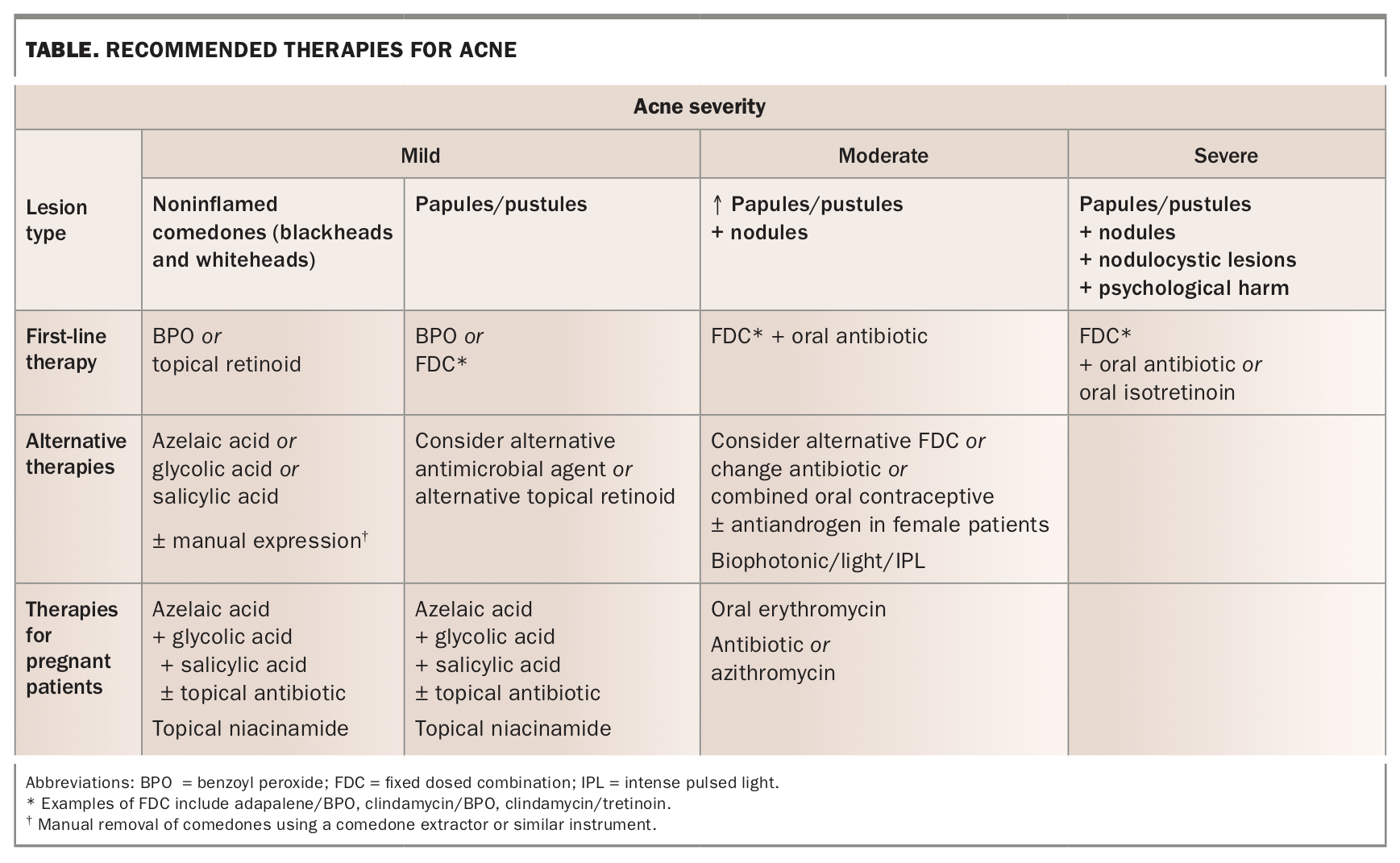{kind=link}
Patients often expect advice regarding skincare and the choice of skincare can be paramount to the success of treatment. There are many inexpensive skincare ranges that offer acne cleansers and moisturisers that aim to be gentle to the skin and not be occlusive. The use of an appropriate cleanser and moisturiser can also minimise the irritancy of many topical acne treatments as well as dry skin often associated with oral isotretinoin use.
Patients may also expect advice on diet and, as mentioned previously, it is important to dispel acne myths and consider offering patients an acne educational resource such as the All About Acne website (www.acne.org.au).
Mild acne
When seeing a patient for the first time, be mindful that they may have already been to a chemist or beautician for advice. They may have fixed ideas about what is causing their acne and, even in patients with mild disease, acne can have significant psychological impact that does not necessarily correlate with their acne severity.14
Acne cleansers can be beneficial for all types of acne and are available at pharmacies and supermarkets. Cleansers usually contain salicylic acid, glycolic acid, azelaic acid or benzoyl peroxide. Cleansing twice daily is ideal to remove excess sebum, keratinous debris, make up and pollution. Micellar water can also be used on sensitive skin. Non-prescription leave-on acne treatments can be used once or twice a day and may contain benzoyl peroxide, salicylic acid, glycolic acid or azelaic acid.
Benzoyl peroxide reduces pilosebaceous duct colonisation by C. acnes, as well as decreasing sebum and comedone formation. Gradual introduction and starting with a low concentration are recommended to minimise potential skin irritation. It is the active ingredient in acne facial washes or leave-on creams and has also been incorporated into the fixed-dose combination prescription products clindamycin phosphate/benzoyl peroxide and adapalene/benzoyl peroxide combinations.
Alpha hydroxy acids such as glycolic acid (and others such as lactic, citric and mandelic acid) and the beta hydroxy acid, salicylic acid, decrease altered follicular keratinisation in blocked oil glands and improve skin appearance by exfoliation.
Azelaic acid works by inhibiting C. acnes growth and improving abnormal pilosebaceous follicular keratinisation. It has fewer irritant side-effects compared with benzoyl peroxide.
Prescription first-line therapy for mild acne usually consists of a topical fixed dose combination. The combination products tend to be more effective, work faster and target more areas of acne pathogenesis than monotherapy. They are applied at night to a cool dry face and are not used as spot treatments. Patients should be followed up eight to 12 weeks after starting treatment to assess its effectiveness and determine whether a change should be made. Therapies include:
- clindamycin phosphate 1% plus benzoyl peroxide 5% (not listed on the PBS)
- adapalene 0.1% or 0.3% plus benzoyl peroxide 2.5%, note that there are two strengths (currently listed on the PBS)
- clindamycin phosphate 1% plus tretinoin 0.025%, the newest combination (not listed on the PBS).
Moderate acne
Patients with moderate acne have more lesions, characterised by papules and pustules, and usually require oral treatment, including an oral rather than topical antibiotic. Women with unresponsive acne may benefit from the oral contraceptive pill, cyproterone acetate or spironolactone.
Oral antibiotics
Oral antibiotics have been prescribed for decades as an acne treatment. They work by suppressing C. acnes growth and have anti-inflammatory action. Due to the growing concern over antibiotic resistance, use with topical benzoyl peroxide, topical retinoid and/or a probiotic is recommended. Oral antibiotics should not be used simultaneously with a topical antibiotic and the duration of usage should be limited to three to six months.
Doxycycline is probably the most prescribed oral antibiotic, at an average daily dosage of 100 mg daily; however, doses can range from 50 to 200 mg daily. Doxycycline should be taken with water, not milk, and should not be taken before lying down or at bedtime because of the risk of oesophageal irritation. It is not recommended for children under 12 years of age due to the risk of tooth discolouration, or in women who are pregnant or breastfeeding.
Minocycline at a dosage of 100 mg daily is also prescribed. However, there are rare safety issues associated with its use including minocycline-induced hepatitis, drug-induced lupus-like hypersensitivity syndrome and hyperpigmentation.
Erythromycin 500 mg twice daily is also effective but C. acnes resistance and gastrointestinal side effects are more common. It is used in children and pregnant women, in whom tetracycline is contraindicated.
Other antibiotics such as trimethoprim can also be used as third-line therapy at a dosage of 200 to 300 mg twice daily. Although not commonly used, azithromycin has been considered as effective as doxycycline in some trials.19 The dosage of 500 mg once daily for three days per week or in cycles of 10 days for 12 weeks are the most commonly used regimens.20
Hormonal therapy
The most commonly prescribed antiandrogen hormonal therapies for moderate acne are the oral contraceptive pill, cyproterone acetate and spironolactone. These can be prescribed as monotherapy, or as oral contraceptive/spironolactone or oral contraceptive/cyproterone acetate combinations. These therapies can be effective in women with acne, especially those who show resistance to other therapies, and can even be effective when serum androgen levels are normal. They work by decreasing ovarian and adrenal androgen production and also inhibit the local activity of androgen nuclear receptors on sebocytes and keratinocytes.21 Before prescribing an oral contraceptive, it is important to check for any contraindications.
Women over the age of 25 years may have higher rates of treatment failure.17 Suspect hormonal acne in women who fail multiple courses of systemic antibiotic medications or if there is a recurrence of acne shortly after treatment with isotretinoin.22,23
Patients may not see an improvement in their symptoms until after three months of taking an oral contraceptive for acne and the best response rate may not be seen until after six to nine months of treatment. Acne has been shown to improve in 50 to 90% of cases.16 Many patients may experience a flare of their hormonal acne when their long-term oral contraceptives are ceased. Some patients may also have a worsening of their acne when contraceptive implants are used.24
Cyproterone acetate reduces sebum production and is usually given in combination with the oral contraceptive pill at a dosage of 12.5 to 50 mg daily during the first 10 to 15 days of the menstrual cycle. It can also be prescribed on its own at a dose of 50 to 100 mg daily from day 1 or 5 of the menstrual cycle and stopped before ovulation on day 14. An improvement is usually seen within three months.
Spironolactone is a safe and effective treatment requiring no monitoring in a young fit and healthy female.25 Treatment can be started with a low dose such as 25 to 50 mg twice daily and then increased to 200 mg daily if the patient has no significant adverse events such as breast tenderness, ‘breakthrough’ bleeding or headache. Improvement in acne may take up to three months. Spironolactone is contraindicated in pregnancy because of the risk of feminisation of the male fetus.
Severe acne
For patients with widespread and inflammatory deep lesions, oral antibiotics, often in conjunction with a topical retinoid, are the treatment of choice. Consider referral to a dermatologist for oral isotretinoin in the following situations:
- patients with severe acne that is unresponsive to treatment
- patients at risk of scarring
- patients with psychological distress as a result of their acne.
When referring for isotretinoin, some baseline investigations can be done, as mentioned previously. The daily dose and duration of treatment depends on the patient’s weight, response to treatment and any side effects experienced. There is no standardised isotretinoin dose, and many dermatologists tend to start patients on a low daily dose and then gradually increase it as tolerated.26 Female patients should be counselled on the need for contraception, as isotretinoin is teratogenic. All patients should be advised to report any mood changes to their GP or specialist and more regular review may be required. In the rare event of psychological distress or a psychiatric disorder resulting from isotretinoin use, consider referral to a psychologist or psychiatrist.27
Acne medication and pregnancy
Topical and oral retinoids are contraindicated during pregnancy because of the risk of birth defects, and tetracycline antibiotics should not be given due to the risk of deposition and staining of the infant’s teeth. Treatment options for pregnant women include topical non-tetracycline antibiotics, azelaic acid, topical niacinamide and topical alpha hydroxy acids such as glycolic acid (Table).28
Adjuvant therapies
The following therapies may improve patients’ appearance and be helpful additions to the overall treatment plan. They may also be helpful in treating acne scarring. These treatments include comedo extraction, electrocauterisation, chemical peels, microdermabrasion, intralesional corticosteroids, laser treatment, photodynamic therapy and phototherapy (Table).
Biophotonic light therapy is a noninvasive treatment, used especially for inflammatory acne, whereby a gel is applied to the affected area (either face or trunk) and fluorescent light energy applied to stimulate the skin’s repair mechanisms.
Surgical techniques including punch excision, subcision and trichloroacetic acid cross hatching and filler may be used for acne scarring.
Complementary and alternative therapies
Many patients look to ‘more natural’ herbal and alternative treatments. There are limited data on the efficacy and safety of such products, and the specific ingredients, their concentrations and production processes are not well regulated. These alternative therapies include tea tree oil, niacinamide, ayurvedic compounds, antioxidant agents, zinc, probiotic treatments and many types of naturally occurring oils. Dietary modification, biofeedback-assisted relaxation, cognitive imagery and acupuncture have also been tried as alternative therapies to treat acne.
We must remember that patients will often seek treatment advice from non-medical sources and that even when seen by their own doctor, they may not adhere to the medication or attend follow-up appointments. The initial consultation should aim to establish trust between GP and patient and to emphasise the importance of review to see if treatment is working.
Novel treatments
New therapies for acne continue to be developed. Last year, a new fixed dose combination for acne treatment was launched (1% clindamycin phosphate/tretinoin 0.025%), and this year trifarotene 0.005%, a new type of retinoid cream, will likely be available to treat both facial and truncal acne. The newest agents include minocycline foam (currently available in the US) and a topical androgen clascoterone.29,30 These new treatments are not available in Australia at the time of writing.
The role of cannabinoid signalling in skin maintenance and regeneration has prompted investigation of cannabinoids as potential therapeutic targets in acne treatment and includes the topical agent BTX1503, which demonstrated mixed results in a recent phase 2 clinical trial.31,32
Many of these therapies are in various stages of testing, and show promise for future treatments.
Conclusion
Patients with acne need to be assessed for severity of disease as well as for its psychological impact. Listening to patients’ concerns and individualising treatment will help to strengthen the doctor–patient relationship. In a world of ‘fake news’ and so-called experts, healthcare professionals need to rely on their medical expertise and scientific background to offer patients effective treatment. MT